Hyperthyroidism is a condition of hyperfunction of the thyroid gland, which is accompanied by excessive production of thyroxine and triiodothyronine. An increase in the level of hormones in the blood accelerates metabolic processes in the body and has a negative effect on almost all organ systems. Symptoms of hyperthyroidism reduce the patient's quality of life. Hyperthyroidism is a condition of hyperfunction of the thyroid gland, which is accompanied by excessive production of thyroxine and triiodothyronine. An increase in the level of hormones in the blood accelerates metabolic processes in the body and has a negative effect on almost all organ systems. Symptoms of hyperthyroidism reduce the patient's quality of life.
Adequate and timely treatment allows you to prevent complications and slow down pathological processes, up to the complete restoration of thyroid function.
Types of hyperthyroidism
There are three forms of the disease:
- Subclinical. There are no obvious symptoms, T4 levels are normal, triiodothyronine levels are low;
- Manifest. Characteristic signs of hyperthyroidism appear. T4 level is normal, triiodothyronine level is low;
- Complicated. Symptoms include heart failure, arrhythmia, psychosis and other severe conditions.
According to the level of occurrence of hyperthyroidism, there are:
- primary – pathology of the thyroid gland;
- secondary – the pituitary gland is affected;
- tertiary – processes develop in the hypothalamus.
Causes of hyperthyroidism
A number of endocrine diseases lead to thyroid dysfunction, such as:
- Graves' disease (Bazedow, Bazedow-Graves) . The syndrome is autoimmune in nature. The body produces antibodies that stimulate the thyroid gland to produce excess amounts of the hormone T4;
- Nodular goiter, toxic adenoma . The listed pathologies are accompanied by the formation of benign nodes in the tissues of the gland. The formations begin to produce hormones and cause hyperthyroidism. Doctors cannot yet say for sure why some adenomas synthesize T4 and others do not;
- Thyroiditis . The inflammatory process destroys thyroid cells. Hormones enter the bloodstream and cause hyperthyroidism. The autoimmune nature of thyroiditis is possible. The body produces antibodies against TSH receptors. The cells cause active growth and inflammation of the thyroid gland.
People with a hereditary predisposition to endocrine pathologies are most susceptible to the disease. Symptoms of hyperthyroidism are more common in women than in men. The development of the disease is also influenced by the environmental situation, chronic iodine deficiency, and stress.
What is Graves' disease?
Graves' disease is the main cause of thyrotoxicosis. According to the Graves' Disease and Thyroid Foundation, about 2-3 percent of the population - about 10 million people - have the disease.
The Virginia Mason Institute states that 70-80 percent of patients with thyrotoxicosis have Graves' disease. This is an autoimmune disease where the immune system attacks the thyroid gland. In response, the thyroid gland produces too much thyroid hormone.
The pituitary gland releases a hormone that helps control thyroid function. Thyrotropin receptor antibodies (Trab) are associated with Graves' disease, and they work as a pituitary hormone regulator. As a result, Trab overrides the normal regulation of the thyroid gland and causes thyrotoxicosis.
Anyone can develop Graves' disease, but there are a number of factors that increase the risk, including:
Women are more likely than men to develop Graves' disease.
- Family history of Graves' disease or other thyroid or autoimmune diseases
- Other autoimmune disorders: People with other immune disorders such as type 1 diabetes or rheumatoid arthritis are at increased risk
- Emotional or physical stress: Stressful life events or illnesses can trigger the onset of Graves' disease
- Pregnancy: Pregnancy or recent childbirth may increase the risk of the disease in some women
- Cigarette smoking may affect the immune system and increase the risk of Graves' disease
Women are also more likely to develop the disorder than men. According to the Office of Women's Health, it affects 10 times more women than men, and often strikes while they are in their 20s and 30s.
Symptoms of hyperthyroidism
The first signs of dysfunction are uncharacteristic, so the disease is often confused with other somatic conditions. Symptoms of hyperthyroidism of the thyroid gland increase as metabolic processes in the body are disrupted.
Main signs of the disease:
- loss of body weight while maintaining appetite, volume and quality of food;
- arrhythmia, tachycardia;
- anxiety, depression;
- increased sweating;
- fine tremor of fingers and hands;
- indigestion;
- the formation of a visible goiter, changing the contours of the neck;
- increased fatigue.
A symptom of hyperthyroidism in men is a decrease in potency and libido. In women, increased levels of thyroid hormones cause menstrual irregularities. Pregnancy may end in spontaneous abortion. A symptom of thyroid hyperthyroidism in women can also be decreased fertility, including infertility. During menopause, the pathology in the initial stages is asymptomatic.
Complications of hyperthyroidism
As the disease progresses, the symptoms of thyroid hyperthyroidism intensify, and complications may arise:
- Disturbances in the functioning of the heart . Atrial fibrillation is added to the general symptoms of hyperthyroidism. The patient does not tolerate physical activity well, and there is a disturbance in heart rhythm. Congestive heart failure may develop. The consequences are reversible. After eliminating hyperthyroidism, the signs of arrhythmia are completely cured.
- Increased bone fragility . In its advanced form, hyperthyroidism causes disturbances in the structure of bone tissue. Osteoporosis develops. The reason bones become brittle is that excess hormones prevent calcium from being incorporated into the bone.
- Eye diseases . Graves' ophthalmopathy adds to the symptoms of hyperthyroidism. The cause of the pathology is the growth and swelling of the tissues located behind the eyeballs. The patient feels pain in the eyes, sensitivity to light, and complains of double vision. Visual acuity gradually decreases. In advanced cases, blindness develops.
- Skin problems . Ocular symptoms in hyperthyroidism often develop in parallel with Graves' dermopathy. The skin becomes swollen and red, especially around the feet and legs.
- Thyrotoxic crisis . An increase in the level of thyroid hormones in the blood can cause a sudden fever and an increase in all the main symptoms. Thyrotoxic crisis is accompanied by tachycardia. In some cases, delirium (mental disorder) occurs. The patient requires emergency medical care.
Clinical picture
Thyrotoxic crisis is a pathology that develops against the background of severe Graves' disease or diffuse toxic goiter. These diseases relate to thyroid dysfunction, accompanied by excessive production of thyroid hormones (T3, T4). High levels of thyroid hormones cause severe thyrotoxicosis, which is the impetus for the development of thyrotoxic crisis.
Differences between hypo- and hyperthyroidism
Influencing factors
The disease in most cases develops in women at a young age. The ratio of cases of the disease in men to women is 1:9. There are several factors that cause the development of pathology.
This:
- surgical intervention to remove toxic diffuse goiter;
- effect of ether anesthesia during operations;
- tooth extraction;
- exposure to x-rays during examination of the thyroid gland;
- therapy using radioactive iodine;
- unsystematic use of drugs that correct the production of thyroid hormones;
- taking iodine-containing drugs during X-ray examination;
- mechanical damage to the thyroid gland.
But, in addition to the above factors, the pathological process can be provoked by:
- stress;
- intense physical activity;
- infectious diseases;
- cerebrovascular dysfunction;
- injuries and damages;
- exacerbation of chronic diseases;
- pulmonary embolism;
- difficult pregnancy and childbirth;
- any surgical interventions.
Severe stress can cause thyrotoxic crisis
Important. In children, thyrotoxic crisis is a very rare phenomenon, the etiology of which is not fully determined. It is assumed that the impetus for the development of the disease is a sudden release of thyroid hormones, while their concentration in the blood is not high. Emergency care for thyrotoxic crisis in children should be provided immediately at the first suspicion.
Etiology
The main reason for the development of thyrotoxic crisis is a sharp increase in the concentration of thyroid hormones in the blood.
This phenomenon is characterized by the following processes:
- high adrenal insufficiency, with increasing deficiency of the hormones they produce;
- increased metabolism of catecholamines (substances that stimulate the activity of the glands of the endocrine system);
- activation of the system of subcortical centers of the hypothalamus and the reticular formation of the brain.
The above changes in the body lead to the fact that against their background, a person’s reserve forces cannot cope with the problem, which is why a thyrotoxic crisis develops, which requires urgent treatment.
Attention. The development of the crisis occurs suddenly, which aggravates the current situation. But sometimes you can observe a prodromal period, when symptoms increase gradually and unnoticeably. In this case, it is possible to promptly recognize the disease and stop an attack of thyrotoxic crisis.
The photo shows people suffering from thyrotoxicosis, which is a factor in the development of a crisis.
Symptoms
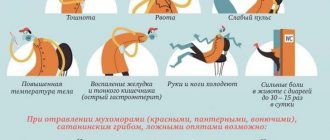
The pathological condition is characterized by an acute and abrupt onset of development, the symptoms of which gradually increase.
In the clinical picture, the following symptoms of thyrotoxic crisis can be distinguished:
- febrile body temperature (up to 40 degrees);
- activity of the musculoskeletal system;
- mental anxiety;
- excitation;
- strong heartbeat;
- suffocation;
- causeless panic and fear;
- pain in the heart area;
- headache;
- the skin is hot, hyperemic;
- high sweating;
- dyspnea;
- sinus tachycardia;
- tremor of the limbs;
- anuria (decreased urine output).
Extreme psychological instability
In addition to the above symptoms, disorders in the central nervous system, gastrointestinal tract, and cardiovascular system are observed.
Table No. 1. Dysfunction of individual body systems:
|
|
| central nervous system | CNS function disorders are observed in 90% of all cases of pathology. May manifest:
|
| The cardiovascular system | Accompanied by the following symptoms:
|
| Gastrointestinal system | Accompanied by the following symptoms:
|
Patients with thyrotoxic crisis are incapacitated in most cases. This pathology is very dangerous, especially for people over 60 years of age. Therefore, it is very important that emergency care is provided in a timely manner during a thyrotoxic crisis; the cost of the patient’s life depends on this.
The patient is treated in the intensive care unit
Attention. Symptoms such as severe vomiting, diarrhea and high body temperature are a consequence of dehydration. Death occurs after hypovolemic shock, thyrotoxic coma and high heart failure. The mortality rate in this case is 100%.
In 1977, medical scientists identified 3 stages of thyrotoxic crisis, varying in severity.
Table No. 2. Symptoms of the three stages of the disease:
|
|
| First stage | The following symptoms appear:
|
| Second stage | After the first stage symptoms appear, the following are added:
|
| Third stage | After signs of a thyrotoxic crisis of the first and second stages appear, the victim falls into a coma. |
Diagnosis of hyperthyroidism
Consultation with an endocrinologist
Diagnosis of hyperthyroidism begins with an appointment with an endocrinologist. At the appointment, the doctor asks the patient questions that will help in diagnosis: how long ago did the clinical symptoms appear, what is the dynamics of the disease, are there any other patients with goiter or thyroiditis in the family. A physical examination is required: palpation of the thyroid gland. In case of obvious hyperthyroidism, the doctor will try to palpate the contours of the organ, determine its position, uniformity of structure, and pain. After the examination, the patient receives directions for further examinations to accurately diagnose the cause of the disease.
Laboratory research
Hyperthyroidism is confirmed by blood tests to measure the level of thyroid hormones. Elevated levels of thyroxine in the absence or minimal amount of TSH indicate hyperfunction of the gland. A blood test is especially important in the early diagnosis of the disease in older people. For example, menopausal women may not have symptoms of hyperthyroidism. Pathology is detected only by the results of laboratory tests.
A blood test helps confirm the condition of the endocrine organ, but additional tests will be required to determine the cause of hyperthyroidism.
Instrumental research methods
Ultrasonography. Ultrasound of the thyroid gland allows you to determine the shape and size of the lobes, assess the degree of its enlargement, and detect nodes, cysts, and other neoplasms.
Radioisotope scintigraphy . The patient is given a special solution intravenously. The drug contains radioactive isotopes of iodine, which are actively captured by the thyroid gland. After some time, the doctor assesses the degree of saturation of the tissues and makes a conclusion about their functionality. A large amount of radioiodine indicates excessive production of thyroxine, which develops, in particular, with Graves' disease.
If, with severe symptoms of thyroid hyperthyroidism in a woman or man, a minimal amount of isotopes is observed in the gland, then the probable cause of the pathology is thyroiditis. The radioactive iodine uptake test helps in differential diagnosis.
Fine needle biopsy . Under the control of an ultrasound probe, the doctor takes samples of thyroid tissue for examination. Biopsy materials make it possible to determine the nature of the neoplasm: benign or malignant. The study results also provide information about autoimmune processes that may cause hyperthyroidism.
Diagnosis and treatment
Thyrotoxic crisis is an extremely severe pathological condition, so treatment is carried out only in the intensive care unit, where the doctor prescribes appropriate rehabilitation therapy. It is important that timely assistance is provided to the victim, therefore, at the first suspicion of a crisis, the patient should be urgently hospitalized, and then specialists will carry out a full diagnosis.
Diagnostics
To diagnose the disease, a number of laboratory tests are carried out to determine:
- blood ESR level;
- degree of concentration in the blood of T3 and T4;
- degree of concentration of the hormone TSH;
- level of adrenal hormone (cortisol);
- blood glucose and cholesterol levels.
Blood for thyroid hormones
An ECG study allows you to determine the presence of tachycardia and various types of arrhythmia. The most common manifestation is atrial fibrillation caused by an excess of thyroid hormones.
Another effective diagnostic method is ultrasound examination, which allows you to determine the size of the thyroid gland and the speed of blood flow in the tissues of the organ. The diagnosis is established based on the results of the examination and the patient’s medical history.
Ultrasound of the thyroid gland allows you to determine the speed of blood flow and its size
Treatment of hyperthyroidism
The approach to therapy depends on the cause of hyperthyroidism, the age and condition of the patient.
Conservative treatment methods:
- Radioactive iodine preparations . Isotopes accumulate in the tissues of the thyroid gland, suppressing compensatory mechanisms. The organ decreases in size, the symptoms of hyperthyroidism gradually weaken. Treatment takes several months. It is important that radioactive iodine suppresses gland function, so over time the patient may develop hypothyroidism, which is corrected by hormone replacement therapy.
- Antithyroid drugs . Medicines suppress the production of thyroid hormones. Symptoms decrease within a few weeks after taking the drugs in the correct dosage. The course of treatment is up to 1 year or longer. In some cases, hyperthyroidism is cured completely, but sometimes relapses occur. It is important that antithyroid drugs can cause allergies, individual intolerance, and can reduce immunity. The effects of this group of drugs cause disturbances in liver function. You can take medications only under the supervision of a doctor.
- Symptomatic treatment . Depending on the severity of the manifestations of hyperthyroidism, the doctor may prescribe medications to lower blood pressure, maintain heart rhythm, etc. Symptomatic treatment is continued until the patient’s general well-being improves.
In cases of severe hyperthyroidism, accompanied by significant enlargement of the thyroid gland, multiple neoplasms in functional tissue, as well as medullary cancer, surgical intervention is indicated. The doctor partially or completely removes the endocrine organ. After the operation, the patient is given a dosage of hormones that are taken for life.
Thyrotoxic crisis (thyroid crisis)
The importance of early treatment of thyrotoxic crisis , the diagnosis of which is based on clinical impression, cannot be overestimated. Before starting treatment, blood should be drawn to test thyroid function and determine cortisol levels, as well as a complete clinical blood count and routine biochemical tests. Cultures are indicated to detect infection. It is advisable to draw up a clear treatment plan to avoid unnecessary delay in specific therapy. The goals of specific treatment are: maintaining the basic functions of the body at the physiological level; inhibition of thyroid hormone synthesis; slowing the release of thyroid hormones; blockade of the effects of thyroid hormones in the periphery; identification and correction of provoking factors. You should strive to achieve all of these goals simultaneously.
Maintaining Basic Body Functions Adequate hydration with intravenous fluids and electrolytes is indicated to replace so-called insensible losses, as well as losses through the gastrointestinal tract. Additional oxygen administration is necessary due to increased oxygen consumption. During a crisis, hyperglycemia and hypercalcemia may occur; they are usually corrected with fluids, but in some cases specific therapy is required to reduce unacceptably high calcium and glucose levels. Fever is controlled with antipyretics and a cooling blanket. Acetylsalicylic acid should be used with caution or not at all, since salicylates increase free T) and T4 levels due to decreased protein binding. This consideration is rather theoretical, since no adverse effects have been noted with the use of acetylsalicylic acid. During thyrotoxic crisis, sedatives should be used with caution. Sedation depresses consciousness, which reduces the value of this parameter as an indicator of clinical improvement in the patient’s condition. In addition, it can cause hypoventilation.
Congestive heart failure is treated with digitalis and diuretics, although failure due to hyperthyroidism may be refractory to digitalis. Cardiac arrhythmias are treated with conventional antiarrhythmic drugs. Atropine should be avoided as its parasympatholytic effect may increase heart rate. In addition, atropine may counteract the effects of propranolol.
Intravenous glucocorticoids are prescribed in a dose equivalent to 300 mg hydrocortisone per day. The role of the adrenal glands in the pathogenesis of thyrotoxic crisis is unclear, but the use of hydrocortisone has been shown to improve survival. Dexamethasone has some advantages over other glucocorticoids, as it reduces the conversion of T4 to T3 in the periphery.
Inhibition of thyroid hormone synthesis Antithyroid drugs propylthiouracil (PTU) and methylmazole block the synthesis of thyroid hormones by inhibiting the organification of tyrosine residues. This action begins within an hour after administration, but the full therapeutic effect is not achieved even after several weeks. Initially, a loading dose of PTC is prescribed (900-1200 mg, and then 300-600 mg per day for 3-6 weeks or until a therapeutic effect is obtained (control of thyrotoxicosis). An acceptable alternative is the administration of methylmazole at an initial dose of 90-120 mg followed by 30-60 mg per day. Both drugs are administered orally or through a nasogastric tube, since their parenteral forms are not available. PTU has an advantage over methyl mazole: it inhibits the peripheral conversion of T4 to T3 and produces a therapeutic effect more quickly. Although these drugs inhibit synthesis again formed thyroid hormones, they do not affect the release of already accumulated hormones.
Slowing down the release of thyroid hormones The introduction of iodine preparations immediately slows down the release of thyroid hormones from the sites of their accumulation. Iodides can be given as strong iodine solutions (30 drops orally every day) or as sodium iodide (1 g every 8 to 12 hours as a slow intravenous infusion). Iodide should be administered an hour after a loading dose of an antithyroid drug to prevent the thyroid gland from using iodine during the synthesis of new hormone.
Blockade of the peripheral effects of thyroid hormones Adrenergic blockade is the mainstay of treatment for thyrotoxic crisis. In an extensive series of observations, Waldstein et al. (1960) noted an increase in patient survival when using reserpine. Guanethidine was subsequently demonstrated to be effective in alleviating the symptoms and signs of thyrotoxicosis due to sympathetic hyperactivity. Currently, the beta-blocker propranolol is the drug of choice. In addition to reducing sympathetic hyperactivity, propranolol partially blocks the conversion of T4 to T3 in the periphery.
Propranolol can be administered intravenously at a rate of 1 mg/minute, with careful increases in the dose of 1 mg every 10 to 15 minutes until a total dose of 10 mg is reached. The positive effects of the drug (control of cardiac and psychomotor manifestations of thyrotoxic crisis) are observed within 10 minutes. The lowest dose sufficient to control thyrotoxic symptoms should be used; if necessary, this dose can be repeated every 3-4 hours. The oral dose of propranolol is 20-120 mg every 4-6 hours. When administered orally, propranolol is effective for approximately 1 hour. Propranolol has been successfully used in the treatment of thyrotoxic crisis in children. Young children may require high doses of the drug (240-320 mg/day orally).
Usual precautions should be taken when prescribing propranolol to patients with bronchospastic syndrome and heart block. If it is used, a preliminary ECG study is carried out to assess conduction disorders. In patients with congestive heart failure, the beneficial effects of the drug (reduction in heart rate and some arrhythmias) should be compared with the risk of its use (inhibition of myocardial contractile function with beta-adrenergic blockade). Urbanic believes that the benefits of propranolol treatment outweigh the risks in this situation, but the author recommends pre-administration of digitalis.
When treating thyrotoxicosis or thyrotoxic crisis, propranolol should not be relied upon alone. Two cases of thyrotoxicosis occurring in patients who received seemingly adequate propranolol therapy for thyrotoxicosis are described. It is known that with a single or repeated oral dose of propranolol, its plasma level is very variable in controls and in patients with thyrotoxicosis. Treatment of thyrotoxic crisis should be quite flexible and individualized.
One of the authors recommends a gradual reduction in the dose of propranolol as the thyrotoxic crisis resolves. He believes that an objective assessment of the patient's condition may be difficult because propranolol masks the symptoms of hypermetabolism. In patients who have already received beta blockers, the symptoms of thyroid crisis may be masked, which carries the risk of late diagnosis of thyrotoxic crisis.
Alternative drugs to propranolol are guanethidine and reserpine, which also provide effective autonomic blockade. Guanethidine reduces catecholamine stores and blocks their release. When administered orally at 1-2 mg/kg per day (50-150 mg), it is effective within 24 hours, but its maximum effect may take several days. Toxic reactions are cumulative and include postural hypotension, myocardial decompensation and diarrhea. The advantage of guanethidine over reserpine is the absence of the pronounced sedative effect characteristic of reserpine.
The action of reserpine is aimed at reducing catecholamine reserves. After the initial dose (1-5 mg intramuscularly), the drug is administered every 4-6 hours at 1-2.5 mg. Improvement in the patient's condition can be observed after 4-8 hours. Side effects of reserpine include drowsiness, mental depression (this can be severe), cramping abdominal pain and diarrhea.
Identification and elimination of provoking factors A thorough assessment of the provoking factors of thyrotoxic crisis is carried out. Treatment of thyrotoxic crisis should not be delayed until these factors are identified; appropriate examination can be carried out as the patient’s condition stabilizes. The provoking factor is identified in 50-75% of cases.
Recovery After starting treatment, symptomatic improvement is observed within a few hours, primarily due to adrenergic blockade. Elimination of a thyrotoxic crisis requires the destruction of circulating thyroid hormones, the biological half-life of which is 6 days for T4 and 22 hours for T3. Thyrotoxic crisis can last from 1 to 8 days (average duration - 3 days). If standard methods of crisis control are unsuccessful, alternative therapeutic options may be considered, including peritoneal dialysis, plasmapheresis, and charcoal hemoperfusion to remove circulating thyroid hormones. After recovery from the thyrotoxic crisis, radioactive iodine therapy is the treatment of choice for hyperthyroidism.
Mortality If thyrotoxic crisis is untreated, the mortality rate approaches 100%. There is a reduction in mortality with the use of antithyroid drugs. The lowest mortality rate for thyrotoxic crisis over a 10-year period is reported to be 7%; its usual figure is 10-20%. In many cases, the cause of death is a preexisting disease. The main means of reducing mortality, of course, is to prevent the development of thyrotoxic crisis. Early recognition and timely treatment of this complication of hylerthyroidism gives the patient a better chance of survival.
Prevention of hyperthyroidism
People with a family history, women during menopause and older men need to be examined annually by an endocrinologist and take a blood test to check the level of thyroid hormones.
It is recommended to balance the diet according to the BZHU and introduce foods rich in vitamins A, B, C and minerals into the diet. Diet and hydrotherapy help not only in the prevention of hyperthyroidism, but also in the rehabilitation of patients after treatment. Regular visits to specialized sanatoriums help maintain and improve the health of the endocrine system.