Arterial hypertension is the most common cardiovascular pathology, affecting about 40% of the adult European population [1]. Of course, this leads to high demand for antihypertensive drugs, regardless of the season. And although the chief’s task is, first of all, to offer several drug options according to the INN prescribed in the prescription, he also has to explain side effects, dosage, and sometimes answer questions about the features of the mechanism of action. Therefore, we decided to offer our readers a series of articles about the group of antihypertensive drugs and the features of working with requests for them. Let's start with blockers of the renin-angiotensin-aldosterone system.
RAAS: the basics
Before we begin describing the drugs, let’s dive briefly into the intricacies of pharmacology and once again remember what the mechanism of action of the renin-angiotensin-aldosterone system, or RAAS, is.
The RAAS is a complex hormonal-enzymatic system in which almost all organs and tissues of the body are involved, but the key roles in it belong to the liver, kidneys, adrenal glands and lungs.
Alpha-2‑globulin angiotensinogen is constantly synthesized in the liver. At the same time, the kidneys produce the enzyme renin in response to decreased intrarenal pressure, decreased delivery of sodium and chloride, and hypoxia. It enters, like angiotensinogen, into the systemic circulation, where it binds to it to form angiotensin I.
Angiotensin I is a practically inert substance. It does not act on blood vessels and is only a precursor of the active component angiotensin II. In the formation of the latter, along with angiotensin I, angiotensin-converting enzyme (ACE), which is produced in the lungs, is involved.
Angiotensin II is the main link in the RAAS circuit.
It exhibits a powerful vasoconstrictor effect and affects the target organs in which its receptors are located. First of all, we are talking about the endothelium, heart and kidneys. This is why high levels of angiotensin II are associated not only with increased blood pressure, but also with damage to the vascular wall, myocardium, kidneys, and the development of chronic heart and kidney failure.
In addition, angiotensin II causes increased synthesis of the adrenal hormone aldosterone. The latter is involved in the control of blood pressure (BP) by regulating the homeostasis of potassium, sodium and intracellular fluid volume. Under its influence, blood pressure increases and the sensitivity of vascular smooth muscles to vasoconstrictor substances, including angiotensin II, increases.
Thus, the RAAS is directly involved in the drama called “arterial hypertension”, playing one of the main roles in it. Fortunately, it is possible to block this system. This can be done with drugs of two pharmacological groups - angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs, also known as sartans).
Features of the treatment of hypertension
Therapy for hypertension is not carried out periodically, but with the constant use of an antihypertensive drug.
It is an extremely dangerous misconception to use the drug only “when there is pressure.” If hypertension is diagnosed, there is a tendency for a persistent increase in systolic pressure above 140 mm. rt. Art., an antihypertensive drug is taken daily, preferably at the same time, under constant monitoring of blood pressure, for life.
The first class of drugs is ACE inhibitors.
Drugs of this group became one of the first classes of drugs that effectively reduce the activity of the RAAS; their development began in the 60s of the last century [2]. Today they are included in the category of so-called “life-saving drugs” due to their proven ability to improve the prognosis of a number of cardiovascular and renal diseases [2].
ACE inhibitors: mechanism of action and effect
ACE inhibitors reduce the level of circulating angiotensin II by blocking the angiotensin-converting enzyme, which causes a complex pharmacological effect:
- antihypertensive;
- cardioprotective;
- angioprotective;
- antiatherosclerotic;
- anti-inflammatory.
When taking drugs from the ACE inhibitor group, carbohydrate metabolism also improves: tissue sensitivity to insulin increases and glucose metabolism improves.
Indications and properties
The spectrum of activity of ACE inhibitors allows their use in arterial hypertension, coronary heart disease, chronic heart failure, nephropathies and acute myocardial infarction [3].
ACE inhibitors belong to the group of antihypertensive drugs that specifically lower blood pressure and slow the progression of heart failure, which determines their widespread use in cardiology. Data from a review of 158,998 patients with hypertension showed that taking ACE inhibitors reduces mortality from all of the above causes. This is a significant advantage of ACE inhibitor drugs, including compared to angiotensin II blockers [4].
However, ACE inhibitors are still not able to completely prevent the conversion of angiotensin I to angiotensin II, since there are a number of other enzymes that successfully “replace” ACE. This is exactly how the enzymes chymase, elastase and cathepsin G work, for example [5]. When using ACE inhibitors, these substances are compensatory activated, and the blockade of the RAAS becomes incomplete. This is a significant drawback of ACE inhibitors.
What should I warn the client about?
Important!
During the consultation, it is appropriate to emphasize that drugs that block the activity of the RAAS - ACEIs and ARBs - with constant use, along with an antihypertensive effect, protect the heart and blood vessels, significantly reducing the incidence of cardiovascular accidents. This small note can serve as a convincing argument in favor of regular and disciplined use of such drugs, according to the instructions and recommendations of the doctor.
Arterial hypertension – lifelong medication use?
Perhaps the majority of patients seen by a cardiologist are patients with high blood pressure - arterial hypertension (AH). Some of them had their blood pressure rise for the first time due to a stressful situation, some have been taking medications for a long time, but, as a rule, few have a complete understanding of their disease, and most importantly, how to live with it correctly and effectively treat it .
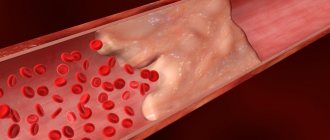
In a healthy person, blood pressure changes throughout the day depending on the level of stress (physical, mental, etc.), but in general these fluctuations do not exceed the so-called physiological norm, which supports the normal functioning of the body. For an adult, blood pressure is considered normal no higher than 140/90 mmHg. Art. And in some cases, for example, in the presence of diabetes mellitus, kidney disease, the pressure should be even lower at the level of 130/80 - 120/70 mm Hg. Art., which helps prevent the progression of these diseases and the development of complications. The state of the nervous system, heart and blood vessels plays an important role in maintaining blood pressure within optimal limits. With hypertension, the heart works overload, pumping an additional volume of blood. Over time, this leads to increased resistance from the vessels, which narrow under conditions of constant overload. The walls of the arteries thicken and harden, losing their elasticity. With the long-term existence of hypertension, the load on the vessels becomes unbearable, which can lead to degenerative changes in their wall, with the development of narrowing or pathological expansion, and even rupture of the vessel can occur. If this complication occurs in a vital organ (heart, brain), then it can result in myocardial infarction or cerebral hemorrhage (stroke) . But, despite this danger, the insidiousness of hypertension is that it can be completely asymptomatic for a long time.
The diagnosis of hypertension is usually not made after a single blood pressure measurement, unless the readings are too high, for example, over 170-180/105-110 mm Hg. Art. Typically, a series of measurements are taken over a period of time to completely eliminate random fluctuations and inaccuracies. It is also necessary to take into account the circumstances during which blood pressure measurements are taken. As a rule, blood pressure increases under stress, after drinking strong coffee or smoking a cigarette.
About 1/3 of the adult population has a persistent increase in blood pressure above 140/90 millimeters of mercury. 2/3 of those who suffer from hypertension do not know about their disease, and those who know often do not give it due importance (especially if the numbers are not so high, about 160/100 mm Hg), until headaches, heart pain, shortness of breath, arrhythmia, and swelling will not occur.
An interesting fact is that in a doctor’s office, when measuring blood pressure, the readings can be higher than at rest at home. This effect is called "white coat hypertension" and is caused by the patient's fear of the disease or the doctor. In addition to measuring blood pressure, the doctor usually checks for changes in other organs, especially if the pressure readings are at high levels.
If the blood pressure in an adult does not exceed 140/90 mm. rt. Art., then re-measurement is usually carried out no earlier than a year later. In patients whose blood pressure is between 140/90 and 160/100, repeated measurements are taken after a short period of time to confirm the diagnosis.
A high diastolic (bottom) pressure, such as 110 or 115 mmHg, indicates the need for immediate treatment.
Hypertension is one of the most common diseases. In developed countries, 10% of the adult population and about 60% of people over 65 years of age have high blood pressure. Unfortunately, no more than 30% of these people know about their illness, regularly receive therapy and follow the doctor’s recommendations. Unlike a number of diseases that you can “get over,” hypertension, as a rule, is a chronic, lifelong condition.
Arterial hypertension is most often primary in nature and is a symptom of hypertension. Less commonly, high blood pressure is secondary and is a sign of diseases of various organs (kidneys, blood vessels, etc.). Each of these diseases requires special treatment, which is why any increase in blood pressure requires consultation with a cardiologist.
In older people, a special type of hypertension sometimes occurs, so-called “isolated systolic hypertension.” In this case, systolic pressure readings are equal to or exceeding 140 mmHg, and diastolic pressure readings remain below 90 mmHg. This type of hypertension is a dangerous risk factor for the development of strokes and heart failure. Often, patients seek help only when the diastolic pressure, in their opinion, becomes too low - 50-60 mm Hg. Art. Sometimes this can be a sign of heart disease, but more often it is associated with age-related changes in the vascular wall, and it is very important to find drugs that will reduce the gap between systolic and diastolic pressure numbers, which in turn reduces the risk of stroke and heart failure .
In cases where routine and dietary measures do not allow adequate control of blood pressure, additional (and not instead) medications are prescribed. Today their list is quite impressive. Often, when a patient seeks help with complaints of high blood pressure despite taking prescribed medications, you can see that the medications were chosen correctly and are suitable for the patient for long-term use, but their dosages are inadequate. In cardiology, there is the concept of an effective dose - that is, one at which one can count on the manifestation of the desired effect. And if you take the same drug in halves or fours, and not just 2, but once a day, and often not even every day, then there is no need to talk about any hypotensive, much less therapeutic, effect of the drug. When prescribing one or more drugs, the cardiologist takes into account the level of blood pressure, the severity of hypertension, the individual daily blood pressure profile, the main risk factors or causes of arterial hypertension, the severity of target organ damage, the presence of concomitant diseases, and the interaction of drugs with each other and with other medications taken. , the possibility of developing side effects. Therefore, it is absolutely unacceptable for a patient to change doctor’s prescriptions, drug doses, frequency of administration, or discontinue one or another drug on their own. If, when taking a prescribed combination of antihypertensive drugs, the patient notices the occurrence of any side effects, the pressure does not decrease or, on the contrary, decreases excessively, it is necessary to discuss this with the attending physician, who, having understood the reasons, will adjust your prescriptions.
The role of the patient in the treatment of arterial hypertension cannot be underestimated. The effectiveness of treatment measures largely depends on how ready he is, in accordance with the doctor’s recommendations, to actively and consistently fight and, if possible, eliminate his risk factors. Dealing with risk factors means stopping smoking, limiting alcohol consumption, regularly taking recommended medications and monitoring their effect on blood pressure by recording measurements in a special diary.
Effective control of blood pressure should be considered if, as a result of lifestyle modifications, elimination of risk factors and bad habits, or taking antihypertensive drugs, it is possible to maintain blood pressure levels below 140/90 mmHg. Art., and for patients with diabetes mellitus, if possible, below 130/80 mmHg. Art. Achieving a target blood pressure level helps reduce the relative risk of developing fatal and non-fatal conditions/diseases, compared with patients who are not treated or are taking ineffective combinations. Each patient with hypertension needs to reduce excess weight, lead an active lifestyle, stop smoking, limit alcohol consumption (10 - 20 g for women, 20 - 30 for men in terms of pure ethanol), regularly take recommended medications and monitor their effect on blood pressure, enter blood pressure measurement data and other information necessary for the doctor in a special blood pressure self-monitoring diary.
If blood pressure exceed the specified level, then you should discuss with your doctor the possible reasons for the lack of effectiveness of the treatment. Among them:
- in blood pressure has not been identified
- Failure to comply with lifestyle modification recommendations
- Irregular use of antihypertensive drugs
- Inadequate antihypertensive therapy
As practice shows, if the patient trusts his doctor, with competent interaction between the doctor and the patient, in most cases it is possible to control this terrible disease.
What if you are already taking 3 or more medications and your blood pressure has not stabilized at your target level? This form of hypertension is classified as resistant.
Resistant hypertension is a condition in which blood pressure remains above target despite taking a combination of three or more antihypertensive drugs. Uncontrolled hypertension is not synonymous with resistant hypertension. Uncontrolled hypertension is caused by insufficient secondary control of blood pressure due to non-compliance with treatment regimen or true resistance to therapy. The criterion for refractory arterial hypertension is a decrease in systolic blood pressure by less than 15% and diastolic blood pressure by less than 10% from the initial level against the background of rational therapy using adequate doses of three or more antihypertensive drugs.
The lack of adequate blood pressure in more than 2/3 of patients is due to non-compliance with the treatment regimen - pseudo-refractoriness. Another most common and easily eliminated cause of this phenomenon is excessive consumption of table salt. Reasons that are much more difficult to cope with include obesity, alcohol abuse, the use of certain medications, breathing disorders and stopping during sleep, and kidney disease.
The following factors are associated with an increased risk of developing resistant hypertension: older age, high initial blood pressure, obesity, excessive consumption of table salt, chronic kidney disease, diabetes mellitus, left ventricular hypertrophy, female gender. The cause of true refractoriness in hypertension is volume overload associated with inadequate use of diuretics.
What's the solution?
Usually, in the case of resistant (refractory) hypertension, doctors continue to increase the doses of drugs taken by the patient to the maximum tolerated or add sequentially a fourth, fifth, and sometimes a sixth drug from other groups. Patients react to this differently. Many people stop trusting the doctor, some refuse to take medications altogether, because they do not notice any difference between their blood pressure while taking handfuls of medications and without them.
Of course, this decision is fundamentally wrong. In order to avoid progressive target organ damage and serious complications in the future, it is necessary to continue taking medications even if it is not possible to achieve the target blood pressure level. But no one will deny that the use of a multicomponent combination of drugs significantly increases the risk of side effects and unpredictable drug interactions.
What can modern medicine offer in this case? It turns out there is a way out.
Soon in our clinic we will be able to offer a non-surgical method for correcting blood pressure by denervation of the renal arteries. A new procedure, catheter-based renal denervation of the renal arteries, helps control high blood pressure by destroying some of the nerve fibers located in the wall of the renal arteries.
As often happens, the idea of denervation is not new, it is a well-forgotten old thing. Surgeons have long known that excision of the sympathetic nerve fibers responsible for maintaining blood pressure resulted in a decrease in blood pressure. But the procedure could not be used to treat hypertension, since it was accompanied by high operative mortality and long-term complications such as severe hypotension when moving to a vertical position, up to loss of consciousness, dysfunction of the intestines and pelvic organs. But this happens because the sympathetic stimulation of the kidneys and other organs is completely turned off, which leads to an imbalance of nervous regulation. Since the sympathetic nerve fibers innervating the kidney pass directly into the wall of the main renal artery and are adjacent to it, using catheter radiofrequency ablation (RFA) targeted destruction of fibers in the renal arteries will not lead to disruption of the innervation of the abdominal organs and lower extremities. In addition, by destroying only a small part of the nerve endings in the renal arteries, the kidneys are not deprived of nervous regulation. THE CAUSE OF RESISTANT HYPERTENSION IS EXCESSIVE SYMPATHETIC ACTIVITY OF THE KIDNEYS. And catheter RFA allows you to eliminate this excess activity. HYPERTENSION BECOME CONTROLLED.
The introduction of this procedure into our practice is based on a study published in the famous journal Lancet, which showed the safety and effectiveness of the technique, which allows us to achieve a lasting reduction in blood pressure up to 30 mm. rt. Art. from the initial level.
For this treatment, a radiofrequency catheter from Ardian is used, which is inserted through a puncture in the femoral artery. Next, the catheter is passed under X-ray control into the renal artery. Through the tip of the catheter, radiofrequency energy is dosed around the circumference at 4-5 points of the renal arteries. The procedure takes about 40 minutes, after which the catheter is removed. The patient's hospital stay is 24 hours. The condition for the procedure is normal kidney function. But the most striking thing about the procedure is that over time, the therapeutic effect not only does not decrease, but, on the contrary, the blood pressure of the majority gradually and steadily normalizes.
Currently, renal denervation is used only in patients with resistant hypertension. This should lead to approximately a 50% reduction in hypertension-related complications and mortality. This does not mean that medications are no longer needed. Patients will still likely need to take high blood pressure medications, but the number of medications needed to keep blood pressure at target levels will be significantly reduced.
What are the side effects of RFA of the renal arteries?
To date, no serious complications of catheter-based renal denervation have been reported worldwide. The procedure was accompanied by moderate abdominal pain, which was relieved by intravenous analgesics and sedatives. Only one patient had damage to the renal artery by the catheter before RFA, which was corrected by implantation of a stent. The most common complication in a small number of patients was pain and swelling in the groin area. No deterioration in renal function was noted.
Who needs renal denervation?
Denervation of the renal arteries
- Cost: 250,000 rub.
- Duration: 20-30 minutes
- Hospitalization: 1 day in hospital
More details
This intervention is indicated for patients with resistant hypertension, i.e. with a persistent increase in systolic (upper) blood pressure higher than 160 mm Hg. Art., despite the use of 3 or more antihypertensive drugs, including a diuretic. This is especially indicated if the combination of drugs is poorly tolerated or if there are side effects. In this case, patients must be preliminarily examined, and possible secondary causes of arterial hypertension (for example, diseases of the adrenal glands) must be reliably excluded. At the preliminary stage, it is necessary to conduct a computed tomography scan of the renal arteries to clarify the anatomical features of the vessels.
If you have high blood pressure , contact the cardiologists of our center. They will definitely help you.
ACE inhibitors: remember by name
Let's consider the features of some drugs - representatives of the ACE inhibitor group.
- Captopril is the first non-peptide ACEI, synthesized in 1975 [2]. The only tableted ACEI used to relieve hypertensive crisis. The dose is prescribed by the doctor (12.5–50 mg).
- Lisinopril is the only hydrophilic ACEI that does not accumulate in adipose tissue. Therefore, it is recommended for hypertension against the background of excess body weight and metabolic syndrome [2].
- Ramipril is an ACE inhibitor, which in a randomized trial demonstrated a significant reduction in overall mortality from CVD in high-risk patients by 16%, mortality from myocardial infarction by 20%, from stroke by 32%, and from chronic heart failure by 23% [ 6]. In addition, the incidence of new cases of diabetes while taking ramipril was 33% lower than in the placebo group [7].
- Fosinopril is an ACE inhibitor that is suitable for patients with hypertension due to severe renal failure, since it is eliminated in two interchangeable ways: through the liver and kidneys.
- Enalapril is the only ACEI that has a parenteral form (the active metabolite of enalapril is enalaprilat). Enalaprilat, like captopril, is used to relieve hypertensive crisis.
- Zofenopril is one of the most lipophilic ACE inhibitors. Due to its high lipophilicity, it easily penetrates into organs and tissues, showing a special affinity for the heart and blood vessels. It has a long-term anti-ischemic and cardioprotective effect, and exhibits an antioxidant effect [8].
- Spirapril has a long half-life, which provides a long-lasting and uniform antihypertensive effect. Does not require dose titration [9].
- Quinapril has high tissue specificity - it suppresses ACE in the plasma, lungs, kidneys, heart, and vascular walls. Improves the function of the vascular endothelium, providing an antiatherosclerotic effect [10].
How do diuretics work for hypertension?
The development of hypertension is based on a violation of the mechanisms of sodium excretion by the kidneys. When an increase in blood pressure occurs in the body, the excretory system tries to compensate for the imbalance by removing sodium ions and fluid to normalize physiological parameters. However, in hypertensive patients, compensatory mechanisms are impaired, so independent excretion of excess water occurs at maximum blood pressure values.
Diuretics lead to sodium imbalance
Diuretics have a pronounced therapeutic effect against high blood pressure due to diabetes mellitus. Since the pathology is characterized by increased susceptibility to sodium chloride, the result is an increase in the amount of fluid in the bloodstream, which is detected by an increase in blood pressure. For type 1 diabetes, preference is given to the thiazide group of drugs in minimal doses. Loop diuretics are used to relieve a hypertensive attack, but their long-term use is contraindicated. Some types of medications can worsen disturbances in glucose metabolism, which must be taken into account in the treatment of this category of patients.
The hypotensive effect of diuretic drugs is based on two mechanisms:
- Diuretic (increasing the daily amount of urine, as well as excretion of water and minerals).
- Non-diuretic (promotes the expansion of the vascular lumen by reducing the concentration of intracellular sodium ions).
The duration of the therapeutic effect is about 2–3 months, then the number of urinations decreases in parallel with the stabilization of heart contractions. This phenomenon is due to the inclusion of a compensatory mechanism that prevents fluid loss by increasing the concentration of renin and aldosterone in the blood.
Tolerability of ACE inhibitors
The subject of special attention of pervostolniks, as specialists dispensing the drug, is the side effects of ACE inhibitors. Despite the generally favorable safety profile, adverse reactions are the weak link of drugs in this group.
What should I warn the client about?
- While taking ACE inhibitors, a dry cough develops in 1–10% of cases [6]. Different members of the group practically do not differ from each other in their ability to cause it, and replacing one ACE inhibitor with another does not improve tolerability in this regard [11].
- When taking single-agent ACEIs, Quincke's edema can extremely rarely occur (but more often than when taking other antihypertensive drugs) [2]. It is believed that drugs in this group do not cause this complication, but alleviate its occurrence in predisposed patients. When releasing ACE inhibitors, it is appropriate to emphasize that if difficulty breathing and shortness of breath occur, you should immediately contact your doctor [11].
The cause of cough while taking ACE inhibitors has not been fully determined. It is assumed that the leading role is played by the accumulation of bradykinin in the bronchial mucosa, which is activated by blockade of angiotensin II [11].
Classification of diuretic drugs
Diuretic drugs are classified into:
- loop diuretics: furosemide, torsemide, ethacrynic acid;
- thiazide diuretics: hydrochlorothiazide;
- thiazide-like diuretics: indapamide, xipamide, chlorthalidone;
- potassium-sparing diuretics: spironolactone, eplerenone, triamterene, amiloride;
- osmotic diuretics: mannitol;
- carbonic anhydrase inhibitors: acetazolamide, brinzolamide, dorzolamide;
- xanthines: aminophylline (theophylline);
- diuretics of plant origin: erva woolly grass (half-fallen), orthosiphon staminate leaves, bearberry leaves, birch buds, horsetail grass, lingonberry leaves.
In addition, there are combination preparations of furosemide and spironolactone, as well as a combination preparation containing triamterene and hydrochlorothiazide.
The psychostimulant and analeptic caffeine sodium benzoate, as well as the cardiac glycoside digoxin, also have a diuretic effect.
The second class of drugs is angiotensin II receptor blockers.
Research that has focused on studying the possibilities of blocking the RAAS has led to the discovery of a group of drugs that do not have the classic disadvantage of ACE inhibitors - the side effect of cough. ARBs, or sartans, block the RAAS more completely, resulting in better tolerability than their predecessors. Despite their relatively recent introduction into clinical practice - sartans began to be used for long-term treatment of hypertension only in 1999 - representatives of this group have today become one of the most popular antihypertensive drugs [12].
Sartans: mechanism of action and effect
The pharmacological effect of sartans is identical to the effect of ACE inhibitors. Due to competitive blockade of angiotensin II receptors, they suppress vasoconstriction, aldosterone secretion, reduce myocardial hypertrophy, and also improve endothelial function.
The mechanism of action of ARBs is not the blockade of angiotensin-converting enzyme, as is the case with ACE inhibitors, but the blockade of angiotensin AT1 receptors, through which the vast majority of the physiological effects of angiotensin II are realized (vasoconstriction, etc.). AT1 receptors are located predominantly in vascular smooth muscle, heart, liver, adrenal cortex, kidneys, lungs and brain.
Over the past 10 years, drugs have appeared that some experts propose to separate into a separate, second generation of ARBs. They not only block AT1 receptors, but also help normalize carbohydrate and lipid metabolism.
Indications and properties
Sartans, like ACE inhibitors, are prescribed for a number of diseases, including arterial hypertension, chronic heart failure, previous myocardial infarction, diabetic nephropathy, atrial fibrillation and metabolic syndrome. In addition, ARBs become the drugs of choice in situations where cough develops while taking ACE inhibitors [13].
The effectiveness of sartans has been proven to significantly reduce blood pressure and have a cardioprotective effect [13, 14], as well as:
- reduce the incidence of myocardial infarction and stroke;
- reduce the frequency of hospitalizations due to chronic heart failure;
- reduce the severity of symptoms of CHF;
In addition, some ARBs, like ACEIs, reduce the likelihood of developing diabetes and exhibit nephroprotective effects.
New drugs are the safest
New generation medications for hypertension cause fewer side effects and are the safest.
Advantages:
- The composition includes active ingredients that reduce the negative effects on the body. At the same time, they do not lose their effectiveness.
- The effect of one tablet is enough for at least a day, because new generation drugs have a cumulative effect.
- The medications contain substances that have a positive effect on all organs and vital systems.
Individual representatives of sartans
Most sartans have similar properties and differ little from each other both in pharmacokinetic parameters and in hypotensive and cardioprotective activity. But still, some ARBs have features:
- Losartan, the first synthesized sartan, has a uricosuric effect, that is, it increases the excretion of uric acid. Therefore, it is advisable to use it for concomitant gout [4].
- Valsartan blocks, along with AT1 receptors, AT2 receptors located in blood vessels. Due to the blockade of the latter, the drug has a vasodilating effect [13].
- Telmisartan increases tissue sensitivity to insulin and enhances glucose utilization in muscles and tissues. At the dosages used for the treatment of hypertension, the drug acts similarly to hypoglycemic drugs - thiazolidinedione derivatives (pioglitazone, rosiglitazone). It is this drug that some experts consider to be a representative of the second generation sartans [13].
- Azilsartan medoxomil is a new sartan that binds more tightly to AT1 receptors compared to other ARBs, due to which it has a powerful and long-lasting antihypertensive effect that is superior to the effect of other sartans. The drug increases tissue sensitivity to insulin and affects the mass of adipose tissue, reducing it. The drug is promising for patients with hypertension and metabolic disorders [14].
- Fimasartan is another new ARB inhibitor developed by a Korean company. It is used only as an antihypertensive agent [15].
Indications for use
Diuretics are used for conditions associated with fluid retention in the body: edema due to diseases of the heart, kidneys, liver - heart failure, renal failure, cirrhosis of the liver. Osmotic and loop diuretics are also used for life-threatening edema - cerebral edema and pulmonary edema (when a quick and pronounced effect is needed).
Diuretics are used in the treatment of arterial hypertension (hypertension), as well as for increased intraocular pressure - glaucoma.
Osmotic and loop diuretics are prescribed for acute poisoning with water-soluble poisons - to accelerate the removal of toxins from the body, hypertensive crisis, as well as oliguria (reduced urination) for kidney injuries, large blood losses and burns.
Carbonic anhydrase inhibitors are also used in the complex treatment of epilepsy, as well as increased intracranial pressure, sleep apnea syndrome (breathing stops during sleep).
Thiazide diuretics are additionally used in the treatment of diabetes insipidus (deficiency of the posterior pituitary hormone vasopressin).
Diuretics of plant origin are also prescribed for inflammatory diseases of the kidneys and urinary tract (pyelonephritis, pyelitis, cystitis).