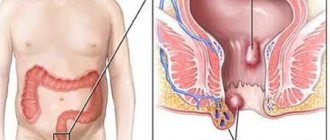
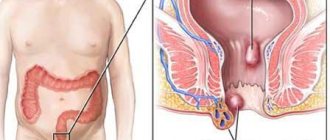
External hemorrhoids
- a pathological proctological condition characterized by varicose veins of the external venous hemorrhoidal plexus. It is manifested by a wide range of unpleasant sensations, including a sensation of itching and burning in the anus, aggravated by prolonged standing, sitting, during or after bowel movements.
According to medical statistics, hemorrhoids are one of the most widespread diseases. According to various sources, it affects up to 10% to 80% of the world's population. Proctologists distinguish between external and internal hemorrhoids. The former accounts for 35 to 40 percent of the total number of diagnoses, with male patients suffering from hemorrhoids much more often. It is diagnosed in 80% of cases in men aged thirty to sixty years.
Etiology of external hemorrhoids
The main initiating factor of external hemorrhoids is the disruption of the outflow from the blood veins of the external hemorrhoidal zone due to congenital or acquired anomalies of the venous walls. This leads to its stagnation, enlargement of the cavernous bodies, the development of their pathological changes, and with serious expansion - loss from the muscular basket, displacement to the anus and protrusion under the skin in the corresponding area. Factors that provoke this condition include the following:
- The need to tense the muscles of the perineum, accompanied by an increase in pressure in the hemorrhoids with systematic stool disorders in the form of constipation and prolonged diarrhea, during pregnancy or with birth injuries;
- Lack of sufficient physical activity, lack of exercise, working in a sitting or standing position, lifting heavy weights, consuming food that irritates the intestinal mucosa;
- Compression of the intestines by the uterus increasing as the fetus grows.
Symptoms of hemorrhoids
External hemorrhoids of the anus
characterized by pathological changes in the muscular-ligamentous structures of the anus and the final part of the rectum. Due to the weakening of collagen fibers, hemorrhoids protrude even more, the number of arteries and their branches increases, which increases blood flow. Thus, due to the obstructed outflow, it accumulates even more, so the walls of the hemorrhoids stretch even more.
| Symptoms of external hemorrhoids | |
| Symptom | Features of manifestation |
| Pain | External hemorrhoids manifest themselves as painful symptoms, localized in the anus and appearing after prolonged standing or sitting, after physical exertion, as well as during coughing or sneezing. The pain can vary in intensity: from mild to unbearable. |
| Uncomfortable sensations | The external lump of hemorrhoids may manifest itself as severe itching or burning, localized in the anus. |
| Bleeding | They occur quite rarely and are characterized by a minimal volume of lost blood. Extremely rarely, it can appear on feces, mainly on linen or toilet paper. |
| Feeling of a foreign body | If the nodes have a large diameter, the patient can not only feel them on his own, but will also experience unpleasant sensations of a foreign body in the anal area. Inflamed hemorrhoids can cause increased pain and even an increase in overall body temperature. |
Removal of anal fimbriae
Another important problem that many patients (most often women) treat is anal fimbria. They ask to remove them. What are these fringes? This is the “extra” skin that appears at the edge of the anus. It always gets in the way, causes aesthetic problems, and often becomes inflamed and grows.
Anal fimbria are always associated with diseases of the anal canal: hemorrhoids, inflammation of the canal - sphincteritis, anal fissures. Without eliminating these causes, removing fringes is pointless and sometimes harmful. They will then grow again. Dear patients, remember this when you insist on removing fimbriae!
Complications of external hemorrhoids
If treatment of external hemorrhoids
is not carried out, it can become complicated, manifesting itself as inflammatory processes of cavernous bodies and thrombosis of the blood veins. In the first case, there are three stages of inflammation of hemorrhoids:
- The first is characterized by increased pain, itching and burning, especially after bowel movements or consumption of foods that irritate the intestinal mucosa. An examination by a proctologist reveals a dense, slightly swollen nodule;
- The second is manifested by an increase in the above symptoms, redness of the skin around hemorrhoids, increased swelling and the inability to palpate due to severe pain;
- The third differs in that the inflammation covers the subcutaneous tissue and adjacent tissues. The skin on inflamed hemorrhoids becomes burgundy and has a bluish tint. Under it you can feel the infiltrate, inside of which there is a dense formation. Sometimes necrotic areas are found.
As for thrombosis, it covers one of the nodes and manifests itself with sudden pain symptoms after bowel movement or occurring suddenly. During the examination, the specialist discovers a bluish nodule with swelling.
Symptoms of anal fissure
An anal fissure is treated with medications only at the beginning of its occurrence - about a month. At this time, the doctor will diagnose you with “Acute anal fissure”. If it has not healed during this time, the chances of success of conservative treatment are greatly reduced. Scar tissue always forms around the crack, and the longer it exists, the rougher and more massive these scars become. The crack becomes chronic. It was necessary to treat patients whose scars along the edges of the cracks were more than half a centimeter. At this stage of existence there is pain, often severe. The pain is associated with the process of bowel movement and can last for several hours. A chronic fissure is always accompanied by a spasm of the sphincter, the muscle that compresses the anus. The spasm further intensifies the pain. Over time, sentinel tubercles appear - skin growths at the inner and outer edges of the fissure (internal sentinel tubercles are sometimes mistakenly called anal polyps).
Here are the attributes of a chronic anal fissure:
- pain,
- spasm,
- scarring,
- sentinel tubercles.
The time it takes for an acute crack to become chronic can vary from one month to six months. There are also intermediate stages of the disease. For chronic anal fissure, the use of medications has almost no effect. The time for medical manipulation is coming. They can be carried out either on an outpatient basis (there are appropriate treatment methods) or on an inpatient basis - classic operations for excision of anal fissures. Further treatment after the manipulations is prescribed by the doctor.
Of course, all diseases of the anus cannot be considered in one article. I hope to write a series of articles devoted to various diseases in proctology. I have already mentioned inflammatory processes in the anal canal. Inflammation of the structures of the anal canal (anodermis, anal papillae, anal glands) almost always occurs against the background of existing hemorrhoidal disease. It is rare to do without hemorrhoids in this matter. And these diseases must be treated together, sometimes in turn. But if hemorrhoids are left unattended, relapses of inflammation very often occur. Hemorrhoids progress over time and cause additional suffering.
Diagnosis of external hemorrhoids
Diagnosis of hemorrhoids, in fact, is not difficult in any way and can be carried out during an external examination of the patient. The doctor identifies specific lumps localized around the anus. They are palpable only under the skin or bulge outward, forming lumps. Their bluish tint indicates the presence of thrombosis. Further diagnostic studies are aimed at clarifying the primary conclusion and identifying associated pathological conditions. They provide the following:
- Complete blood count - to identify inflammatory processes of hemorrhoids;
- Sigmoidoscopy - to exclude internal hemorrhoids with their prolapse, polyps and neoplasms of malignant etiology;
- Colonoscopy - to obtain more accurate information if rectoscopy did not provide it;
- Angiography - to identify the source of hemorrhage, if any;
- Ultrasound scanning of the rectum - for the best visualization of pathological changes in the cavernous bodies and veins.
External hemorrhoids must be differentiated from prolapsed internal hemorrhoids, prolapse of the rectum, its polyps or neoplasms of any nature.
How to treat external hemorrhoids?
The treatment tactics are chosen by the attending physician, guided by the patient’s individual indications and the results of diagnostic studies. Unfortunately, conservative therapy cannot provide a complete cure, but it can eliminate all the unpleasant symptoms of hemorrhoids: swelling, pain, discomfort. Patients should eat in accordance with the diet selected by the doctor, move more and avoid lifting heavy objects.
The best results for external hemorrhoids are obtained by removing the nodes: thanks to it, you can eliminate this unpleasant problem for a very long time and even forever. The operation is performed under local anesthesia and does not require the patient to remain in the hospital. Various techniques are used in the process:
| Methodology | Description |
| Hemorrhoidectomy | Radical excision, indicated in advanced stages of hemorrhoids with large nodes. Aimed at their removal by stitching the leg. Requires general anesthesia and is characterized by a minimal risk of complications. |
| Latex ligation | A minimally invasive procedure that involves placing a latex ligature on the hemorrhoid stem in order to compress the blood vessels feeding the node and stimulate its death. |
| Photocoagulation | The process uses a focused infrared beam, with which the doctor cauterizes the hemorrhoidal node, which provokes disruption of its blood supply and subsequent atrophy. |
If a patient has thrombosis, he is prescribed thrombolytics (at an early stage) or anticoagulants. If drug therapy does not give the desired result, the blood clot is removed through surgery. It involves making an incision on the node and removing the clot.
Modern methods of treating hemorrhoids
Etiology
Hemorrhoids (from the Greek haimorrois) literally mean “bleeding.” This disease, known since time immemorial, is still explained ambiguously and sometimes contradictorily, which fully reflects the level of our knowledge about it. Most researchers recognize that the sources of bleeding are cavernous formations, which under normal conditions are formed during intrauterine development.
The first group of hemorrhoidal formations, the defeat of which leads to the formation of external hemorrhoids, is located at the exit from the anal canal, in the subcutaneous tissue.
The second group of cavernous formations, located in the submucosal layer of the rectum, above the dentate line, is the source of the development of internal hemorrhoids.
There are anastomoses between the external and internal cavernous formations, the functional purpose of which is not entirely clear, if only because with an increase in intra-abdominal pressure, as a rule, external rather than internal nodes thrombose. Along with the external and internal sphincter, the cavernous plexuses are part of the obturator apparatus of the rectum. Their ability to increase in volume due to filling with blood allows for an ideal sealing of the intestine. Indirect evidence of this assumption is the ordered arrangement of hemorrhoidal formations around the circumference of the intestine; it corresponds to 3, 7 and 11 o'clock. Unfortunately, this delicate mechanism is very vulnerable and there are many reasons for this. The immediate cause of hemorrhoids is a violation of the blood supply to the cavernous veins, which can be caused by increased arterial blood flow, but more often by a slowdown in venous outflow. The dilated vein forms a “bag of blood”, which is called a hemorrhoid. In recent years, much attention has been paid to studying the condition of the ligamentous apparatus of the submucosal layer of the rectum, the violation of which leads to the prolapse of internal hemorrhoids. Therefore, from the point of view of modern pathophysiology, both variants of the development of the disease should be considered not only as equivalent, but, possibly, as complementary.
Prevalence . Data on the prevalence of hemorrhoids are very contradictory; for example, in Russia this figure ranges from 130–145 cases per 1000 adults [1]. Statistical data provided by foreign researchers is only about 4.4% [2, 3]. The inconsistency of the indicators is most likely due to the difference between morbidity and negotiability, which is indirectly confirmed by data from examinations of US residents, which stated that 80% of people who had hemorrhoids did not complain [4].
Classification of hemorrhoids . The classification was proposed by the State Scientific Center of Coloproctology [1]. It includes the symptoms of the disease, its clinical manifestations and anatomical changes. According to the course of the disease, chronic and acute types of hemorrhoids are distinguished. In shape - internal, external, combined. The chronic course of internal hemorrhoids is divided into 4 stages. It should be emphasized that the clinical symptoms of the disease correspond to the morphological changes occurring in the longitudinal muscle, which fixes cavernous formations in the submucosal layer of the rectum.
In the first stage: bleeding and discomfort are clinically noted, hemorrhoids do not fall out of the anal canal, the vascular pattern of the mucous membrane is enhanced, anatomically - changes in the longitudinal muscle are insignificant.
In the second - bleeding, prolapse of nodes, itching, mucous discharge; prolapsed nodes are automatically reset into the anal canal; histologically in the fibromuscular framework there is unexpressed dystrophy, the number of elastic fibers predominates.
In the third - bleeding, prolapse of nodes, anal itching, mucous discharge. Prolapsed hemorrhoids require manual assistance to reposition them into the anal canal; At the same time, morphological changes in muscle tissue indicate a loss of elasticity, which proves the predominance of dystrophy processes.
In the fourth - bleeding, itching, discomfort, incontinence of the anal sphincter, severe pain; constant prolapse and inability to manually reduce hemorrhoids into the anal canal; which corresponds to complete degeneration of the fibromuscular framework that holds the nodes in the anal canal.
Complications of hemorrhoids . The most common complication of hemorrhoids is thrombosis of hemorrhoids. As a rule, the lesion occurs in the external nodes and quite often thrombosis is the first manifestation of the disease. Precipitating moments for the development of thrombosis most often include pregnancy, childbirth, long air travel, lifting heavy weights, and acute stool disorders. If patients seek help in the first 2 days from the onset of the disease, an enlarged bluish (at an early stage) hemorrhoid, covered with skin and partially mucous, is easily visually detected. More often, the appearance of a node is accompanied by pain, especially intense if two or more nodes are affected. If the size of the node is significant (usually more than 2 cm) with pronounced tension in the mucosal tissue, an area of necrosis appears on it; after rejection of the latter, bleeding develops, sometimes parts of the blood clot may partially come off and the size of the prolapsed formation may decrease significantly. The skin part of the node becomes swollen and hyperemic. Clinically, as a rule, in this case, the patient notes a decrease in pain. Digital examination should begin with examination of the wall of the anal canal opposite to the thrombosed node, which makes the examination more gentle. A digital examination can reveal signs of thrombosis of the internal hemorrhoid. Examination of the anal canal using instruments is carried out only by proctologists.
More rare complications include the formation of a hematoma with a sharp increase in pressure and damage to the wall of the venous vessel. If an internal hemorrhoid prolapses, it may become strangulated. If necrosis of the internal node occurs, massive bleeding is possible, so the patient should be shown to a proctologist. In the event of strangulation of several prolapsed nodes or the occurrence of stool disorders, a purulent process may occur in the perirectal tissue.
Differential diagnosis
Clinical manifestations of hemorrhoids do not differ in the specificity of symptoms. In case of acute hemorrhoids or its complications, these are acute paraproctitis, anal fissure, cryptitis, rectal prolapse. In the case of chronic hemorrhoids, the development of a tumor of the rectum or anal canal should first be excluded. The group of patients who have been suffering from hemorrhoids for a long time, who have come to us due to increased bleeding or unstable stools, is of particular concern in terms of oncological diseases. In case of any treatment of a patient with hemorrhoids to a therapist or general practitioner, it is necessary to refer him for a consultation with a proctologist.
Conservative treatment
The choice of treatment method is usually determined by the stage of the disease or the nature of the complications that have developed.
A special diet for patients with hemorrhoids is not required, except in certain cases. For thrombosis of hemorrhoids, a protein-vegetable diet with a high fiber content and the exclusion of fried and spicy foods, spices, and alcohol is recommended. In patients with concomitant diseases of the colon (irritable bowel syndrome, diverticular disease or nonspecific colitis), the diet should be aimed at normalizing stool. In case of thrombosis of hemorrhoids, accompanied by constipation, patients should be prescribed microenemas to cleanse the intestines. Patients leading a sedentary lifestyle, without exacerbation, should be recommended to play sports, with the exception of weightlifting and cycling. Patients should pay special attention to performing hygienic measures. During the acute period of the disease, it should be recommended to take a cool shower 2-3 times a day and always after stool, and it is necessary to wash not only the skin of the perineum and anus, but also the anal canal itself. In cases where water procedures are not available, the use of special wet sanitary napkins should be recommended.
Systemic drugs . In the conservative treatment of hemorrhoids, one of the leading roles belongs to drugs containing bioflavonoids (diosmin and hesperidin). The use of the latter in the treatment of hemorrhoids is traditional, but with the creation of modern biotechnologies it was possible to obtain Detralex, a micronized drug, which made it more bioavailable and increased the effectiveness of treatment by about 30%. Bioflavonoids have several properties: first of all, they are able to increase venous tone, enhance lymphatic drainage, reduce vascular fragility and improve microcirculation. First of all, the listed qualities make it necessary to use Detralex in the event of thrombosis of hemorrhoids. The drug is prescribed 2 tablets 3 times a day for the first four days, then 1 tablet 4 times for up to 7 days. In addition, Detralex is able to reduce and prevent the development of hemorrhoidal bleeding and exacerbation of hemorrhoids. For preventive purposes, it is recommended to take the drug for up to 6 months, 2 tablets per day. The use of micronized bioflavonoids (the source of which are natural sources, for example, red grape seeds) is possible even during pregnancy, although not for a long time (up to 7 days). The drug is well tolerated and rarely causes allergic reactions. To date, the drug “Phlebodia 600” has been successfully used, which has a prolonged effect, which allows it to be taken once a day. In patients with thrombosis of hemorrhoids, accompanied by severe pain, it is possible to use non-steroidal anti-inflammatory drugs and analgesics, but it is extremely difficult to assess the effectiveness of their effects, so the question of their use should be decided individually in each specific case.
Local therapy . Local treatment is prescribed to relieve inflammation and analgesia. Among the drugs of the first group, we can recommend Posterisan Forte ointment (or suppositories of a similar name). The drug contains a suspension of E. coli culture and hydrocortisone. E. coli metabolites can enhance local immune responses, accompanied by the release of cytokines, especially intraleukin-1. In addition, a suspension of bacterial culture causes the formation of specific immunoglobulin A, which forms a delicate film on the intestinal mucosa, acting as a local protective barrier. Hydrocortisone, which is the second component of the drug, helps to quickly suppress inflammation and accelerates the processes of tissue regeneration induced by a suspension of Escherichia coli culture. The drug is administered rectally 2 times a day; in case of severe inflammatory process, for example, in patients with nonspecific colitis, the frequency of administration can be increased taking into account the frequency of stool. The maximum duration of treatment does not exceed three weeks. If it is necessary to continue therapy, it is possible to use Posterizan suppositories or ointments containing exclusively a suspension of bacterial culture.
Among the drugs that have a complex effect, we recommend Relief Advance suppositories. The composition includes 10% benzocaine, which has a rapid analgesic effect, in addition, shark liver oil containing fat-soluble vitamins, free fatty acids, squalene and alkylglycerol, which are powerful reparants, which allows them to be recommended even for use in the postoperative period in patients who underwent surgery for hemorrhoids. The frequency of administration is 3–5 times a day. The drug is highly effective, well tolerated and rarely produces adverse reactions.
Surgical treatment of hemorrhoids
External hemorrhoids . In addition to conservative treatment of thrombosed hemorrhoids in the first 24–48 hours, until inflammatory changes in the skin part of the node occur, surgical intervention is possible. It is usually performed under local anesthesia and involves removing the hematoma or thrombotic masses, although there is an opinion that it is necessary to remove the entire node along with the affected vein [5]. This tactic is justified in the presence of one (less often two) large nodes or in severe pain. Unfortunately, such operations can not be performed often, because the majority of patients consult a doctor already in the presence of severe inflammation, which sharply intensifies the pain syndrome that existed until that moment. Surgical removal of large external nodes is justified in case of difficulties arising with hygiene, persistent anal itching or after previous thrombosis, although in recent years many patients have turned to a proctologist for aesthetic reasons.
Internal hemorrhoids . Currently, there is a fairly large selection of minimally invasive treatments, used mainly for isolated internal hemorrhoids of stages I–II. True, sometimes the indications for their use can be expanded, mainly in elderly and senile people with severe concomitant diseases. Minimally invasive interventions include: infrared photocoagulation, latex ring ligation and, finally, transanal ligation under Doppler control. The first two of these methods have long been used in clinical practice, and their strengths and weaknesses are well known, so we will dwell in more detail on the last method.
Ligation of hemorrhoidal arteries under Doppler control . The essence of the method is based on the fact that Doppler examination reveals the distal branches of the superior hemorrhoidal artery, supplying blood to the internal hemorrhoids. The necessary equipment is an electronic unit and an anoscope with a Doppler sensor. The method can be used for stages I–III of the disease. The procedure can be carried out in a hospital within one day. The procedure lasts 20–40 minutes, does not require general anesthesia, restrictions on physical activity for about two weeks. Temporary disability is not required for patients. There are no problems with stool in the early postoperative period.
Operation Longo . Prolapse of the mucous membrane of the anal canal with internal hemorrhoidal plexuses, caused by damage to the muscular and ligamentous apparatus of the latter, is accompanied by a disruption of their blood supply and a change in the anatomical relationships between the external and internal nodes. This prerequisite served as the basis for the creation of the Longo operation, which involves tightening the prolapsed mucosa, restoring the anatomical position of the hemorrhoidal plexuses and normalizing their blood flow. The Longo method has been used in clinical practice since 1993, in our country for the last 5 years. The intervention is performed with a disposable set of instruments. The operation is indicated for stages II–IV of hemorrhoids. In our opinion, the advantages of this procedure are most convincing for circular prolapse of nodes. The operation can be performed under conduction or local anesthesia.
Advantages of the method; the duration of the operation is 10–20 minutes, the hospitalization period does not exceed one day, the pain syndrome is well relieved without the use of narcotic analgesics, there is no need for dressings, the patient can return to work in 5–10 days.
Bipolar coagulation of hemorrhoids using the LigaSure device . A modern alternative to classical hemorrhoidectomy is the method of bipolar coagulation of hemorrhoids, which is successfully used in stages III–IV of the disease. The method is based on the principle of bipolar coagulation using a modernized generator equipped with a feedback unit that allows tissue differentiation. In this case, the usual burn of the tissue does not occur, but welding occurs due to the polymerization of its own collagen and instead of the usual scab, the wound is covered with a collagen film. The intervention can be performed under spinal or epidural anesthesia. The intervention technique is simple. The reliability of polymerization guaranteed by the method makes it possible to coagulate vessels up to 7 mm in diameter. The duration of the operation is about 20 minutes. The duration of postoperative treatment is determined by the size of the wound defects of the anal canal. Pain syndrome in the postoperative period is less pronounced than during traditional surgery.
Literature
- Vorobyov G.I., Shelygin Yu.A., Blagodarny L.A. Hemorrhoids. M.: Publishing house "Mitra-Press", 2002. 192 p.
- Johanson JF, Sonnenberg A. The prevalence of hemmhoroids and chronic constipation // Gastroenterology. 1990, 98; 380–386.
- Bayer I., Myslovaty B., Picovsky BM Rubber Band ligation of hemorrhoids: covenient and economic treatment // J. Clin. Gastroentrol. 1966; 23:50–52.
- Haas PA, Haas GP, Schmaltz S., Fox TA Jr. The prevalence of hemorrhoids // Dis. Colon Rectum. 1983; 29: 435–439.
- Corman MI Colon and Rectum surgery, 3rd ed.Philadelphia, Pa: JB Lippincott. 1993: 54–115.
K. E. Mayat , Candidate of Medical Sciences European Medical Center , Moscow
Prognosis of external hemorrhoids
With timely diagnosis and treatment of external hemorrhoids, the prognosis is favorable. The disease will proceed latently, without creating discomfort or reducing the patient’s quality of life. Vein thrombosis is a serious problem: treatment in this case must be started immediately, otherwise complications cannot be avoided.
The Doctor Nearby network of clinics invites you to undergo diagnostics and treatment for hemorrhoids in Moscow. Our clinics are equipped with the latest technology and have a powerful diagnostic base that allows us to accurately diagnose and develop treatment tactics. We employ highly qualified proctologists with many years of practical experience. They know how to cure hemorrhoids and return the taste of life to the patient.
You can make an appointment with our specialists by filling out and sending us the online form presented on the website, or by contacting our operators!