General information
Epidermolysis bullosa (abbr. EB) is a concept that unites a whole group of rare hereditary diseases that have genetic and clinical heterogeneity. Most often, pathological processes occur in keratinocytes and lead to the formation of blisters with a benign course, the appearance of erosive areas of the skin and mucous membranes, increased vulnerability and sensitivity of the skin to any minor mechanical trauma, and the development of “ mechanobullous disease ,” also called Butterfly syndrome . The occurrence of different types of pemphigus is only 1 case per 30-100 thousand people.
The concept of epidermolysis bullosa was introduced by the German dermatologist Heinrich Koebner back in 1886, although similar cases of skin diseases had been encountered earlier.
Life expectancy with epidermolysis bullosa
Despite the rapid development of global medicine, the life expectancy of patients with congenital epidermolysis – “butterfly children” – is most often not high. It all depends on the subtype of the disease, the depth and extent of the pathological lesions. With proper care and complex therapy, simple emidermolysis bullosa is easier, the number of blisters is minimized with age, and the prognosis for such patients is favorable. Other types of genodermatous disease, especially with the addition of infections, most often staphylococcal or streptococcal, with the development of systemic complications and sepsis most often lead to death in the early years of children's lives.
Treatment
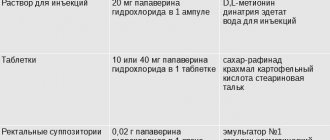
According to DEBRA, there are the following directions in the treatment of epidermolysis bullosa. 1. Protein therapy – a sufficient amount of normal protein is introduced into the patient’s body. Correction of clinical manifestations is carried out by intradermal injection of type 7 collagen. 2. Gene therapy – a gene encoding a damaged protein is introduced. This method is carried out by transplanting a piece of skin with a corrected gene - transgene (introduced missing gene). 3. Cell therapy - the necessary and sufficient number of cells containing a normal gene encoding a protein is introduced. With this method of treatment, fibroblasts from a healthy donor are injected into selected areas of the skin. Fibroblasts synthesize sufficient amounts of collagen to ensure the connection of the layers of skin (epidermis and dermis). 4. Combination therapy – “hybrid” skin grafts are created using donor fibroblasts and keratinocytes from the patient. This combination is used, because fibroblasts are less likely to cause graft rejection. 5. Therapy using bone marrow stem cells – two main directions can be distinguished in this area. First, the systematic introduction of donor bone marrow stem cells to the recipient. Second, reprogramming the patient's own skin cells to produce a new source of genetically corrected stem cells. 6. Drug therapy - includes the following areas: • “Knockout and replacement” siRNA (messenger RNA) • Drugs that prevent premature termination of gene expression (PTC124, or gentamicin). Some genetic defects in epidermolysis bullosa cause the protein synthesis mechanism in skin cells to stop working before the synthesis of complete protein is completed. These drugs prevent premature recognition of the stop signal by the protein synthesis mechanism, thereby prolonging the translation process. • Symptomatic therapy – includes the use of analgesics, antibiotics of various spectrums, antianemic drugs, selenium and carnitine preparations (for cardiomyopathy), etc.
Pathogenesis
The pathology is detected from birth - on the skin there are blistering formations with serological contents, which, when opened after about 2-3 days, leave long-term non-healing erosions, most often leading to the development of atrophic scar tissue, hyper- or hypokeratosis , and re-development of blisters. There are known cases of the disease manifesting itself at a later age - in infancy, early childhood and even adolescence.
Skin damage - the occurrence of ulcers and blisters is caused by any mechanical impact, so the areas with the most frequent friction - the armpits and various folds, the places where clothes and straps fit - are the most affected.
The pathology is based on mutations in genes encoding proteins of various layers of the skin - basement membranes, dermis. In this case, an imbalance occurs in the system of enzymes and inhibitors, proteins become the target of attack by the body’s defense systems - enzymatic cytolysis, causing swelling of the cytoplasm , rupture of cell membranes and, as a result, disruption of intercellular connections, the structure of the epidermis with the formation of intra- or subepidermal bullae and vesicles.
Classification
Studying at the ultrastructural level the morphology of the skin (the number, types of skin structures such as keratin , desmosomes, hemidesmosomes, anchor threads, anchor fibers, etc.) and the localization of vesicular formations in the layers of the epidermis. There are three main types of epidermolysis mechanobullosa, which are divided into more than 30 subtypes depending on the phenotypic and genetic characteristics of the patients, as well as the type of inheritance:
- The simple type ( epidermolytic according to the Pearson classification of 1962) is the most common, occurs in 75% of cases and is characterized by the formation of blisters in the upper layers of the epidermis on the skin of the feet, hands, and in severe cases, the whole body. Divided into 2 main subtypes : suprabasal , in which the target proteins are plakophilin-1 , desmoplactin , etc., as well as the basal subtype, which causes changes in the structure of alpha-6/beta-4 integrin , and skin disorders can be localized, generalized (blisters occur in groups) and in the form of patchy pigmentation. The most common clinical forms are lethal acantholytic, superficial, with muscular dystrophy, with pyloric atresia, Ognassian, migratory annular , etc.
- The borderline type ( lucidolytic ) leads to the formation of blisters in the area of the light plate of the basement membrane and occurs in the form of the Herlitz subtype , which disrupts the structure of laminins 332 and 5 , as well as other subtypes involving not only laminins, but also collagen type XVII and α alpha-6 /beta-4 –integrin. In addition, there is a clinical form of inversion , with a late onset, in the form of laryngo-onycho-cutaneous syndrome .
- Dystrophic type ( dermolytic ) - affects the upper part of the papillary layer of the dermis, which comes in dominant and recessive subtypes and develops due to disruption of the structure of type 4 collagen. It can be generalized, peripheral, pretibial, centripetal, pruriginous , affecting only the nails, inverse .
- Kindler syndrome is considered a separate form, the rarest and least studied , since blisters can form in different layers of the epidermis and this is caused by a violation of the structure of proteins - kindlin-1 . They are detected immediately at the birth of a child, most often on the skin of the hands and feet. As a consequence, the occurrence of dystrophic changes in the nails, the development of caries , periodontitis , various diseases of the oral cavity, gastrointestinal tract, eye membranes, and genitourinary system may occur. With age, the number of newly formed blisters decreases, but the skin still remains thin, easily vulnerable, sensitive, the capillary network is located too close to the surface of the epidermis.
Clinical manifestations of BE
Epidermolysis bullosa manifests itself already during childbirth: the baby’s skin is injured when he passes through the birth canal. The nose, chin and heels are usually affected. In rare cases, the disease makes itself felt at 1-6 months of life. With age, depending on the type of EB, new symptoms of the disease may appear.
The main clinical manifestations of epidermolysis bullosa are blisters on the skin that appear at sites of friction, bruise, pressure, with increased body temperature, the environment, or spontaneously. Blistering can also occur on the mucous membranes of any organ. Most often the mucous membrane of the oral cavity, esophagus, intestines, genitourinary system, and eye mucosa are affected.
Causes of epidermolysis bullosa
The main causes of the pathology are mutations in more than 10 genes responsible for encoding proteins of various layers of the skin, most often in 75% - these are the genes KRT5 and 14, LAMC2, LAMA3, LAMB3, COL17A1. As the online resource Wikipedia indicates, for almost each of the established subtypes of EB, it was possible to identify mutations in certain genes, among them the most common are:
- missense point mutations;
- nonsense point mutations;
- deletions and insertions – losses and, accordingly, insertions of chromosome sections;
- frameshift mutations;
- splicing.
The type of inheritance of epidermolysis bullosa occurs as autosomal recessive (most often), autosomal dominant, and uniparental disomy, and somatic mosaicism .
Factors provoking congenital epidermolysis bullosa
Congenital Butterfly syndrome can develop even in healthy parents who do not carry mutated genes. Spontaneous mutations occur in utero and are caused by:
- bad habits of a pregnant woman - smoking, alcohol abuse;
- chaotic use of medications and other teratogenic factors.
Literature
- Boeira V., Souza E., Rocha B., Oliveira P., Oliveira M., Rêgo V., Follador V. (2013). Inherited epidermolysis bullosa: clinical and therapeutic aspects. An. Bras. Dermatol. 88 (2), 185–198;
- Fine J. D. (2010). Inherited epidermolysis bullosa. Orphanet. J. Rare Dis. 5, 12;
- Shinkuma S. (2015). Dystrophic epidermolysis bullosa: a review. Clin. Cosmet. Investig. Dermatol. 8, 275–284;
- Albanova V.I., Chikin V.V., Epishev R.V. (2014). On the issue of diagnosing congenital epidermolysis bullosa. Bulletin of dermatology and venereology. 3, 53–59;
- Bruckner-Tuderman L., McGrath J. A., Robinson E. C., Uitto J. (2013). Progress in epidermolysis bullosa research: summary of DEBRA International Research Conference 2012. J. Invest. Dermatol. 133, 2121–2126;
- Soro L., Bartus C., Purcell S. (2015). Recessive dystrophic epidermolysis bullosa. A Review of disease pathogenesis and update on future therapies. J. Clin. Aesthet. Dermatol. 8 (5), 41–46;
- Murauer E.M., Koller U., Pellegrini G., De Luca M., Bauer J.W. (2015). Advances in gene/cell therapy in epidermolysis bullosa. Keio J. Med. 64 (2), 21–25;
- Shouldn't we try to… change the genome?;
- CRISPR systems: immunization of prokaryotes;
- Mutagenic chain reaction: genome editing on the verge of science fiction;
- Kiritsi D., Garcia M., Brander R., Has C., Meijer R., Jose Escámez M. et al. (2014). Mechanisms of natural gene therapy in dystrophic epidermolysis bullosa. J. Invest. Dermatol. 134 (8), 2097–2104..
Symptoms
Symptoms of epidermolysis bullosa are associated with a violation of the structure of keratinocytes and manifest as:
- burning, pain in the affected areas and relief when emptying the blisters;
- itching during the healing of opened blisters - peeling off of the dried cap of the vesicle, which can subsequently cause peeling and pigmentation;
- development of skin areas with erosion;
- increasing the sensitivity and vulnerability of the skin to any mechanical damage;
- spontaneous occurrence of tense blisters containing clear, colorless liquid or hemorrhagic contents.
The pathology is usually detected immediately at birth, because thin and “brittle” skin is easily injured even from passing through the birth canal. Moreover, skin lesions have varying degrees of severity and prevalence, even within a family. Multiple widespread blisters can cause death in a newborn, especially if a secondary infection occurs. Exacerbations usually occur in the summer - warm season; with age, the prevalence of blisters is minimized.
Additional symptoms of simple EB
Simple epidermolytic lesions usually occur on the hands and feet or may cover the entire body. In addition, you may experience:
- development of palmoplantar hyperkeratosis of a widespread or confluent type;
- dystrophic changes in the nail plates;
- laryngeal stenosis;
- milia;
- hyper- or hypopigmentation ;
- growth retardation.
Healing of blisters most often occurs without scarring, sometimes even reminiscent of herpes simplex, but the likelihood of relapse is very high.
Epidermolysis bullosa simplex
Features of the course of borderline EB
This type is characterized by the development of a pathognomonic symptom - the appearance of areas of abundant granulation tissue on various parts of the body (as in the photo of borderline epidermolysis bullosa), for example, localized symmetrically around the mouth, in the middle part of the face, around the nose, on the upper back, in the armpits or nail folds. The pathology can lead to onychodystrophy and even complete loss of nail plates, a large number of milia , serious scars on the body, including cicatricial alopecia , crusts on the skin, oral ulcers, enamel hypoplasia and severe dental caries. Possible systemic complications usually include polyetiological anemia , growth retardation, erosion, vesicular skin rashes and detachment, and strictures in the gastrointestinal tract. The risk of their development increases depending on the area, degree of destructiveness and depth of skin lesions.
Borderline epidermolysis bullosa
Borderline epidermolysis bullosa is characterized by extremely high mortality, mainly in the first years of life, caused by cessation of weight gain, sepsis, pneumonia , or obstruction of the trachea and larynx.
Extracutaneous manifestations of dystrophic EB
In addition to generalized skin lesions - recurrent formation of blisters, erosions, milia, atrophic scarring and loss of nails, “Butterfly syndrome” causes:
- disorders of the gastrointestinal tract;
- damage to the genitourinary tract and outer eye membranes;
- chronic anemia;
- osteoporosis;
- growth retardation;
- compaction, degeneration and even loss of nail plates;
- contractures of various joints of the limbs - elbow, knee, wrist, metatarsal-tarsal, metatarsophalangeal, etc.;
- increased risk of developing neoplasms, for example, aggressive squamous cell carcinoma .
Dystrophic epidermolysis bullosa
Tests and diagnostics
The greatest importance in making a diagnosis is played by a biopsy - the examination of skin samples using transmission electron microscopes, which allow visualization and semi-quantitative analysis of various structures of the epidermis. Due to the availability of monoclonal and polyclonal antibodies against proteins of different layers of the epidermis involved in the pathogenesis of epidermolysis bullosa, immunohistological methods are gaining increasing popularity today.
The immunohistochemical research method and the method of indirect immunofluorescence make it possible to determine the state of expression of structural proteins with hereditary defects in skin cells - keratinocytes and basement membranes (the basis of the epithelium, which performs a barrier and trophic function), as well as the distribution pattern of proteins in previously formed or artificially provoked blisters, including number - their localization depth.
Thanks to modern DNA diagnostic methods, it is possible to quickly classify the type of pathology, identify structural proteins that have undergone mutation, and make a clinical prognosis. An innovative method of genetic analysis - direct sequencing - makes it possible to identify mutations, their type and location, and reliably confirm the diagnosis.
In addition, an important role is played by collecting a family history and medical history of the patient, a comprehensive examination of the whole body, and conducting laboratory tests.
Discussion
The diagnosis of VBE in Russia is mainly established on the basis of anamnesis and clinical picture, as in the cases described by us. The disease is included in the orphan list, and patients need to be provided with dressings, medications, medical nutrition products and the creation of special conditions at home, which requires high material costs. However, the implementation of these measures, due to the lack of statistical records of patients with VBE, complicates the provision of targeted assistance. At the same time, auxiliary laboratory diagnostic methods - transmission electron microscopy and immunofluorescence antigen mapping are absent in most regions, which makes it difficult to identify the type of VEB and predict the life expectancy of an individual and the future medical care he will need from specialists in various fields. To provide them with regular and complete palliative care, it is advisable to train mothers in caring for such patients during inpatient treatment. A full-scale registry and clinical surveillance, as well as an algorithm for their routing in the region, will improve the quality of life of these patients. These issues need to be addressed.
The authors declare no conflict of interest.
In children
Children diagnosed with epidermolysis bullosa are called butterflies because their skin is so vulnerable, delicate and unprotected like the wings of these insects.
The main way to protect your future child from this diagnosis is responsible family planning and genetic testing. Do not forget about the importance of screening, which can identify abnormalities in fetal development. For example, it is important to undergo prenatal diagnosis of pemphigus simplex, which can be detected in the second trimester of pregnancy by the high content of fetoprotein in the blood serum.
Diet for epidermolysis bullosa
Diet 15 table
- Efficacy: therapeutic effect after 2 weeks
- Timing: constantly
- Cost of food: 1600-1800 rubles per week
Regardless of the patient’s age and type of pathology, the therapeutic diet must fully compensate for the loss of proteins, salts, and fluids that are caused by pathological changes in the external integument and internal systems. When it comes to infants, the most recommended is breast milk, supplemented with protein foods - at least 20%. Nutrition should be fractional, mechanically, thermally and chemically sparing, and should be eaten in small portions. With age, the diet should include:
- non-acidic fruit juices and purees;
- add unrefined vegetable oil to breakfast to facilitate bowel movements and provide healthy fats;
- vegetables rich in plant fiber, for example, cabbage, zucchini, dried fruits, beets, which are best consumed mashed and boiled.
Caramel and candies, sweets, cookies, alcoholic drinks, hot and spicy foods - any food that can provoke the formation of bullous lesions in the esophagus and other parts of the gastrointestinal tract are strictly prohibited.