Home » Department of Orthopedics » Diseases » Chest deformity
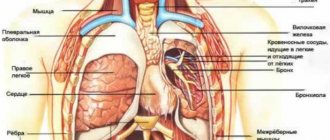
The chest is a part of the human body. It is formed in front by the sternum, behind by the spine, on the sides and partially in front and behind by the ribs. It is also formed by muscles that connect these bones to each other and to other bones. The rib cage contains the chest cavity, which contains the most important organs of the human body.
The chest contains the lungs and heart, as well as the aorta , the largest artery in the body. If these organs stop functioning, the person dies within a few minutes. That is why, during evolution, they settled in such a protected place. Due to the rigidity of the chest, the organs inside it are in a constant position, which ensures the stability of their functioning.
However, in some cases the chest changes its shape. Depending on the degree of change in shape, the position of the organs inside changes, their transformation occurs as they adapt to changing conditions. It should be noted that the chest is deformed, in most cases, in children, or is completely congenital. And with intensive growth, changes occur very quickly. This can lead to serious consequences for the entire body.
Types of chest deformation
Chest deformities can be divided into two groups.
- Congenital - usually caused by a violation of skeletal development in the prenatal period (changes in the shape of bones, absence of elements of the chest walls): - funnel-shaped deformity of the chest; – keeled chest deformity; – flat chest deformity.
- acquired (more common) - are the consequences of injuries, lung diseases, bone tuberculosis, rickets, scoliosis: - emphysematous; – paralytic; – scaphoid; – kyphoscoliotic.
How can parents find out if their child has a congenital chest pathology?
Ryzhikov Dmitry Vladimirovich
Ryzhikov Dmitry Vladimirovich (Head of the Department of General Bone Pathology of the Federal State Budgetary Institution "National Medical Research Center for Pediatric Traumatology and Orthopedics named after G.I. Turner, Candidate of Medical Sciences, doctor of the highest qualification category, traumatologist-orthopedist)Most often, parents learn about a child’s disease in preschool or school age by accidentally noticing asymmetry or an unusual shape of the chest. This situation is noticed more quickly in families where a similar pathology was previously identified in other family members.
The disease progresses while the skeleton is growing, that is, on average until 15-17 years of age. (more about the causes - types and types of deformations)
Our center actively provides telemedicine consultations in Doctor/Doctor mode. For additional information about the work of the Telemedicine Center NMIC DTO named after. G.I. You can contact Turner by writing to us at [email protected]
For patients from regions of the Russian Federation, there is the possibility of correspondence consultation.
Congenital chest deformities
The reliable causes of congenital chest deformity are currently unknown. However, any teratogenic factors negatively affect the development of the fetus in the womb.
The causes of congenital deformity are currently divided into three groups.
As a rule, with the development of deformation, a combination of these is observed.
- Uneven growth of costal cartilage and sternum.
- Pathology on the part of the diaphragm - too short parts of this muscle are able to “pull” the developing sternum inward.
- Developmental pathology of connective tissue and cartilage.
Funnel chest deformity
Deformation of the chest, manifested in retraction of the sternum, anterior ribs and costal cartilages. It occurs more often than other congenital malformations of the chest. You can also find its name as “ shoemaker's breast ”. Previously, shoemakers, when working, rested the heel of their shoes on the lower third of the sternum. This led to professional deformation of the chest.
Similar pathologies are often observed in the patient’s relatives, which indicates the genetic nature of this pathology.
A deformed chest is the cause of other diseases. As the child actively grows, the shape of other bones, in particular the spine, changes. There is also a change in position and disruption of the functioning of internal organs.
There are three degrees of pectus excavatum:
- I – depth of depression up to 2 cm, organs are not displaced;
- II – funnel 2-4 cm. deep, the heart is displaced up to 3 mm;
- III – depression more than 4 cm, heart displaced more than 3 mm.
Symptoms
At first, the violation is hardly noticeable. As the child grows, a “funnel” forms. Children lag behind their peers in development and suffer more often from colds. The deformation reaches its maximum by 3-4 years. Afterwards it gradually stops progressing. By this time, the child additionally develops kyphosis and scoliosis, disorders of the chest organs, asymmetry of the chest develop, and decreased excursion of the chest is noted.
Pileated chest deformity
The pathology is a protrusion of the sternum forward, which gives the breast cell a keel shape. Protrusion is caused by excessive growth of costal cartilages, which “push” the sternum forward, increasing the anteroposterior size of the chest.
There are three degrees of severity of deformation:
- I – protrusion of the keel up to 2 cm above the normal contours of the chest;
- II – protrusion from 2 to 4 cm;
- III – protrusion from 4 to 6 cm.
Symptoms
The main symptom is protrusion of the sternum forward. The degree of deformation increases with age. Unlike the previous pathology, keeled breasts do not cause serious problems. This is explained by the fact that the volume of the chest does not decrease and compression of the internal organs does not occur. The position of the heart changes. It occupies a vertical position and takes the shape of a “hanging drop”. The child complains of shortness of breath and fatigue.
Medical Internet conferences
The shape and size of the chest were subject to significant individual variations. In 20 corpses of men in the first period of adulthood (12.2%), the proportionality index is 47-51. In 10 study subjects (6.1%), this figure is 42-46; 5 (3%) – 52-56; in 2 corpses of men in the first period of adulthood (1.2%), the proportionality index is 37-41; in 1 male corpse this figure is 65. In the second period of adulthood, the proportionality index in 28 male corpses (17.1%) is 47-51; in 10 (6.1%) – 42-46, in 7 (4.3%) – 52-56, in 3 (1.8%) – 57-61, in 1 male corpse (0.6%) it is equal to 38 and in another 1 (0.6%) – 66. Thus, in men of both the first and second periods of adulthood in our study, the proportionality index prevails, equal to 47-51 (20 and 28 cases), which is slightly lower normative indicator of the proportionality index (50-55). With approximately the same frequency, an even lower proportionality index occurs, ranging from 42 to 46 (10 observations each in the first and second periods of adulthood). Thus, in the sample of male research subjects, a predominantly low proportionality index is recorded, which indicates their relative broad chest. In female corpses in both age periods, the proportionality index of 52-56 prevails, which was recorded in 13 cases (7.9%) in the first period of adulthood and in 16 cases (9.8%) in the second period. Relative broad-breastedness (proportionality index 47-51) was noted in 6 corpses of women in the first period of adulthood (3.7%) and in 13 (7.9%) in the second period. We identified relative narrow-chest (proportionality index 57-68) in 12 corpses of women in the first period of adulthood (7.3%) and in 11 (6.9%) in the second period.
Table 2 contains an analysis of the ratio of study objects according to the Charpy angle indicator. According to the table, we can conclude that in 54 corpses of mature people (32.9% of the total number of corpses studied), the Charpy angle (the angle of convergence of the lower ribs of the chest) is 90-92 degrees, in 51 corpses (31.1%) a Charpy angle of more than 92 degrees is recorded, for the same number of study objects it is less than 88 degrees. In 8 study objects (4.9%) the Charpy angle is 88-90 degrees. In 14 corpses of men in the first period of adulthood (8.5% of the total number of corpses studied), we found an angle of 90-92 degrees, in 1 man (0.6%) an angle of 89 degrees was found, an angle of more than 92 degrees. We registered an angle of less than 88 degrees in 12 study subjects (7.3%), almost as often. (11 men – 6.7%). In 25 corpses of men of the second period of adulthood (15.2%), a Charpy angle of more than 92 degrees was determined; an angle of 90-92 degrees was recorded one and a half times less often. (15 men - 9.1%), even less often the Charpy angle is less than 88 degrees. (10 men – 6.1%). In 21 corpses of women in the first period of adulthood (12.8% of the total number of study subjects), the Charpy angle is less than 88 degrees. An angle of 90-92 degrees is recorded three times less often. (7 corpses - 4.3%), in 2 women (1.2%) the Charpy angle is 88-90 degrees, in 4 people (2.4%) the angle is more than 92 degrees. In the second period of adulthood, 18 women (11.0%) recorded a Charpy angle of 90-92 degrees. , in 5 (3.0%) women the angle is 88-90 degrees. In 9 women (5.5%) the Charpy angle is less than 88 degrees, in 10 (6.1%) it is more than 92 degrees. Based on the results of a statistical analysis of the average Charpy angle and graphical presentation of the data, we can conclude that in men of the first period of adulthood in our study, the cylindrical shape of the chest predominates, and in the second period of adulthood, the conical shape predominates. Women of the first period are characterized by a flattened chest shape, and women of the second period are characterized by a cylindrical chest shape.
Table 3 shows data on the average sizes of the chest of human corpses depending on gender and age. There are almost equal average rates in both age groups, regardless of gender. When studying the corpses of men in the first and second age periods, we found an index of chest width equal to 136±12 and 136±13, respectively. In women in the first period of adulthood, the chest width index is 133±13, in the second period – 136±13.
Acquired chest deformities
Emphysematous chest
Emphysema is an increase in the airiness of the lung tissue. The disease is accompanied by an increase in lung size. This entails a gradual change in the shape of the chest. The anteroposterior size of the chest increases. The patient's chest takes on a rounded shape, the so-called “barrel” chest. Chest excursion decreases.
Paralytic chest
It is observed in chronic diseases of the lungs and pleura, characterized by organ shrinkage. The anteroposterior and lateral dimensions of the chest decrease. There is a retraction of the intercostal spaces, which indicates difficulty in breathing in patients. The collarbones and shoulder blades are also clearly visible - this is due to a change in their location relative to the ribs and sternum. The symmetry of movements of the right and left halves of the chest is disrupted.
Scaphoid chest
It is observed in patients with a rare disease - syringomyelia. This disease causes cavities to form in the spinal cord. One of its manifestations is a change in the composition of bones due to the leaching of calcium salts from them. Bones become less rigid and are able to deform. Patients have a scaphoid depression localized in the upper and middle thirds of the sternum.
Kyphoscoliotic chest
The reason for this is disorders of the spine. This can be a consequence of diseases such as spinal tuberculosis, rickets, scoliosis, or as a result of injuries. When the shape of the spine changes, pathology in the chest organs may be observed.
Also worth mentioning is deformation due to trauma and surgery.
Diagnostics
It is important for the doctor to obtain information on the form of the deformity and data on the function of the patient’s heart and lungs (ECG, echo-kg, spirography).
We use modern diagnostic methods for preoperative examination with assessment of lung and heart function, reconstruction of the original shape of the chest using multislice computed tomography, which also allows us to exclude concomitant pathologies of the chest organs, which reduces the risk of intraoperative complications.
Of course, a general preoperative examination of systems and organs is also carried out for planned surgical treatment.
Each patient has a photo and video recording of the initial deformity, which also facilitates preoperative planning and follow-up with assessment of the achieved correction.
Treatment of chest deformity in Israel
Most acquired deformities of the chest are a consequence of chronic diseases of the chest organs and do not pose a threat to the patient’s life.
Congenital deformities are treated
Conservative treatment of chest deformity is ineffective. Surgical treatment is indicated for disorders of the chest organs or for severe cosmetic defects. It is carried out when the child reaches the age of 6-7 years. By this time, the formation of the defect usually stops.
Chest reconstruction
Reconstruction of the chest is being carried out. The sunken parts return to their place and are fixed mechanically. With keeled deformity, the costal cartilages are truncated (this pathology is less often an indication for surgical intervention).
Magnet implantation
New treatments involve implanting a magnet in the area that needs to be corrected. The second magnet is positioned so that their interaction generates a force aimed at eliminating the defect.
Some deformities can be masked by implanting silicone over the area of deformation.
Currently, operations to eliminate chest defects with minimal consequences for the body are being successfully carried out in Israel.
Attention! All form fields are required. Otherwise we will not receive your information. Alternatively use
Publications in the media
Congenital chest deformities are developmental defects associated with changes in the shape of the chest wall.
Funnel chest (pectus excavatus) is a developmental defect, which, in addition to a cosmetic defect in the form of retraction of the sternum and ribs, is accompanied by various functional disorders in the respiratory system and cardiovascular system. In boys it is observed 3 times more often. There are three stages of the disease (compensated, subcompensated and decompensated), three forms of deformities (symmetrical, asymmetrical and funnel-shaped), three degrees of deformation (I degree - deformation depth less than 2 cm, no displacement of the heart; II degree - deformation depth less than 4 cm, displacement heart by 2–3 cm; III degree - depth of deformation more than 4 cm, displacement of the heart by more than 3 cm). Treatment: general and special gymnastic exercises, massage. Surgical treatment is indicated for progressive deformities with functional impairment at the age of 4–5 years. There are many methods in the arsenal of surgical treatment, but none of them is accepted as optimal. With each, the risk of late relapses is noted • Removal of deformed costal cartilages • Osteotomy of the sternum • Correction of the sternum defect by introducing a bone wedge • Fixation with a support bar located behind the sternum • Other options: dosed traction, use of magnets, etc.
Keeled chest deformity (“chicken breast”, pectus carinatum) is a protrusion of the sternum and the costal cartilages attached to it. Damage to the costal cartilages can be unilateral or bilateral, and the sternum protrudes anteriorly in the upper or lower sections. With conservative treatment, general and special gymnastic exercises and massage are prescribed. Of the proposed surgical treatment methods, subperichondral resection of cartilage is the most acceptable. Corrected by transverse osteotomy with posterior movement of the sternum.
Poland syndrome is a combination of abnormalities including absence of the pectoralis major and minor muscles, syndactyly, brachydactyly, atelia and/or amastia, deformed or absent ribs, absence of hair in the armpit, and decreased thickness of the subcutaneous tissue. Each patient has different components of the syndrome. Deformation of the chest varies from mild hypoplasia of the ribs and costal cartilages on the affected side to aplasia of the anterior part of the ribs and all costal cartilages. Surgical treatment is necessary for only a small proportion of patients.
Sternal defects - a wide range of rare anomalies of the sternum, heart and upper abdominal wall • Thoracic ectopia cordis - the classic “naked heart”, not covered in front by any tissue, often noted is tetralogy of Fallot, pulmonary stenosis, transposition of the great vessels and VSD. Treatment of thoracic ectopia of the heart is almost always unsuccessful • Cervical ectopia of the heart. Patients differ from patients with thoracic ectopia in the distance to which the heart is moved • Thoraco-abdominal ectopia of the heart. The lower part of the sternum is split, the heart is covered with a membrane. Surgery is aimed at closing the skin defect over the heart and abdomen • Cleft or bifurcated sternum • Distal sternal defect is encountered as part of Cantrell's pentad.
Anterior scalene syndrome • Causes: accessory cervical rib, spasm and secondary shortening of the scalene muscle or traumatic deformity of the bones of the chest and shoulder girdle • Clinical picture. Pain in the neck, shoulder girdle and arm (along the ulnar nerve) and peripheral paresis of the arm caused by compression of the neurovascular bundle in the anterior interscalene space (between the anterior and middle scalene muscles). The clinical picture resembles Raynaud's disease • The diagnosis is confirmed by studying the functions of the ulnar nerve • Treatment. Decompression of the neurovascular bundle, most often by resection of the first or accessory cervical rib (if present), dissection of the anterior scalene muscle. Release of nerves from surrounding scar tissue, usually performed through a supraclavicular approach.
ICD-10 • M95.4 Acquired deformity of the chest and ribs • Q67 Congenital musculoskeletal deformities of the head, face, spine and chest • Q67.6 Sunken chest • Q67.7 Keeled chest • Q67.8 Other congenital chest deformities