General information
Bronchial asthma is recognized as one of the most common chronic pathologies among school-age children. The number of patients increases every year, which is associated with the deterioration of the environmental situation.
Asthma is a serious and severe pathology, which, if left untreated, is accompanied by the development of complications. The least dangerous are frequent ARVI, chronic rhinitis, sinusitis. But there are also more serious ones. The lack of adequate correction of the disease significantly worsens the patient’s quality of life, leading to impaired physical and mental development and even life-threatening conditions.
The nature of the disease is not fully understood. The pathology is considered multifactorial. Predisposition is determined genetically. In children, bronchial asthma often develops against the background of allergic reactions.
Pathogenesis of bronchial asthma in children
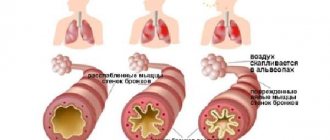
In bronchial asthma, the reaction of the mucous membrane of the bronchial tree to certain conditions (triggers) is disrupted.
These include increased or decreased temperature and humidity, inhalation of allergens (pollen, fur, dust mites), contact with medications and chemicals, physical activity, and stressful situations. As a result, dysfunctional immune inflammation develops in the bronchial mucosa. The epithelial lining swells and produces excessive mucus for protection. However, with bronchial asthma, its thickening occurs, and partial or complete obstruction of the bronchi develops. The situation is aggravated by bronchospasm - contraction of the smooth muscles of the bronchi. As a result, the lumen of the bronchial tree narrows significantly (due to obstruction by mucus and muscle spasm). The patient suffers from bouts of painful coughing and difficulty exhaling air from the lungs (expiratory dyspnea). The volume of oxygen entering the body is sharply reduced, all tissues begin to experience hypoxia (oxygen starvation), as a result of which any biochemical reactions are disrupted.
Causes
The most dangerous provoking factors for the development of bronchial asthma are exogenous allergens, laboratory tests for which confirm a high level of sensitivity in patients with asthma and in individuals who are at risk. The most common allergens are household allergens - house and book dust, aquarium fish food and animal dander, plant allergens and food allergens, which are also called nutritional allergens. In 20-40% of patients with bronchial asthma, a similar reaction to medications is detected, and in 2% the disease was acquired as a result of working in hazardous industries or, for example, in perfume stores.
Infectious factors are also an important link in the etiopathogenesis of bronchial asthma, since microorganisms and their metabolic products can act as allergens, causing sensitization of the body. In addition, constant contact with infection maintains the inflammatory process of the bronchial tree in the active phase, which increases the body's sensitivity to exogenous allergens. The so-called hapten allergens, that is, allergens of non-protein structure, entering the human body and binding to its proteins also provoke allergic attacks and increase the likelihood of asthma. Factors such as hypothermia, family history and stressful conditions also occupy an important place in the etiology of bronchial asthma.
Types of bronchial asthma in children
Depending on the cause of the disease, the following types of bronchial asthma in children are distinguished:
- allergic: attacks are triggered by contact with allergens;
- infectious-dependent: manifests itself against the background of acute respiratory viral infections or bacterial diseases of the respiratory tract;
- mixed: occurs against the background of a combination of several factors.
There is also aspirin-induced asthma. Bronchial asthma, which manifests itself during physical or mental stress, is considered separately.
Depending on the frequency of attacks and their severity, asthma can be mild, moderate or severe.
Factors that cause exacerbation in an asthmatic child
The main “provocateurs” of the disease are opportunistic microorganisms, household and pollen allergens.
The most common triggers in young children are viral and bacterial respiratory tract infections. Exercise can also trigger an attack in a child with uncontrolled asthma. Hyperventilation that occurs during activity causes dryness of the bronchial mucosa, which provokes bronchospasm. Moreover, symptoms can appear either a few minutes after physical effort or many hours later.
Allergic asthma in children worsens after contact with allergens in the air (pollen, house dust). An attack can also be caused by emotions (stress, excitement), weather changes (low temperature combined with high humidity, sunny, windy weather, thunderstorms), certain medications (antibiotics, vitamins), so an asthmatic child should take medications only after consultation with the doctor doctor. Additional irritants (tobacco smoke, polluted air, strong odors) aggravate existing asthma symptoms.
The causes of asthma in children are not precisely known, since the nature of the pathology is not fully understood. Factors that increase the risk of disease:
- hereditary predisposition: the likelihood of developing bronchial asthma is 6.6 times higher in children whose parents suffer from asthma;
- diathesis and other allergic diseases in early childhood. Read more about diathesis on our website Dobrobut.com;
- unfavorable environmental conditions;
- frequent acute respiratory viral infections with complications in the bronchi;
- woman smoking during pregnancy;
- obesity in a child.
Symptoms of bronchial asthma in children
At the initial stage of development, the symptoms of bronchial asthma in children and adolescents may be vague and resemble a cold. However, later the clinical picture becomes more characteristic. The disease manifests itself:
- paroxysmal unproductive cough (at the end of the attack a small amount of mucus is coughed up);
- whistling sounds during inhalation and exhalation;
- shortness of breath (mainly difficult to exhale);
- a feeling of chest compression.
Children with bronchial asthma have a cough with wheezing for a long time. The symptom intensifies during active games, stressful situations (during crying, fear), at night. Seizures occur soon after the baby goes to bed.
After coughing, there is a feeling of lack of air. Breathing becomes more frequent, wheezing appears, chest movements become more noticeable, and it is difficult for the patient to exhale, because it is necessary to suppress strong resistance from the narrowed bronchi. After the attacks, the child is lethargic, apathetic, and drowsy.
Diagnostics and its difficulties
It is more difficult to identify the disease in a child than in an adult. The reason is that children, especially the youngest ones, cannot accurately and correctly describe their condition. In this case, the diagnosis is more difficult, the more moderate the symptoms and discomfort experienced by the patient.
The difficulty is also associated with the structural features of the baby’s bronchi. Until the age of five, they have a narrower opening, and the child’s muscles are generally less developed. Because of this, the main manifestations of the disease are the active discharge of thick sputum and swelling of the mucous membrane, and not suffocation or bronchospasm. Based on this, bronchial asthma is often confused with ARVI and other similar diseases, not only by parents, but also by doctors. The disease often progresses for several years before it is correctly diagnosed.
In general, the following main parameters are important for diagnosing
- presence of symptoms (wheezing, shortness of breath, cough, feeling of lack of air and chest congestion);
- reversibility of attacks;
- excessive activity of the bronchi;
- local inflammatory processes.
In young children it is not always possible to objectively assess all these parameters. Therefore, the greatest attention is paid to:
- collecting anamnesis of the child and his family. Take into account predisposition, frequent cold symptoms, the presence of atopic dermatitis, food allergies, allergic rhinitis;
- analysis of symptoms - their presence and intensity;
- physiological examinations (pulmonary function testing - peak flowmetry, determination of their volume, measurement of the level of bronchial resistance, etc.);
- laboratory tests (in the first two years of life, cough and wheezing are common in children without asthma, so confirmation of the presence of specific antibodies to allergens can be a reason for making a diagnosis of “bronchial asthma”);
- trial treatment for 2-3 months - if there is an improvement against it, and without it there is a new deterioration, this allows us to talk about the presence of asthma;
- Chest X-ray - it does not make it possible to diagnose bronchial asthma, but excludes a number of other similar diseases.
Differential diagnosis is also carried out to exclude diseases accompanied by wheezing: congenital anomalies, infections, mechanical factors, for example, the presence of a foreign body in the bronchi.
An attack of bronchial asthma in a child
A severe attack of bronchial asthma in children is a potentially dangerous condition with specific symptoms that requires immediate help. During an exacerbation it is noted:
- severe difficulty breathing and increased frequency;
- noticeable increase in wheezing;
- child's excitement and anxiety;
- blue lips and nails;
- decreased effect of habitual medications (inhalers).
In this case, an immediate call to the ambulance is required. Depending on the child’s condition, doctors will provide assistance on the spot or hospitalize the little patient.
Causes of bronchial asthma
It is impossible to clearly indicate the exact cause of the development of bronchial asthma in children. Predisposing factors are considered:
- poor heredity (children who have one of the parents with the same diagnosis are more likely to get sick);
- allergic diseases in early childhood;
- obesity;
- maternal smoking while pregnant;
- frequent infectious diseases of the respiratory tract;
- poor ecology (living in big cities, polluted areas);
- unfavorable living conditions (dusty premises, excessive use of household chemicals).
At the moment, food allergies are also considered a predisposing factor. Asthma can be provoked by long-term consumption of foods that stimulate the body's allergenicity (chocolate, spices, additives) against the background of a burdened heredity.
Preventing asthma
There are the following recommendations for prevention:
- Specific and nonspecific immunoprophylaxis.
- Moderate exercise in dust-free areas.
- If there is a genetic predisposition, do not take your child to childcare centers under six years of age.
- If children are prone to food allergies, their diet should consist only of hypoallergenic foods.
- Systematically carry out wet cleaning, eliminate the appearance of mold in the apartment, and use air purifiers in the child’s room.
Diagnosis of bronchial asthma in children
SM-Doctor doctors have extensive experience in diagnosing and treating bronchial asthma in children. With timely detection of the disease and the correct approach to therapy, the number of attacks can be minimized and the patient’s quality of life can be significantly improved. A feature of bronchial asthma in childhood is the possibility of complete recovery. This is due to the fact that the child’s body is constantly and dynamically developing. Therefore, if you create conditions under which the bronchi begin to react normally and the immune system works adequately, then the child will completely get rid of the disease, which will have no place in adult life.
The doctor carefully studies the medical history (including family history), collects complaints, listens to the heart and lungs. Evaluating this information in conjunction with the results of additional examination, the doctor makes a diagnosis and selects the optimal treatment.
The main method for diagnosing bronchial asthma in children is tests to assess external respiratory function. Based on their results, conclusions are drawn about the degree of bronchial obstruction. The examination includes:
- peak flowmetry (measurement of peak velocity during forced expiration);
- spirography (measurement of lung volume);
- pneumotachography (measurement of air exit velocity in the middle of exhalation).
To identify provoking factors, allergic status is determined. Blood and bronchial mucus tests determine the severity of the disease. Chest x-rays are taken to assess the degree of obstruction.
Diagnostics
The diagnosis is usually made by a pulmonologist based on complaints and the presence of characteristic symptoms. All other research methods are aimed at establishing the severity and etiology of the disease. On percussion, the sound is clear and boxy due to the hyperairiness of the lungs, the mobility of the lungs is sharply limited, and their boundaries are shifted downward. On auscultation over the lungs, vesicular breathing is heard, weakened with prolonged exhalation and with a large number of dry wheezing rales. Due to the increase in lung volume, the point of absolute dullness of the heart decreases, the heart sounds are muffled with an accent of the second tone above the pulmonary artery. Instrumental studies include:
- Spirometry. Spirography helps to assess the degree of bronchial obstruction, determine the variability and reversibility of obstruction, and also confirm the diagnosis. In asthma, forced exhalation after inhalation of a bronchodilator increases by 12% (200 ml) or more in 1 second. But to obtain more accurate information, spirometry should be performed several times.
- Peak flowmetry. Measuring peak expiratory activity (PEA) allows you to monitor the patient's condition by comparing the indicators with previously obtained ones. An increase in PEF after inhalation of a bronchodilator by 20% or more from PEF before inhalation clearly indicates the presence of bronchial asthma.
Additional diagnostics include allergen tests, ECG, bronchoscopy and chest x-ray. Laboratory blood tests are of great importance in confirming the allergic nature of bronchial asthma, as well as for monitoring the effectiveness of treatment.
- Blood test. Changes in the CBC - eosinophilia and a slight increase in ESR - are determined only during an exacerbation. Assessment of blood gas composition is necessary during an attack to assess the severity of DN. A biochemical blood test is not the main diagnostic method, since the changes are of a general nature and such studies are prescribed to monitor the patient’s condition during an exacerbation.
- General sputum analysis. Microscopy in sputum can reveal a large number of eosinophils, Charcot-Leyden crystals (brilliant transparent crystals formed after the destruction of eosinophils and shaped like rhombuses or octahedrons), Courshman spirals (formed due to small spastic contractions of the bronchi and look like casts of transparent mucus in the form spirals). Neutral leukocytes can be found in patients with infection-dependent bronchial asthma in the stage of active inflammatory process. The release of Creole bodies during an attack was also noted - these are round formations consisting of epithelial cells.
- Study of immune status. In bronchial asthma, the number and activity of T-suppressors sharply decreases, and the amount of immunoglobulins in the blood increases. The use of tests to determine the amount of immunoglobulin E is important if allergy tests are not possible.
Treatment of bronchial asthma in children
The goal of therapy is to effectively control the disease, which will provide the child with the opportunity to live a full life (play sports, develop properly mentally and physically).
With the right treatment, symptoms can be completely controlled and complications can be prevented. In the treatment of bronchial asthma in children, an integrated approach is used, based on the cause and stage of the disease, severity of symptoms, frequency of attacks, age of the child, and concomitant diseases. The program is based on eliminating factors that provoke an attack (allergens, stress, overexertion, etc.). Taking into account the form of the disease, medications are prescribed that eliminate inflammation in the bronchi, normalize the secretion and removal of mucus, and reduce the reactivity of the bronchi. Separately, drugs are selected for emergency relief of attacks, which relieve bronchospasm and restore lung ventilation.
Treatment of any diseases (flu, ARVI, colds and even headaches) in a child with bronchial asthma should be carried out under the supervision of a doctor.
Classification
Asthma is divided according to etiology, severity, level of control and other parameters. Based on their origin, they distinguish allergic (including occupational BA), non-allergic (including aspirin BA), unspecified, mixed bronchial asthma. Depending on the severity, the following forms of asthma are distinguished:
- Intermittent (episodic). Symptoms occur less than once a week, exacerbations are rare and short.
- Persistent (constant). Divided into 3 degrees:
- mild - symptoms occur from 1 time per week to 1 time per month
- average - frequency of attacks daily
- severe - symptoms persist almost constantly.
During the course of asthma, there are exacerbations and remission (unstable or stable). If it is possible to control attacks, asthma can be controlled, partially controlled and uncontrolled. A complete diagnosis of a patient with bronchial asthma includes all of the above characteristics. For example, “Bronchial asthma of non-allergic origin, intermittent, controlled, in the stage of stable remission.”
Complications of bronchial asthma in children
Without daily monitoring and careful use of medications, asthma can cause severe complications, some of which are life-threatening:
- status asthmaticus (a condition in which an attack does not go away with standard care);
- infectious diseases of the respiratory tract;
- emphysema;
- bronchiectasis (dilation of the terminal sections of the bronchi);
- pneumothorax (damage to the membrane covering the lungs with air escaping into the pleural cavity);
- pathology of the heart and blood vessels, etc.
Forecast and prevention of bronchial asthma in children
Bronchial asthma is a chronic disease that lasts a lifetime in 2 out of 3 affected children.
After puberty, symptoms may increase or decrease. The quality of life largely depends on correctly selected treatment and preventive measures. It is important for parents to know the signs of exacerbation of bronchial asthma in their child and take timely measures to stop it. Preventive measures are relevant for children prone to allergies, as well as whose close relatives suffer from asthma. Such activities must be carried out from birth. To prevent bronchial asthma you should:
- feed the newborn with breast milk for as long as possible;
- introduce complementary foods correctly;
- avoid foods that may cause allergies (honey, chocolate, nuts);
- treat colds and infectious diseases in a timely manner and under the supervision of a pediatrician;
- minimize contact with household allergens (chemicals, dust, animal hair);
- use pillows and blankets with hypoallergenic fillings;
- refuse any interior items that accumulate dust (carpets, heavy curtains);
- regularly ventilate the house and do wet cleaning;
- create a favorable psychological environment in the family.
The most effective measures are aimed at generally strengthening the body and stimulating the immune system. These include an active lifestyle, good nutrition, daily walks in the fresh air, and hardening.
SM-Doctor employs qualified pediatric pulmonologists, allergists and immunologists. Specialists will assess the child’s condition in detail, make an individual prognosis for bronchial asthma and, upon objective diagnosis of the disease, prescribe targeted treatment. Contact the best doctors who will help your child breathe deeply, grow and develop correctly!