Antibiotics are not a toy for children
Uncontrolled and widespread use of antibiotics for all sorts of coughs or snot, it turns out, can lead to unexpected consequences.
Danil Sergeevich Simanovsky, a pediatrician and chief physician at the Osnova Children children's clinic, answers questions about antibiotics.
Why doesn't the doctor prescribe antibiotics if a child has a serious cold?
There is no diagnosis for the common cold. A cold usually means the presence of snot, cough, red throat or sore throat - what doctors call catarrhal phenomena. And all these phenomena can be caused by viral infections, or they can be bacterial. Depending on the etiology of the infection (what caused the infection), antibiotics are used or not.
Even if the snot, cough and red throat are quite strong and cause discomfort, but the infection is caused by a virus, then antibiotics are not prescribed due to their uselessness, because viruses are not sensitive to antibiotics. Antibiotics were invented and are used only against bacteria. Therefore, if your child is sick for a long time and seriously, and you have doubts: is it a common cold, you need to consult a doctor. The doctor will examine the child, determine the etiology of the infection, sometimes this requires additional tests: blood tests, smears. Only after this will he prescribe antibiotics if necessary.
If you have yellow or green mucus coming from your nose, is this a sign of a bacterial infection?
It is impossible to determine the etiology of the infection by the color of the snot. And everyone knows that green snot is scary, but white snot is not. This is not true, because the mucus that is secreted in the nasopharynx can take on color depending on the additional properties of the bacteria. Most often, snot gets its green color from viridans staphylococcus, which is a normal flora of the nasopharynx. Remember, the color of snot has no independent value.
Do I need to take a drug for intestinal microflora while taking antibiotics?
The microflora of the colon is very mobile, therefore, for a person without gastrointestinal diseases who is receiving treatment with an antibacterial drug according to the correct indications, the prescription of probiotics and eubiotics is not necessarily necessary. But the doctor always looks at the child, additional risks, age, and so on. As a rule, when taking antibiotics, we do not observe dysbiosis, but diarrhea, which is a side effect of antibiotics and goes away as soon as we finish this therapy. For example, the most common penicillin antibiotic in outpatient practice is amoxicillin, which is most often used in the treatment of otitis media, bronchitis, and tonsillitis. It contains clavulanic acid, which has a natural side effect - diarrhea, i.e. loose stool. If such a side effect occurs from an antibacterial drug, it is enough to take enterosorbent, but not simultaneously with antibiotics. Everything is at the doctor's discretion.
Can antibiotic resistance develop?
Of course it can, and we are very afraid of this. Therefore, the scientific and medical communities are struggling with polypharmacy - the prescription of too many drugs that are inadequate for the disease. It is also very important to combat parental self-prescription of antibiotics. Therefore, you don’t need to focus on the color, the smell of snot, or anything else. You need to follow the doctor's recommendations. If the recommendations seem unreasonable to you, you need to seek a second opinion. freepik.com
Read more about antibiotic resistance
Polyresistance is not the resistance of the child’s body itself to an antibiotic, but the resistance of microorganisms contained in the body. A colossal amount of viruses and bacteria are simultaneously present on the mucous membrane, and this is normal. Some of them are pathogenic, some are conditionally pathogenic, some are saprophytes, i.e. normal flora. For example, a large number of skin problems arise from the regular use of antibacterial agents. Not only because they dry the skin, but because they disrupt the normal biocenosis of the skin. The same thing happens when you constantly use antibacterial toothpaste or antibacterial gels for intimate hygiene. Our everyday behavior already increases the likelihood that microorganisms that live on mucous membranes and skin will develop resistance to these antibacterial agents. And when we need to cure some kind of infection, a situation may arise that the chosen drug will not work. In this case, you will have to choose other antibiotics with a wider spectrum of action in order to still defeat this infection. This is where the need to prescribe the correct dose arises. Don't give antibiotics for a couple of days just in case. Because when the dose of an antibiotic is too small, resistance develops: hostile microorganisms are not completely defeated: some die, but the surviving bacteria will already be resistant to this antibiotic. The duration of antibacterial therapy is an important factor. If it is not followed, the likelihood of developing antibiotic resistance increases.
How long does it take for antibiotics to work?
The question is different: the effectiveness of antibacterial therapy is assessed based on the results of 48-72 hours from the start of oral administration of the antibiotic. These hours must be counted from the moment of the first appointment. This does not mean that recovery occurs after 2-3 days, but there should be an improvement in both well-being and symptoms of the disease, which are assessed by the doctor during examination. There are diseases that, from the parents’ point of view, take an inappropriately long time to treat, for example, tonsillitis. The course of antibiotic treatment is 10 days. The child already feels good on the fourth day, he has no complaints, and the doctor insists on continuing to take the “harmful, terrible antibiotic that kills everything.” This is necessary to prevent bacteria from developing resistance and dying from antibiotics. When children come to the appointment for whom their parents have independently prescribed an antibiotic for a common ARVI, doctors choose the minimum course of medication. If we cancel them on the second or third day, we risk provoking resistance in the remaining microorganisms. And next time we will have to use an antibiotic that is heavier, broader and more harmful to the child.
One antibiotic helped the older child, why go to the doctor if the younger child can be given the same one?
If children suffer from the same infection, then most likely they will be helped by the same antibiotic. But, at a minimum, it is necessary to correctly determine the dosage of this antibiotic; perhaps your child needs an individually selected dosage. And we, doctors, have the opportunity to deviate a little from the dosages that are written in the annotations of medicines. Because the doctor, unlike the mother, also has regulations in the form of clinical recommendations for treatment. The dosage of the antibiotic will be different for the treatment of different diseases, so even though you have several children who were stereotypically ill, you will still need to consult a doctor.
Doesn't a cold often turn into a bacterial infection?
Why wait for this when you can take antibiotics right away? Firstly, it has been absolutely scientifically proven that taking antibiotics against the background of a viral infection does not reduce the likelihood of developing complications. If you start giving your child an antibiotic from the first day of a viral infection, the likelihood that this viral infection will develop complications does not decrease. Secondly, there is no such pattern that you start getting sick with a virus and continue to get sick with a bacteria. The thicker green snot that appears on days 4-6 of an acute respiratory viral infection does not mean that some hypothetical bacterial infection has occurred. No, this means that the snot stays in the nasopharynx longer and takes on the color of the microflora that prevails there.
Competent approach to prescribing medications
In any case, the doctor must follow two basic principles of antibacterial therapy:
- Rapid prescription of the most effective drugs in cases where their effect has been proven.
- Maximum reduction in the use of antibacterial drugs in all other cases.
Unfortunately, there are no reliable external signs or simple and cheap laboratory methods to distinguish between the viral and bacterial nature of respiratory tract infections. At the same time, it is known that acute rhinitis (runny nose) and acute bronchitis (inflammation of the bronchial mucosa) are almost always caused by viruses, and tonsillitis (inflammation of the tonsils and pharynx), acute otitis (inflammation of the ear) and sinusitis (inflammation of the mucous membrane of the paranasal sinuses) ) in a significant part of cases - bacteria.
It is natural to assume that approaches to antibacterial therapy for individual acute upper respiratory tract infections should be somewhat different.
Sources
- Anci E., Braun C., Marinosci A., Rodieux F., Midun E., Torres MJ., Caubet JC. Viral Infections and Cutaneous Drug-Related Eruptions. // Front Pharmacol - 2021 - Vol11 - NNULL - p.586407; PMID:33776753
- Lassi ZS., Padhani ZA., Das JK., Salam RA., Bhutta ZA. Antibiotic therapy versus no antibiotic therapy for children aged 2 to 59 months with WHO-defined non-severe pneumonia and wheeze. // Cochrane Database Syst Rev - 2021 - Vol1 - NNULL - p.CD009576; PMID:33469915
- Marusinec R., Kurowski KM., Amato HK., Saraiva-Garcia C., Loayza F., Salinas L., Trueba G., Graham JP. Caretaker knowledge, attitudes, and practices (KAP) and carriage of extended-spectrum beta-lactamase-producing E. coli (ESBL-EC) in children in Quito, Ecuador. // Antimicrob Resist Infect Control - 2021 - Vol10 - N1 - p.2; PMID:33407927
- Yousif MK. Mothers' false beliefs and myths associated with teething. // Qatar Med J - 2021 - Vol2020 - N2 - p.32; PMID:33329998
- Willems J., Hermans E., Schelstraete P., Depuydt P., De Cock P. Optimizing the Use of Antibiotic Agents in the Pediatric Intensive Care Unit: A Narrative Review. // Paediatr Drugs - 2021 - Vol23 - N1 - p.39-53; PMID:33174101
- Shahrin L., Chisti MJ., Shahid ASMSB., Rahman ASMMH., Islam MZ., Afroze F., Huq S., Ahmed T. Injectable Amoxicillin Versus Injectable Ampicillin Plus Gentamicin in the Treatment of Severe Pneumonia in Children Aged 2 to 59 Months: Protocol for an Open-Label Randomized Controlled Trial. // JMIR Res Protoc - 2021 - Vol9 - N11 - p.e17735; PMID:33136058
- De Wolf D., Genouw A., Standaert C., Victor A., Vanoverbeke N., De Groote K., Martens L. Endocarditis prophylaxis in daily practice of pediatricians and dentists in Flanders. // Eur J Pediatr - 2021 - Vol180 - N2 - p.397-405; PMID:32780192
- de Sá Almeida JS., de Oliveira Marre AT., Teixeira FL., Boente RF., Domingues RMCP., de Paula GR., Lobo LA. Lactoferrin and lactoferricin B reduce adhesion and biofilm formation in the intestinal symbionts Bacteroides fragilis and Bacteroides thetaiotaomicron. // Anaerobe - 2021 - Vol64 - NNULL - p.102232; PMID:32634470
- Basha GW., Woya AA., Tekile AK. Prevalence and risk factors of active trachoma among primary school children of Amhara Region, Northwest Ethiopia. // Indian J Ophthalmol - 2021 - Vol68 - N5 - p.750-754; PMID:32317440
Effect of probiotics
It is strictly necessary to accompany the intake of antibiotics with liquid active bifidobacteria Bifidum BAG. Prescribing a probiotic during antibiotic therapy is more justified than later.
When taking antibiotics, probiotics protect their own flora from side effects, preserve the composition and functions of the microflora, and prevent allergic reactions and antibiotic-associated diarrhea.
Bifidum BAG price is 90 rubles for one bottle with a large number of beneficial bifidobacteria, vitamins, amino acids and other useful substances.
Bifidum BAG 90 rubles is a small price for ten billion cells (10 in 10 = 10,000,000,000) of beneficial bacteria, each of which contributes to the overall healing effect of the human body.
Pneumonia
Photo: macniak / freepik.com
If pneumonia is diagnosed or there is serious suspicion of this pathology, the tactics of antibacterial therapy differ from the two previous cases.
Certain age groups of children are characterized by certain features of the predominant pathogens. Thus, under the age of 5-6 years, according to some researchers, up to 50% of cases of pneumonia can be caused by viruses. At an older age, the likelihood of the viral nature of pneumonia decreases significantly and the role of bacteria (pneumococci) in the development of pneumonia increases. However, in all age groups, pneumococcus is a common causative agent of this disease, which causes a severe course of the disease. That is why pneumonia is an absolute indication for antibiotic therapy .
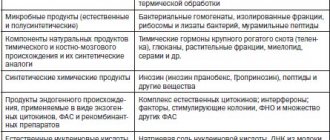
The main types of antibiotics and their common representatives on the market
Below we consider the most popular and frequently used groups of antibacterial agents:
- Beta-lactams . Among them are penicillins, cephalosporins, and carbapenems. Among the penicillins, it is worth highlighting: amoxicillin, ampicillin, ticarcillin, carbenicillin, mezlocillin, mecillam. The most popular cephalosporins are: cefazolin, cephalexin, cefuroxime, cefotaxime, ceftriaxone, cefepime, ceftobiprole. Carbapenems are used much less frequently. Meropenem can be isolated.
- Macrolides . Macrolides include: clarithromycin, azithromycin (sumamed), josamycin.
- Tetracyclines . The most common: tetracycline, doxycycline, oxytetracycline.
- Aminoglycosides . Popular ones: gentamicin, amikacin, isepamycin.
- Levomycetins . Trade names: chloramphenicol, chloromycetin.
- Glycopeptide antibiotics . The most commonly used: vancomycin, bleomycin.
- Lincosamides . Used in medicine: lincomycin, clindamycin.
- Fluoroquinolones . Among them, the most commonly used are: ciprofloxacin, levofloxacin, gemifloxacin. They are a broad-spectrum antibiotic for children. These antibiotics are not contraindicated in pediatric practice, but their use in children is sharply limited.
It is important to remember that these drugs have their own indications and contraindications, and are also used against certain infections.
These drugs have their own indications and contraindications, and have a narrow or broad spectrum of activity against bacteria. Some of the listed drugs can be used by children under one year of age. Children's antibiotics are available in tablets, suspensions, and ampoules for intravenous and intramuscular administration. Calculation of the dose, dilution of antibiotics and administration of the required dose to the child should be carried out by medical personnel in order to avoid unwanted reactions, as well as complications during injections. They should be prescribed exclusively by a doctor.