- Etiology and pathogenesis
- Classification of tonsillitis Clinical forms of vulgar tonsillitis
- Treatment of vulgar tonsillitis.
As a disease of the pharynx, sore throat has been known since ancient times.
Sore throat is described in the works of Hippocrates (IV–V century BC), Celsus (I century AD), and also in the manuscripts of the Tajik physician Abu Ali Ibn Sina (Avicenna, 11th century) mention of intubation and tracheotomy for asphyxia due to tonsillitis, etc. Sore throat is a common acute infectious disease in which local inflammation affects the lymphadenoid tissue of various tonsils of the pharynx. In the vast majority of cases, tonsillitis occurs in the palatine tonsils, while other tonsils are involved in the process much less frequently. Angina is not a homogeneous disease; it differs in etiology, pathogenesis and form of clinical course.
General overview
Follicular tonsillitis (according to ICD 10: code J 03) is one of the four forms of acute tonsillitis (from the Latin tonsillae - tonsil).
Catarrhal tonsillitis is the mildest course of the disease, in which the palatine tonsils are enlarged, full of blood, but there is no purulent discharge on them, and the patient’s general well-being suffers slightly. The risk of complications is minimal.
Catarrhal sore throat photo
Follicular - “islands” of white purulent discharge are noted on enlarged tonsils; they are easily removed during examination by an ENT doctor. Lacunar - “islands” merge into dense yellowish deposits covering the tonsils in the form of “rivulets”.
Follicular sore throat photo
Membranous-necrotic - purulent plaques form dense films covering not only the tonsils, but also the surrounding tissues of the oropharynx.
Membranous necrotic sore throat photo
As the manifestations of the disease increase, the patient’s state of health worsens to severe, and the risk of immediate and delayed complications increases.
General information about the disease
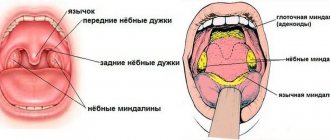
With this type of sore throat, inflammation of the follicles of the palatine tonsils occurs. A follicle is a collection of lymphatic cells that look like small tubercles. It is in them that the protective cells of the immune system - leukocytes - are produced.
The main function of the palatine tonsils is to protect the body of any person, both adults and children, from infection entering the lower respiratory tract. The tonsils are an organ of the immune system. As soon as contact occurs between pathogenic microorganisms and the surface of the tonsil, the follicles begin to intensively produce leukocytes, which are sent to fight the enemy agent. As soon as the enemy is defeated, the dead bacteria, along with the dead leukocytes, are eliminated from the body. But if, for a number of reasons, the immune system is weakened, the tonsils cease to fully perform their functions. The inflammatory process spreads to the palatine tonsils.
If inflammation affects the lacunae of the tonsils, we talk about lacunar angina, if the follicles of the tonsils - about follicular angina, respectively.
Etiological factors
Follicular tonsillitis in children and adults can be caused by various microbial pathogens:
- viruses: adeno-, rhino-, boca-, metapneumoviruses, Epstein-Barr, parainfluenza, etc.;
- bacteria: beta-hemolytic streptococcus of group A (less often - other serogroups), Staphylococcus aureus, Pfeiffer bacillus, Moraxella, pneumococcus, corynebacteria, Neisseria, etc.,
- fungal agents.
What is important is a decrease in the overall resistance of the body against the background of overwork, hypothermia, malnutrition, and advanced chronic diseases.
While viral tonsillitis is more common in children, bacterial pathogens predominate among adults. Group A beta-hemolytic streptococcus is of greatest clinical importance. It causes about 35% of all tonsillitis in children and up to 80% in adults. It is this microorganism that “triggers” autoimmune long-term complications of the disease - acute rheumatic fever, rheumatic heart disease, glomerulonephritis, arthritis.
Causes of the disease
The causative agents of the follicular variety of the disease are most often streptococci, less often - staphylococci, fungi and viral infections.
It is quite easy to become infected with tonsillitis, because it is a highly contagious disease. Sources of infection can be either external (the infection entered the body from the outside) or internal (the source of infection was already present in the body, and when exposed to certain factors, microorganisms became active and caused an exacerbation).
Adults and children can become infected in several ways: through contact with a sick person when he coughs or sneezes; consuming contaminated food or water; when using the patient’s personal items (towel, toys, dishes, etc.).
Inflammation of the tonsils is usually preceded by certain factors that reduce immunity:
- the presence of chronic foci of inflammation in the body (for example, chronic sinusitis);
- carious teeth and other dental problems;
- hypothermia;
- stress;
- poor nutrition and bad habits;
- working or living in unfavorable conditions.
It is generally accepted that children are more likely to get tonsillitis when they are constantly in a closed community (kindergarten, school), but it is also quite easy for adults to become infected at work or in transport.
The incubation period of the disease ranges from several hours to seven days. The inflammatory process first covers the mucous membrane of the tonsils (catarrhal form of the disease), then it moves to the follicles (follicular form). If you begin to treat the disease promptly and correctly, acute tonsillitis lasts a week to a week and a half, then the symptoms of the disease disappear.
In order to contact an ENT doctor in time to prescribe effective treatment, every adult needs to know the main signs of the disease.
Clinical manifestations
Signs of follicular tonsillitis:
- acute onset;
- high fever up to 38-40C, low-grade fever is less common;
- severe sore throat up to refusal to eat and drink, difficulty swallowing saliva, sometimes there is soreness in the cervical lymph nodes and ear;
- intoxication - weakness, headache, feeling of exhaustion, excessive sweating.
In children, sore throat is especially severe. At the height of the fever, moodiness and irritability are noted, sleep becomes shallow and intermittent, and the amount of urine excreted sharply decreases. Dyspeptic symptoms may occur - nausea, vomiting, abdominal pain, increased gas formation in the intestines, and loosening of the stool. There is involvement of the meninges - severe headaches, convulsions, impaired consciousness.
Sometimes general symptoms appear first - a rise in temperature and a deterioration in the general condition, and only on the 2-3rd day of illness does a characteristic sore throat appear.
Classification of sore throats
In practice, the classification of B.S. is most widespread. Preobrazhensky, based on pharyngoscopic signs, supplemented by data obtained during laboratory research, sometimes with information of an etiological or pathogenetic nature.
This classification includes the following forms of sore throat: I - catarrhal, II - follicular, III - lacunar, IV - fibrinous, V - herpetic, VI - phlegmonous (intratonsillar abscess), VII - ulcerative-necrotic (ganrenous), VIII - mixed forms.
To this main diagnosis, after obtaining the appropriate data, the name of the microbe that caused the sore throat (streptococcal, staphylococcal, etc.) or other characteristic features (traumatic, toxic, monocytic, etc.) can be added.
It is customary among clinicians to divide all existing sore throats into vulgar (or banal) and atypical.
Vulgar tonsillitis is characterized by the presence of four general signs: (1) there are severe symptoms of general intoxication of the body; (2) there are pathological changes in both tonsils; (3) the duration of vulgar sore throat does not exceed 7 days (1 week); (4) the primary factor in the etiology of these sore throats is a bacterial or viral infection.
Clinical forms of vulgar tonsillitis
Among a large group of sore throats, the most common are vulgar (ordinary, banal) sore throats, which arise in connection with the introduction of one or another microbial or viral infection. These sore throats are recognized mainly by pharyngoscopic signs. These include catarrhal, lacunar, follicular, fibrinous and phlegmonous (intratonsillar abscess). The most common forms are:
Catarrhal sore throat.
The disease begins acutely, with burning sensations, dryness, soreness in the throat, and then slight pain when swallowing. I am concerned about general malaise, weakness, headache. Body temperature is usually low-grade; There are slight inflammatory changes in the peripheral blood. Faringoscopically, diffuse hyperemia of the tonsils and the edges of the palatine arches is determined; the tonsils are somewhat swollen. The tongue is dry and coated. There is often a slight enlargement of regional lymph nodes. In rare cases, catarrhal tonsillitis is more severe. In childhood, clinical phenomena are more pronounced than in adults. Usually the illness lasts 3–5 days.
Follicular tonsillitis.
It is characterized by predominant damage to the parenchyma of the tonsils and their follicular apparatus. Like lacunar, follicular tonsillitis begins with sudden chills with an increase in body temperature to 40°C, severe sore throat. The phenomena of intoxication are pronounced. Patients are concerned about severe general weakness, headache, pain in the heart, joints and muscles. Sometimes dyspepsia and oliguria are observed. The palatine tonsils are hyperemic and sharply swollen. Follicles in the form of whitish-yellowish formations the size of a pinhead are visible through the epithelial cover. The surface of the tonsil, in the figurative expression of N.P. Simanovsky, takes on the appearance of a “starry sky”. Regional lymphadenitis is pronounced.
Lacunar tonsillitis.
The onset of the disease and its general symptoms are the same as with follicular tonsillitis. More often, lacunar tonsillitis is more severe than follicular tonsillitis. The pharyngoscopic picture in lacunar angina is characterized by the appearance on the hyperemic surface of enlarged tonsils, first limited at the mouths of the lacunae, and then more and more widely covering the tonsil of islands of yellowish-white plaque. Sometimes individual areas of plaque merge and cover a larger or smaller part of the tonsil, without going beyond its limits. Plaque is easily removed without damaging the epithelial layer. During the period of plaque separation, on days 2–5, the severity of symptoms most often decreases, but the temperature usually remains low-grade until the inflammatory reaction in the regional lymph nodes subsides. The duration of the disease is 5–7 days; in case of complications, it can be delayed for a longer period.
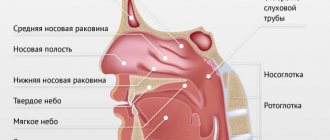
In addition to the palatine tonsils, acute inflammation may also involve other accumulations of lymphadenoid tissue, in particular those located in the nasopharynx (retronasal tonsillitis - adenoiditis, tubular tonsillitis), at the root of the tongue (lingual tonsillitis or tonsillitis IV of the tonsil). Sometimes the inflammation is diffuse, spreading throughout the lymphadenoid pharyngeal ring.
Acute inflammation of the pharyngeal tonsil (adenoiditis) is characterized by: sore throat, radiating to the deep parts of the nose, difficulty nasal breathing. The disease occurs mainly in pediatric practice.
Damage to the lingual tonsil is accompanied by pain when swallowing and when protruding the tongue. Inflammation, spreading to connective and intermuscular tissue, can lead to interstitial purulent inflammation of the tongue.
Complications
Inadequate treatment of follicular tonsillitis can lead to purulent complications.
The first place in frequency is paratonsillar abscess - the formation of an abscess in the soft tissues surrounding the tonsil. With this disease, fever persists for a long time, and opening the mouth is so painful that the patient even refuses to take fluids. Surgery is often required. Purulent lymphadenitis and other pathological processes associated with the spread of bacterial infection and the need for surgical drainage of a purulent focus also occur.
3-5 weeks after an acute streptococcal infection, signs of delayed infectious and allergic complications may appear. Possible damage to the myocardium and valve apparatus, which is accompanied by pain in the heart, rhythm disturbances, and shortness of breath. There is swelling of the joints, pain when moving, and a feeling of stiffness.
The development of glomerulonephritis is possible - kidney damage with decreased diuresis, fluid retention, and arterial hypertension. These conditions require consultation with specialists - a cardiorheumatologist and a nephrologist, respectively.
Follicular tonsillitis
Features of the disease
The peripharyngeal ring is a collection of lymphoid tissue, which is an important peripheral organ of the body's immune system. Pathogenic microorganisms that enter the body with food and water are retained in the oral or nasal cavity precisely by the tonsils of the peripharyngeal ring. As a result of the struggle between the body and the infectious agent, a local reaction of the tonsils occurs, which is expressed in increased production of lymphocytes and can lead to tissue inflammation.
Inflammation of the tonsils can also be caused by an internal infection of the body, namely diseases of the oral cavity or ENT organs: caries, sinusitis, rhinitis, otitis media, etc. When the body's immune defense is weakened due to illness or hypothermia, opportunistic microflora found in the growth or nasal cavity can provoke acute inflammation of the tonsils. Factors that provoke pathology are bad habits (smoking and alcohol abuse), diseases of the gastrointestinal tract, working in hazardous working conditions, and unhealthy diet.
The risk group for the disease includes pregnant women, the elderly and children, as well as people with chronic damage to the immune system.
Diagnostics
To make a diagnosis, an examination by a doctor - a therapist, pediatrician or otorhinolaryngologist - is sufficient. Pharyngoscopy (examination of the oropharynx with a spatula) reveals a significant enlargement of the palatine tonsils, the presence of exudate - white, gray or yellow purulent discharge, swelling of the palatine arches and uvula, and sometimes a bruise-like rash on the soft palate. In order to understand how to treat follicular tonsillitis , and to understand the follow-up plan after the illness, additional examinations may be required:
- general blood test with calculation of leukemia and determination of erythrocyte sedimentation rate (ESR),
- rapid test to detect group A streptococcus,
- examination of a smear from the back wall of the pharynx to determine the pathogen with a negative strep test.
As a rule, it is possible to differentiate viral and bacterial origin already at the examination stage:
- With a viral etiology, tonsillitis is accompanied by a runny nose, hoarseness or conjunctivitis.
- GABHS infection is characterized by petechiae of the soft palate, enlargement and tenderness of the lymph nodes in the neck.
- Epstein-Barr viral infection is characterized by generalized lymphadenopathy (affecting all groups of lymph nodes), an increase in the size of the liver and spleen.
- Enteroviral stomatitis has a summer seasonality and is accompanied by a rash on the palms and soles, which is why it is called “hand-foot-mouth disease.”
- Diphtheria is characterized by abundant dense deposits that are difficult to separate from the bleeding surface.
Recurrent episodes of tonsillitis must be differentiated from Marshall syndrome - recurrent attacks of febrile fever, aphthous stomatitis, pharyngitis and cervical lymphadenitis. Exacerbations occur every 2-8 weeks. The deterioration in health lasts 1-2 days and is relieved by the administration of glucocorticosteroids at the beginning of the episode. More common in children. It stops completely within a few years.
Classification of the disease
Inflammatory pathology of the tonsils varies:
- by type of pathogen, can be bacterial, viral or fungal in nature;
- by the nature of the course - acute or chronic;
- according to the clinical picture - catarrhal, follicular or lacunar.
Sore throat can be primary (simple), which occurs when a bacterial infection penetrates, secondary, which occurs against the background of other diseases of the body, and also specific, caused by the action of a specific agent.
Treatment of follicular sore throat
The need for hospitalization for acute tonsillitis is determined by the severity of the general condition. As a rule, follicular purulent tonsillitis is treated at home. Until the end of the fever, it is recommended to observe bed rest, then gentle rest, i.e. the patient should stay at home and avoid physical activity. A sufficient amount of liquid (warm teas, fruit drinks, juices) helps relieve fever and eliminate bacterial toxins. You need to eat according to your appetite - do not force yourself to eat, but give preference to light, low-fat dishes.
Etiotropic treatment is of key importance - the prescription of drugs that suppress the pathogen. For bacterial infections, antibiotics are indicated for follicular angina - protected penicillins, cephalosporins of the 1st-2nd generation, in case of intolerance to beta-lactam antibiotics - macrolides or lincosamides. For a fungal pathological process, antifungal drugs are indicated - fluconazole, ketoconazole, etc. Herpetic tonsillitis requires the prescription of acyclovir. It is critical to maintain the full course of etiotropic therapy, and not stop taking medications when the first relief occurs. An incomplete course contributes to the formation of microflora that is resistant to medications - more aggressive and difficult to treat.
To eliminate the immunopathological process, the use of antihistamines is indicated. During the period of fever, antipyretic therapy (ibuprofen, paracetamol or nimesulide in appropriate dosages) is recommended.
Local treatment to reduce pain in the throat is prescribed in the form of sprays or gargles. It is necessary to keep in mind the risk of aspiration when resolving tablets and laryngospasm when using the spray in young children. Mechanical removal of plaque is contraindicated.
During the period of convalescence, physical therapy is possible as prescribed by the attending physician.
Treatment of the disease
In most cases, treatment is carried out on an outpatient basis. Patients are prescribed bed rest, warm, plenty of fluids, and food should be light and liquid. Treatment, depending on the type of sore throat, includes antibacterial therapy, antiviral drugs and local symptomatic treatment. Additionally, the tonsils are irrigated with anti-inflammatory drugs, gargling with herbal decoctions and antiseptic solutions. To reduce swelling and symptoms of intoxication, antihistamines are indicated. The course of treatment is 5-10 days.
Diagnosis of acute tonsillitis
To clarify the diagnosis and prescribe treatment, consult a specialist. The diagnosis of tonsillitis can be made by a doctor based on anamnesis, complaints, examination data, and clinical picture.
Laboratory studies include bacteriological (detection of the growth of pathogenic flora in biomaterials from the oropharynx, for example, group A β-hemolytic streptococcus) and serological (determination of antibodies to streptococcal antigens in the blood serum or other media being tested).
There will also be changes in the patient’s blood (leukocytosis, increased ESR, in more severe cases anemia, thrombocytopenia); protein and red blood cells may be detected in the urine if the kidneys are damaged.
If there are plaques on the tonsils, diphtheria should be excluded, especially in unvaccinated individuals. The plaque of diphtheria is characteristic: it is dense, dirty white or yellow, and appears by the second day of illness. The film cannot be rubbed with a spatula; it requires effort to remove it; if you lower the film into a vessel with liquid, it will sink.
Body temperature during diphtheria is often subfebrile (no more than 38 degrees), which does not correspond to the severity of the condition, which progressively worsens. Muscle pain, general weakness, and difficulty breathing appear.
The diagnosis is also confirmed by bacteriological examination of samples taken from the tonsils. The test material is placed on a nutrient medium. With this method, diphtheria bacilli can be detected in 80% of cases.
Differential diagnosis of acute tonsillitis is carried out with the aim of carrying out etiotropic therapy (impact on the cause of the disease). With scarlet fever and measles, tonsillitis will be accompanied by the appearance of a rash; the epidemiological history is also characteristic; children are mainly affected. With infectious mononucleosis, a distinctive feature will be changes in the blood test: namely, the presence of atypical mononuclear cells, with agranulocytic tonsillitis - a decrease in leukocytes and granulocytes in the blood, and with leukemia - the presence of blast cells.
Up to contents
Complication of the disease
Sore throat is dangerous because of its complications, which can be early, i.e. occurring immediately after inflammation of the tonsils or delayed, which appear 3-4 weeks after purulent inflammation. Complications can be single (affect one organ) or multiple and affect several organs.
Early complications of tonsillitis are otitis media, lymphadenitis, sinusitis, sinusitis, laryngeal edema, tonsil abscess, etc. Delayed inflammation provokes diseases of the heart muscle (rheumatism of the heart muscle, myocarditis, pericarditis), joint pathologies (rheumatism, arthritis), kidney diseases (glomerumetritis, pyelonephritis, renal failure).
In medical clinics, at any time convenient for you, they will provide timely and qualified assistance for any diseases of the ENT organs in patients of all age categories. The clinics are equipped with modern diagnostic equipment for diagnosing ENT diseases, and patients also have a modern diagnostic laboratory at their disposal, in which all necessary laboratory tests are performed.
Our otorhinolaryngology doctors have extensive experience in diagnosing and treating various diseases of the ear, nose and throat in adults and children, using both conservative and surgical methods. When the first symptoms of a sore throat or other pathologies appear, do not delay visiting a doctor and seek qualified medical help. You can make an appointment by calling the center or leaving a request on the website.
Treatment of acute tonsillitis
Depends on the severity of the patient’s condition and the stage of development of the disease. Hospitalization is necessary in cases of disruption of the functioning of other organs and systems (lower back pain, changes in urine, arrhythmia, heart failure, suspicion of a heart defect), in case of moderate and severe disease, if a child is sick, as well as social indications (closed groups , boarding schools).
Clinical recommendations for the treatment of acute tonsillitis in adults include non-drug treatment methods: bed rest, isolation of the patient if possible, a gentle diet excluding cold, hot, and solid foods. A diet of plant and dairy products (porridge, stewed vegetables) is preferable. Drinking plenty of fluids is necessary. Frequent ventilation and humidification of the air in the room where the patient is located has a beneficial effect. During treatment, the patient is provided with separate dishes and hygiene items.
Local therapy of acute tonsillitis occupies a special place. In combination with other drugs, it speeds up recovery, relieves discomfort in the throat, and is applicable when systemic therapy is contraindicated7. Methods of irrigating the pharynx with various solutions, for example Hexoral ® spray, can be effective. Its action is based on the suppression of the oxidative metabolism of microbes (thiamine antagonist). The drug can fight many bacteria and fungi, in particular the pathogenic fungi Candida, and Hexoral ® also inhibits the growth of Proteus and Pseudomonas aeruginosa. In addition, the active substance Hexetidine has an analgesic effect on the mucous membrane4. An important method of local therapy is rinsing the tonsils with antiseptic solutions (Hexoral ®, Chlorhexidine, chamomile infusion and others). Also tested are Hexoral ® Tabs Extra5 and Hexoral ® Tabs Classic6 lollipops, which contain antimicrobial components and antiseptics. The active components of Hexoral ® Tabs destroy the walls of bacteria, fight infection, thereby helping to reduce sore throat. They should be kept in the mouth until completely dissolved. It is important to remember that after local treatment it is better not to eat or drink for at least 1 hour.
To reduce inflammation, pain, and in order to reduce high fever, analgesics, anti-inflammatory and antipyretic drugs (ibuprofen, paracetamol and others) are prescribed.
In severe cases, medical treatment includes systemic antibiotics. Remember that self-prescribing antibiotics can be dangerous to your health.
Treatment of sore throat in a child must be carried out under the supervision of a doctor! Diphtheria is especially dangerous for children.
Patients with diphtheria should be hospitalized in the infectious diseases department.
Up to contents
Causes
For effective treatment, it is extremely important to make the correct diagnosis. To determine the etiological factor, consult your doctor. What are the causes of acute tonsillitis? The most common types of microbes that cause sore throat are group A streptococci and staphylococci. In the ICD 10 classification of diseases, acute inflammation of the tonsils is designated by the code J03.0 - streptococcal tonsillitis, J03.8 - acute tonsillitis caused by other specified pathogens, J03.9 - acute unspecified tonsillitis3.
Among other causes of acute tonsillitis there are: other bacteria, fungi, viruses, protozoa, and in severe cases their associations: fungal-bacterial, viral-bacterial. Other pathogens are less common: for example, anaerobic microorganisms, chlamydia, mycoplasma, as well as representatives of the normal microflora of the oral cavity, which, when the immune system is weakened, can cause acute bacterial tonsillitis.
In the pathogenesis (the path of disease development) of acute tonsillitis, the state of the body, its resistance to external factors, the presence of foci of chronic infection of the oral cavity, and difficulty in nasal breathing (especially often in children) also play a role. The process of inflammation can also be triggered by a lack of vitamin C, B vitamins, stress, or a sudden change in climate.
Up to contents