Getting rid of molluscum contagiosum is a very lengthy procedure. Few people manage to get rid of it in a short time. Many forums are full of messages about how difficult it was to remove it, what methods they tried and there was no result. But not everyone knows that two methods are effective in the fight against this disease: time or modern methods of removing shellfish in children.
Molluscum contagiosum in children
Molluscum contagiosum is more common in children than in adults. Children up to one year old practically do not get sick with molluscum contagiosum. This is due to the fact that in the first year of life the child’s circle of contacts is small: the child moves in a limited space, often specially prepared for him and under the strict supervision of adults, without trying to come into contact with other children. But as soon as a child begins to actively communicate and independently explore the world, the threat of becoming infected with molluscum contagiosum increases sharply.
The peak incidence of molluscum contagiosum in children occurs between the ages of 2 and 6 years. Immunity at this age is still weak. Children become infected through toys or dirty hands. The virus penetrates the skin in the place where the integrity of the skin is damaged - through wounds, abrasions, cracks. Children's skin is delicate and sensitive, and the activity of a preschool child is great. As a result, numerous microtraumas occur, opening the way for infection. Cases of infection with molluscum contagiosum while swimming in the pool have also been described.
From 6 to 10 years, the incidence of molluscum contagiosum decreases. Instilling household hygiene skills is of great importance. The sooner your child starts taking care of clean hands, the better.
At-risk groups
At risk are men (they get sick more often), as well as children (mainly under 4 years of age) - they account for up to 11% of all infections. In total, up to 22% of people in the world are infected with this virus, depending on where they live. The virus spreads best in warm and humid climates.
Elderly people with weakened immune systems, as well as patients with immunodeficiencies (for example, HIV) are also at risk. People who suffer from atopic dermatitis often get this disease.
Symptoms of molluscum contagiosum
The incubation period of the disease ranges from two weeks to several months, but most often the rash appears on the 14-15th day.
At first, single rashes appear, then there are more of them. Molluscum contagiosum can affect any area of the skin except the palms and soles. In children, exposed areas of the arms and legs, as well as the face and neck are most often affected. In adults, the genital area and the inner thighs are most often affected.
In the typical form of the disease, the rashes are located only in one anatomical area; in the generalized form, they spread throughout the body.
Rash
The elements of the rash look like protrusions (papules), firm and painless to the touch, pink or flesh-colored, with a pearlescent top. In the center of the papule there is a small depression, from which, when pressed, a white pasty mass is squeezed out. Papules have a round or oval shape, the size usually varies in the range of 2-5 mm, but sometimes the nodules merge, and then such formations can reach a diameter of 1 cm or more.
More about the symptom
Itching
In some cases, the rash is accompanied by itching, which intensifies when scratching. Under no circumstances should papules be scratched, as this can lead to a bacterial infection. The presence of a bacterial infection is indicated by redness of the skin around the papules, swelling, and suppuration.
More about the symptom
Introduction
Molluscum contagiosum is one of the most common diseases of the skin and mucous membranes of children and adolescents [1], less common in adults and occurs with the formation of small hemispherical papules with an umbilical depression in the center.
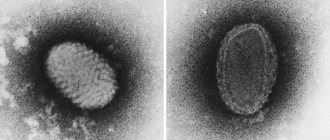
The disease is caused by an epidermotropic virus (Molluscum contagiosum virus), which belongs to the family of smallpox viruses (Poxviridae). When studying the genotype of this virus, four types of MCV-1–4 were identified, the most common of which is type I. The latter causes 96.6% of infections. Type II virus accounts for 3.4% of cases, but no relationship has been found between the type of virus and the morphology of the lesion or the anatomical distribution of the lesions [1]. Types III and IV viruses are rare and are more often verified in patients with immunodeficiency conditions [2]. Molluscum contagiosum rarely occurs in children under 1 year of age, but the main peak incidence occurs between the ages of 2 and 5 years and is associated with accidental direct contact with sick children or indirect transmission of infection through toys or household items. The method of infection of adolescents is explained by the activity of sexual contacts [3, 4]. Men get sick slightly more often than women. The prevalence of this disease has been little studied, but in recent years there has been an increase in incidence not only in Russia, but also in many countries of Europe and America [5]. It was found that in people with immunodeficiency conditions, the rashes are more profuse, and the incidence is much higher. It has been established that about 5–18% of all patients with immunodeficiency are susceptible to this virus, and the severity of the infection is inversely proportional to the number of CD4 lymphocytes [6]. In patients with various chronic skin diseases accompanied by dryness (for example, atopic dermatitis and eczema), the molluscum contagiosum virus is activated, sometimes causing a generalization of the process [5]. A more detailed clinical picture in terms of the number of rash elements, the area of affected skin and the persistence of the infection is also observed in patients receiving prednisone and methotrexate. In addition, cases of activation of the virus in the form of dissemination of molluscum contagiosum in the treatment of eczema, atopic dermatitis, and vitiligo with tacrolimus ointment 1% have been described [7, 8].
The pathogen is transmitted indirectly through bed and underwear, towels, dishes, toys, washcloths, during contact sports, massage, visiting the pool, taking public baths, or by direct contact during sexual intercourse among adults and adolescents [1, 9, 10] . The incubation period is usually 2–7 weeks, but can be extended to 6 months. This is because although viral particles are primarily localized to the stratum basale, viral DNA replication and the formation of new viral particles do not occur until the stratum spinosum and granular layers of the epidermis are involved. The molluscum contagiosum virus does not have a latency period and does not exist in the body constantly like the herpes virus. For the lack of formation of a persistent immune response, it is important that it produces virus-specific proteins that help it avoid aggression from the immune system. Thus, if after treatment the patient again develops lesions of molluscum contagiosum, it means that he has again come into contact with an infected person or object.
The rash can be found on any part of the skin, but in children, lesions of molluscum contagiosum usually appear on the chest, arms, torso, legs and face. Multiple elements may also develop in the axillary and groin areas. It is extremely rare to find single elements on the mucous membranes of the lips, eyelids, tongue and oral mucosa. In adults, molluscum contagiosum is most often limited to the perineum, genitals, lower abdomen, or buttocks.
Clinically, on unaltered skin, isolated hemispherical nodules with a pearly sheen are detected ranging in size from 1–3 to 5–10 mm in diameter, having the color of normal skin or pale pink, most often located in groups, but can also occur in the form of a single element. In the center of some elements there is an umbilical depression filled with horny masses. When opened and pressed, a whitish substance with a cheesy consistency, consisting of keratinized epidermal cells and ovoid bodies, is released from the central recess. As a rule, the rashes do not bother, but sometimes they can be accompanied by itching, an eczematous reaction, and due to injury, new lesions begin to appear, which leads to the spread of the disease. In clinical practice, it should also be taken into account that in 10% of patients with molluscum contagiosum, atypical rashes occur, for example, on the dorsal or lateral surfaces of the feet and hands; they most often look like dry hyperkeratotic nodules (Fig. 1), and in some cases on the lower thirds of the face and neck can imitate acneiform elements.
As long as the elements exist on the skin, the patient is considered infectious to others. The appearance of a pronounced inflammatory reaction of individual elements may indicate the subsequent elimination of the virus or its traumatization and subsequent spread. As a rule, the process proceeds without complications of the disease, but sometimes there may be complications such as the addition of a bacterial infection (requires the prescription of antibacterial drugs), scarring (more common with constant trauma to a number of elements or after insufficiently correct removal of elements), conjunctivitis or keratitis (if elements are present). on the face in the eye area). In the latter case, patients may experience pain, redness and swelling, as well as soreness, tearing and light sensitivity of the eyes. Another rare complication of molluscum contagiosum, erysipelas, occurs in patients infected with the human immunodeficiency virus [11]. The diagnosis of molluscum contagiosum is most often established by a simple examination of the skin; sometimes it is necessary to resort to dermatoscopy of the formations; in some cases, microscopy or even histological examination of the elements is performed.
Dermoscopy of molluscum contagiosum can reveal the following features (Fig. 2):
- a papule with a depression in the central area, in which orange or yellowish horny masses may also be observed;
- homogeneous whitish-pink globules in the central region (white when pressed firmly);
- multiple linear or convoluted vessels along the periphery of the lesion.
Differential diagnosis includes warts, papillomas, chickenpox, epidermal cyst, sebaceous gland hyperplasia, dermatofibromas, warty lichen planus, pyogenic granuloma, and in rare cases, skin cancer.
Treatment
Therapeutic options for treating molluscum contagiosum include the use of various external agents, mechanical methods, electrocoagulation, cryo- or laser removal, and oral medications. But often one therapy session is not enough due to insufficient activity of the drugs, relapse or the appearance of new elements.
Conservative treatment using various creams, ointments, solutions (imiquimod, retinoids, 5-10% solutions of potassium hydroxide, etc.) is not always effective and often helps only with single or small newly appeared elements. Spontaneous healing is extremely rare (with single elements) and occurs within a period of up to 18 months after appearance; isolated cases of self-resolution of elements within 4 years have been described.
In most cases, parents of children choose a wait-and-see approach and do not treat molluscum contagiosum, which most often leads to the spread of elements and infection of other people in the environment. Watchful waiting is especially dangerous for people with various immunodeficiency conditions, because... lost time can lead to a large-scale spread of the process with the subsequent need for general anesthesia to remove elements [11]. In some cases, experts suggest combining several methods during treatment, because It is not always possible to clear the skin of molluscum contagiosum using only one treatment method [12].
The most appropriate therapeutic approach depends largely on the clinical situation and extent of molluscum contagiosum. For healthy children, the main goal is to limit discomfort, trauma, and result in limited spread. For adults, who are most often ready for treatment, cryotherapy, electrocoagulation or curettage of individual elements are effective, and they tolerate them well.
In immunocompromised individuals, molluscum contagiosum rashes can be quite extensive and difficult to treat (Figure 3). The goal may be to treat the largest, irritated, or confluent lesions. In severe cases, these patients may require more aggressive laser destruction, antiviral therapy, or a combination of both [13]. Effective antiretroviral therapy for patients with acquired immunodeficiency syndrome makes therapy for molluscum contagiosum much more effective.
Topical drugs used in the treatment of the disease are listed below.
Potassium hydroxide (Molutrex 5%, Molusderm 10%) – a solution in the form of a solution. Used topically to treat molluscum contagiosum, it destroys skin cells infected with the virus, allowing the development of an adequate immune response. The solution is applied 2 times a day to each element, until signs of inflammation appear and the lesions resolve after this within several weeks. Treatment is interrupted for several weeks immediately when inflammation appears (Fig. 4, 5). If there are no signs of inflammation after use for 14 days, you should take a break and not use the drug. Side effects of these drugs include mild burning, redness, and itching, which usually go away within a few minutes after applying the drug to the skin [14, 15]. The Cochrane Database reviewed the results of studies that examined the effects of several topical, systemic and homeopathic remedies [16]. Among the findings, the researchers found no statistically significant differences between placebo treatment and potassium hydroxide therapy or between placebo treatment and various homeopathic remedies.
Podophyllotoxin (Condilin, Condiline Nycomed) in Russia is presented only in liquid form; a special stick is used for local application of the solution to the elements and dosing the solution onto the skin. When applied, there is often discomfort, which goes away quite quickly. Treatment must be applied for 3 days in a row, followed by a break of 4 days. The number of courses should not exceed five.
Imiquimod (Aldara, Keravort, Vartotsid) is a cream used to treat large areas or large accumulations of elements. The therapeutic effect of the drug is due to its stimulating effect on the immune system. The cream is applied 3 times a week at night and washed off in the morning after 6–10 hours. It takes several weeks of therapy to see results. Common side effects of imiquimod include skin flaking, severe crusting, redness and swelling, burning and itching sensations, and sometimes headaches. These complications usually resolve within 2 weeks after stopping treatment and do not require additional correction. It was later found that imiquimod is not effective as monotherapy for molluscum contagiosum and is used only in combination with other treatment methods [16–21].
Benzoyl peroxide (Baziron AS, Proderm, Desquam, Eclaran) - cream or gel. It is applied in a thin layer to the elements 1 or 2 times a day after showering or washing on dry, clean skin. Benzoyl peroxide may increase sensitivity to sunlight, so avoid excessive exposure to sunlight and ultraviolet light or use sunscreen. Side effects of benzoyl peroxide include redness and dryness, flaking of the skin, burning and itching where the drug is applied. Usually no additional treatments are required, the elements completely resolve on their own after completion of therapy.
Tretinoin (Retin-A, Vesanoid, Lokacid) is available in liquid and cream form, which are applied 1 or 2 times a day to individual elements. As with benzoyl peroxide, tretinoin may increase skin sensitivity to sunlight and ultraviolet radiation. The most common side effects of tretinoin are mild irritation and burning of the skin. It usually takes more than 2 weeks from the start of treatment to improvement. In cases where tretinoin is applied to large areas of the skin, it can cause severe eczematization and inflammation of the surrounding skin, which, on the contrary, can lead to autoculation (self-propagation).
Cantharidin is an irritant (low-molecular toxin), when applied to the skin after 2-5 hours it causes the formation of blisters, bubbles, and while they are intact, no pain is noted, but after opening, irritation, burning, and pain occur. Most often used in combination with imiquimod.
A number of studies have shown the high effectiveness of this combination. In this case, application to only a few elements is initially prescribed in order to check the patient’s response to therapy [22, 23]. Cantharidin is not approved by the US Food and Drug Administration, but has long been used by American dermatologists as a safe and effective drug [24, 25]. Various types of acids (bi- and trichloroacetic, salicylic, lactic, glycolic) are recommended to be used only under the supervision of a specialist, because self-application often leads to scarring and pigmentation (Fig. 3); in addition, many studies have shown that fairly high-percentage acid solutions are effective - from 15% [26].
Oral antiviral drugs (cidofovir, ritonavir). Presumably, antiviral drugs may interfere with the replication of the molluscum contagiosum virus. Due to their high cost, lengthy treatment regimen, and possible side effects, they are considered drugs of choice only for immunocompromised patients [27].
Some studies have shown that gradual removal of molluscum contagiosum is possible by taking cimetidine; it is possible to use it in children, because it is safe, painless and well tolerated, at the same time there is very little data on its use in molluscum contagiosum; in addition, the drug is intended primarily for the treatment of gastric ulcers and, as expected, its effect in infections caused by molluscum contagiosum is indirect due to the effect on the immune system.
In Russia, the permissible age for using this drug is 14 years, which makes its use in pediatric practice impossible [28].
The US Food and Drug Administration has not approved any topical or oral treatments for molluscum contagiosum.
Other treatments should always be performed by a qualified professional.
Cryotherapy involves freezing the lesions with liquid nitrogen to remove them. Each element is frozen within 5-10 seconds. Some authors successfully use cryodestruction to remove molluscum contagiosum [29]. It usually takes several cryotherapy sessions before all the elements are completely gone. And between procedures it is recommended to take a break of at least 10 days, more often 2-3 weeks, so this method can increase the treatment time.
Electrocoagulation (diathermocoagulation) uses heat to remove elements. Before removal, local anesthesia is used in the form of applications of solutions, creams or ointments or local injections with anesthetics (lidocaine, procaine or ultracaine). With extensive rashes, this method, like any other method of destruction, is painful even when using local anesthesia (Fig. 6, 7).
Mechanical removal is carried out with a sharp curette (small Volkmann spoon) or tweezers with blunt ends. After squeezing out, the lesions are treated with a 5% alcohol solution of iodine. As with electrocoagulation, local anesthesia is used before removal [30, 31].
Laser destruction is a relatively new type of treatment for molluscum contagiosum. During and after the procedure, discomfort in the removal area, burning, and change in skin color may be observed. These symptoms usually go away within a few weeks. Most often, one procedure is not enough [32–36].
Re-evaluation after any type of therapy is recommended after 2-4 weeks, and, as a rule, re-treatment is required. If elements do not respond well to one therapy or another, it is recommended to consider combination therapy with several methods [13]. Relapses occur in 35% of patients after initial clearance of all elements and may represent reinfection, exacerbation of ongoing disease, or new lesions occurring after a long incubation period.
As a result of the search for the most effective treatment for molluscum contagiosum in children, a prospective randomized trial was conducted that compared the effectiveness and side effects of four previously established treatments for molluscum contagiosum in 124 children [37]. In the first group, curettage was used, in the second - cantharidin, in the third - a combination of salicylic and lactic acids, in the fourth - imiquimod. It has been established that curettage is the most effective method of treatment, has the lowest level of side effects, but requires adequate anesthesia. Cantharidin is less effective, generally well tolerated, but has moderate complications in the form of blistering rashes. The combination of salicylic and lactic acids causes too much irritation and is therefore poorly tolerated by pediatric patients. Imiquimod did not show any effectiveness against molluscum contagiosum as monotherapy and is not recommended for use by the study authors.
Conclusion
Based on the review of existing treatment methods, the following conclusions can be drawn:
- Curettage, or mechanical removal of molluscum contagiosum, is most effective for all age groups of patients, and is well tolerated with adequate local anesthesia.
- For patients with immunodeficiencies, a combination of methods is recommended, most often laser removal in parallel with adequate antiviral therapy.
- None of the methods of external therapy have shown reliable results compared to placebo, but can be used as a trial option, especially if the patients themselves and/or their parents categorically refuse mechanical removal, so as not to provoke the appearance of new elements, or for treating small only emerging elements with a diameter of up to 2 mm, which do not yet have caseous contents.
- Waiting tactics are not justified, because Most often, the elements spread by autoaccumulation of the virus to other areas of the skin due to trauma and friction.
Methods for diagnosing molluscum contagiosum
Molluscum contagiosum can be confused with manifestations of other diseases, including serious ones such as syphilis or cancer. Also, the activity of the molluscum contagiosum virus increases with a decrease in immunity, so in 20% of cases molluscum contagiosum accompanies HIV infection. This means that when rashes appear that correspond to the description of molluscum contagiosum, a medical examination is required to rule out such options.
When contacting a dermatologist, the doctor will examine the patient, make a diagnosis and suggest a treatment method.
Inspection
In most cases, the diagnosis of molluscum contagiosum is made by a dermatologist based on the results of an examination of the patient.
PCR diagnostics
Since HIV often accompanies molluscum contagiosum, PCR diagnostics for HIV can be prescribed.
More information about the diagnostic method
Serological blood test
When molluscum contagiosum is detected in adults, a serological blood test is prescribed to identify sexually transmitted infections (hepatitis B and C, HIV, syphilis, etc.).
More information about the diagnostic method
Sign up for diagnostics To accurately diagnose the disease, make an appointment with specialists from the Family Doctor network.
Transmission routes
To protect yourself as much as possible, you need to know which routes of transmission of molluscum contagiosum are common. In this case it is:
- Household contact with a sick person or with contaminated things. Usually these are the patient’s personal belongings - for example, a towel.
- Sexual contact with an infected person. Often the rashes are localized on the genitals, lower abdomen and inner thighs.
- Transmission from mother to child. This is not a common option, but it is still possible.
- Infection during the tattooing process occurs in situations where the instruments are unsterile and the artist does not follow safety rules.
If there is a person with such an infection in your immediate environment, you need to be very careful, since the routes of transmission of molluscum contagiosum are quite simple.
Treatment methods for molluscum contagiosum
Molluscum contagiosum should be treated by a doctor. You should not try to remove papules yourself - this can lead to bacterial infection.
Treatment of molluscum contagiosum depends on a number of factors, primarily on the stage of development of the disease, the severity of symptoms and the state of the patient’s immunity. The following methods can be used:
Instrumental removal
Papules can be removed instrumentally, followed by treating the wound with antibacterial agents.
Credestruction
Cryodestruction is the removal of papules using exposure to low temperatures. Papules are treated with liquid nitrogen. Tissues treated in this way freeze and die.
Radio wave removal
Molluscum contagiosum papules can be removed using the radio wave method (using the Surgitron apparatus) and using a laser.
Electrocoagulation
Electrocoagulation is the effect of high-frequency current on papules. It is popularly described as “cauterization with electricity.” At the moment of discharge, a local strong thermal effect occurs, the tissues coagulate, which virtually eliminates the risk of infection at the treatment site.
Conservative treatment
The course of treatment for molluscum contagiosum may include conservative treatment with ointments and creams, as well as taking antiviral drugs (if the affected area is large).
Make an appointment Do not self-medicate. Contact our specialists who will correctly diagnose and prescribe treatment.
Rate how useful the material was
thank you for rating