The article was checked by a cardiologist, Ph.D. Zhelyakov E.G. , is for general informational purposes only and does not replace specialist advice. For recommendations on diagnosis and treatment, consultation with a doctor is necessary.
Specialists at the Clinical Hospital on Yauza diagnose the causes of shortness of breath (assessment of respiratory function, X-ray, ECG) and treat the diseases that cause it at the modern level. Treatment of shortness of breath always involves treating the underlying disease and eliminating its causes (for example, achieving compensation for heart failure, etc.).
- Shortness of breath is the main symptom of chronic heart failure, bronchial asthma, chronic obstructive pulmonary disease
- Up to 27% of people worldwide suffer from some form of shortness of breath
- Spirography is the gold standard for assessing external respiration
sign up for a consultation
Shortness of breath (dyspnea) - a violation of the rhythm, frequency, depth of breathing, a subjective feeling of lack of air, difficulty breathing - this is a complaint with which the patient first of all turns to a doctor. This symptom can be a manifestation of various diseases.
Respiration is an important body function that ensures that all cells have enough oxygen to survive and that toxic carbon dioxide is removed. Any problems that arise during the breathing process and cause shortness of breath may be a sign of serious illness. Therefore, there is a need for immediate medical attention.
Sudden shortness of breath may be caused by the development of heart pathologies or an asthma attack. Long-term shortness of breath is usually associated with pulmonary pathology.
Types of shortness of breath
The sensation of shortness of breath occurs when a signal from receptors located in the epithelium of the respiratory tract enters the respiratory center located in the brain stem. Respiratory signals are processed taking into account behavioral, intellectual and situational signals.
Shortness of breath is a symptom of the disease, not the disease itself. Therefore, its etiology can be defined as arising from four main categories:
- Central – diseases of the nervous system with impaired functioning of the respiratory center, with neuroses and other functional pathologies of the central nervous system.
- Pulmonary – observed in diseases of the lungs (pneumonia, chronic obstructive pulmonary disease, bronchial asthma, pulmonary fibrosis) and chest.
- Cardiac – a symptom of heart failure during myocardial infarction, myocarditis, cardiomyopathies, heart defects, etc.
- Hematogenous - any type of anemia, the effect on the respiratory center of changes in blood acidity and toxic metabolic products in case of poisoning, liver failure, decompensated diabetes mellitus, etc.
For different diseases, shortness of breath is perceived differently, but in any case it differs from increased breathing, which occurs during physical activity in healthy people.
Note!
Differences between cardiac and pulmonary dyspnea:
- With cardiac dyspnea, the heart cannot cope with the load, stagnation occurs and gas exchange is disrupted, which provokes rapid breathing.
- Pulmonary shortness of breath appears due to the accumulation of sputum in the organs of the respiratory system and is accompanied by a cough.
Cardiac dyspnea, unlike pulmonary dyspnea, occurs without expiratory difficulties (short inhalation and difficult exhalation). In an upright position and at rest the condition improves. With pulmonary dyspnea, hypoxemia (low oxygen in the blood), respiratory acidosis (accumulation of large amounts of carbon dioxide in the blood) and hypercapnia (excessive amount of CO2 in the blood) are observed.
Shortness of breath is a subjective sensation. Only the patient himself can differentiate its intensity. However, in any case, if you feel short of breath, it is better to consult a doctor and determine the cause of the ailment. Shortness of breath is often a symptom of a serious pathology that can lead to disability. To avoid serious illnesses, make an appointment with a doctor and get tested without delay.
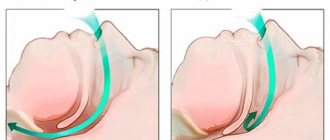
Take a deep breath: learning to breathe correctly with a Moscow psychologist
Human breathing is an everyday and imperceptible process that we usually don’t think about. But as soon as you are deprived of oxygen for a minute, all other problems fade into the background. Often during anxiety, people experience a feeling of difficulty breathing, the inability to breathe deeply, or a sudden or increasing feeling of lack of air. Konstantin Zherdev , a specialist at the Moscow Psychological Assistance Service, told us how to cope with this illness
There are several types of shortness of breath:
- True shortness of breath is associated with diseases (usually chronic) in organs and systems.
- Functional shortness of breath indicates physical stress; a person experiences it, for example, when running. It goes away after the end of the load or as the body adapts to such work. This ability to adapt is sometimes called "second wind."
- Psychogenic shortness of breath is associated with the experience of acute or chronic psycho-emotional stress: anxiety, depression, neurosis, stress and even intense joy. Episodes associated with joyful difficulty breathing are well known to us: “the breath stole from the goiter from joy.”
“Often, hidden anxiety manifests itself through difficulty breathing, nighttime and daytime episodes of suffocation, which go away on their own. True, at the moments of these experiences they are seriously frightening. Such experiences were clearly illustrated by G. Fusli in a series of paintings, which he called “Nightmare”. As a rule, shortness of breath during anxiety goes away when attention is switched from it to something extraneous. Warm drinks, conversations, and simply getting out of an alarming situation have a positive effect on breathing,” notes the psychologist.
Breathe out your anxiety
Frequent shallow breathing, which often accompanies anxiety, leads to an increase in oxygen levels in the blood and a decrease in carbon dioxide. This shift in balance is accompanied by various unpleasant manifestations: dizziness, a feeling of suffocation, cold extremities, a feeling of impending loss of consciousness, and increasing tinnitus. Often such complaints are the reason for seeking help from doctors.
Of course, in order to rule out various types of diseases, you need to seek advice from medical specialists and undergo an examination. But it often happens that no diseases are detected. In this case, you should pay attention to your psychological state.
“To overcome these moments, it will be useful to reduce excess muscle tone, as well as normalize respiratory cycles. That is, allow the body to independently manage important processes, in other words, do not interfere. Using the power of breathing to create a comfortable psychological environment is the right way. Thinking that the body won’t cope without us and will forget to breathe is wrong,” advises Konstantin.
Moderate sports and physical activity, reducing caffeine and alcohol consumption, and limiting negative information load will also be useful.
Workshop from a psychologist
During an acute state of anxiety, the whole consciousness “screams” that there is not enough air and you want to inhale as deeply and often as possible - to get air into your chest.
Try to do the following: relax the muscles of the shoulders, neck, abdomen, relax the chest muscles, facial muscles, base of the tongue. At the same time, exhale calmly and slowly. Help yourself with your stomach by pulling your abdominal muscles inward as you exhale. Make room inside yourself for a short but full breath. Relax your stomach and take a calm breath (1-2 seconds) and exhale long again (4-6 seconds). Sometimes it is recommended to take a short pause between each cycle: inhale - pause for 2-4 seconds, exhale - pause, etc. If it is difficult for you to hold a pause, then at the beginning you can not include it in the exercise. Repeat this cycle of inhalation and exhalation 6 times. Practice breathing like this in a calm state. Do not hurry.
There is no need to try to exhale all the way and there is no need to take a sharp breath.
This leads to irritation by the air flow of the upper respiratory tract and causes a feeling of additional tension in the throat, and can also provoke coughing and tickling. The entire exercise is performed in a comfortable mode. The task is to breathe calmly and without jerking. Breathing cycles can be accompanied mentally with the phrase: “My breathing is smooth and calm.” We say the first part of the phrase - “My breath” while inhaling, the second part - “even and calm” - we say as we exhale. You can sign up for free classes on self-regulation and training in breathing techniques at the Moscow Service for Psychological Assistance to the Population
www.msph.ru. Source
Press service of the Department of Labor and Social Protection of the Population of Moscow
Causes of shortness of breath
Shortness of breath, a feeling of lack of air can be associated with disturbances in external (oxygen supply through the lungs) or internal (tissue) respiration:
- Impact on the respiratory center of toxins, metabolic products in severe infectious diseases.
- Respiratory impairment due to exposure to toxic chemicals at the cellular level.
- Chest injuries that violate the tightness of the pleural cavities; compression of the lungs with pneumothorax, hydrothorax.
- Neurological complications in multiple sclerosis, myasthenia, functional and neurotic breathing disorders in hysteria, neurasthenia, etc.
- Blockage of the airway lumen with viscous secretion (with bronchitis, bronchial asthma), tumor, foreign body (button, food, vomit).
- Swelling and thickening of the bronchial wall, spasm of the bronchial muscles of an allergic or inflammatory nature in bronchial asthma, pneumonia, etc.
- Heart failure, in which there is stagnation of blood in the vessels of the pulmonary circulation, effusion of fluid into the alveoli of the lungs, a decrease in the vital capacity of the lungs, and a decrease in peripheral blood flow.
- Coronary heart disease, when the main symptom of insufficient blood supply to the myocardium is shortness of breath.
- For anemia as a result of decreased hemoglobin levels and a decrease in the number of red blood cells due to blood loss; in case of poisoning with certain chemicals that bind hemoglobin.
- Obesity and physical detraining can also cause shortness of breath with minimal physical activity.
Intense exercise, extreme temperatures, obesity, and high altitude can all cause shortness of breath in a healthy person. Outside of these examples, dyspnea is a sign of a medical problem. If you experience unexplained breathing problems, especially if they occur suddenly, you should consult a doctor immediately.
Difficulty breathing - causes of the disorder
The feeling that there is not enough air in the lungs is not always due to any disease. This phenomenon can occur during physical exertion, emotional shock, or sudden climate change. If the feeling of shortness of breath bothers you regularly, this may be due to serious problems:
- diseases of the heart muscle;
- vegetative-vascular dystonia;
- pulmonary pathologies;
- the presence of foreign bodies in the respiratory tract;
- diabetes mellitus;
- oncology;
- infectious processes.
Other causes of difficulty breathing are active smoking, a tendency to allergies, excess body weight, and nervous disorders. The problem often occurs during pregnancy and is associated with bearing a large fetus, twins or triplets, and polyhydramnios.
Symptoms of shortness of breath
Dyspnea can be characterized by a variety of clinical manifestations due to the large number of possible causes. However, the most common symptoms are coughing and changes in breathing patterns. Signs may appear when a person is at rest and during intense exercise.
Symptoms that accompany shortness of breath:
- fatigue, weakness;
- cardiopalmus;
- sudden lack of air;
- difficulty breathing in and out;
- signs of dizziness;
- swelling of the lower extremities;
- fast, irregular heartbeat;
- decreased physical activity;
- cough or wheezing when breathing;
- hemoptysis (coughing up blood);
- blueness of nails and lips due to poor circulation;
- pain, tightness in the chest (if shortness of breath occurs as a result of a heart attack).
The patient feels as if after intense physical activity or hard physical work. Respiratory dysfunction prevents a person from speaking normally and pronouncing long words and phrases. Speech becomes short and abrupt.
All breathing problems, whether sudden or long-term, regardless of symptoms, should be taken seriously. Although many of the possible causes are harmless and easily treatable, you should still see a doctor for a thorough medical examination.
Shortness of Air: Case Studies
Woman, 32 years old, entrepreneur.
From the anamnesis: over the past five to seven years, I worked very hard, practically never rested. A month before the first complaints appeared, she gave birth to a child (caesarean section). She did not tolerate anesthesia well (long awakening, headaches, drowsiness). A week after giving birth, an episode of “shortness of air” occurred.
I contacted our clinic in November 2011. The main complaint is a constant feeling of shortness of breath when breathing, aggravated by excitement, while talking with other people (“I can either breathe or talk”), as well as when walking, in enclosed spaces or public places.
Also about chills, unstable blood pressure, rapid resting pulse (up to 130 beats per minute). I developed a cold allergy (nasal congestion when going outside in the autumn-winter period).
The woman underwent 2 courses of therapy. There are currently no symptoms.
Female, 27 years old, journalist
The onset of his illness is associated with the stress he experienced. Before her eyes, her father suddenly dies, who, in her words, was an absolutely healthy person.
Just a few days after the funeral, she develops a classic panic attack with severe weakness, a feeling of shortness of breath when inhaling, shortness of breath and palpitations. Shortness of breath also tormented the patient during the interictal period. So, at the clinic appointment, she was noticeably breathing heavily, spoke with pauses, resting for a long time after several spoken phrases.
After the examination, a diagnosis of severe dysfunction of the autonomic nervous system was made.
After the first course of therapy, panic attacks stopped completely. A repeated course helped to cope with residual manifestations of the disease in the form of episodes of lack of air when breathing.
Feelings of fear and anxiety Presyncope, weakness Sweating, sweating, heavy sweat Prolonged low-grade fever Sleep disorder, insomnia, drowsiness Chronic fatigue syndrome Headaches Constant heaviness in the head
Muscle tone, spasm of the neck muscles Weather dependence Lack of air, heavy breathing Strong heartbeat, rapid pulse Burning in the abdomen, pain in the stomach Discomfort in the intestines, diarrhea Urinary incontinence Blurred vision, vision problems
What to do if you have severe shortness of breath?
Noninvasive ventilation (NIV) provides relief for increased breathing needs. This procedure is less useful for patients with defects in oxygen diffusion in the alveolar arteries. The most effective component of pulmonary rehabilitation is special breathing exercises.
Recommendations to follow in case of severe shortness of breath:
- If you have serious breathing problems, it is better to sleep with the head of the bed raised. This will help the lungs expand and promote drainage of secretions.
- While sitting, lean forward on your elbows. This will also help your lungs expand and make breathing easier.
- To reduce anxiety, you can use relaxation techniques (take slow, even, deep breaths and try to focus on pleasant things).
- Take medications strictly as prescribed by your doctor.
- If you experience side effects from your medications, especially if they are severe, tell your doctor or emergency team members.
- Use pursed-lip breathing when you feel short of breath. Inhale through your nose and exhale very slowly through your mouth, pursing your lips slightly. The exhalation should last twice as long as the inhalation.
- If you experience sudden breathing problems, you should open a window, move to another room where there are fewer people, or go outside.
- Nicotine and other chemicals in cigarettes can make shortness of breath worse. Electronic cigarettes also contain nicotine.
- Cold air and using fans to blow air onto the face can significantly improve shortness of breath. Supplemental oxygen has only been shown to be beneficial in hypoxic patients.
Simple but effective recommendations help improve your shortness of breath. Additional measures are aimed at reducing anxiety and providing an increased sense of control.
There are a huge number of reasons for shortness of breath. It is impossible to determine on your own whether it is a symptom of a serious illness. Only a highly qualified specialist can determine which organ disease caused the pathology and prescribe the appropriate examination. Make an appointment with your doctor to determine the cause of your discomfort.
sign up for a consultation
Diagnostic stages
Consultation with a therapist. The doctor will conduct a thorough examination of the patient and ask him about accompanying symptoms. If necessary, he will refer the patient to other specialists at our hospital - a cardiologist, hematologist, and psychotherapist.
Laboratory diagnostics
:
- general blood analysis;
- blood chemistry.
Instrumental diagnostics
:
- spirography
- ECG;
- ECHO-KG
- Chest CT scan or radiography.
Additional examination
, the volume of which is determined individually depending on the direction of the diagnostic search.
Treatment of shortness of breath
Treatment of shortness of breath is carried out in accordance with the cause and individually for each patient.
For bronchitis with difficulty in sputum discharge, the therapist may prescribe sputum thinners and expectorants; for bronchial obstruction, bronchodilators.
Treatment of shortness of breath in heart failure is complex and prescribed by a cardiologist.
For hematogenous dyspnea, treatment is aimed at combating anemia.
The psychogenically caused feeling of lack of air, characteristic of panic attacks and other forms of neurotic disorders, is treated in a course of psychotherapy.
In case of massive pleural effusion (accumulation of fluid in the pleural cavity and compression of the lung), puncture of the pleural cavity (removal of fluid) may be necessary, performed by a surgeon.
In acute conditions with severe life-threatening respiratory disorders, urgent hospitalization of the patient in the intensive care unit for mechanical ventilation is required.
If you are concerned about shortness of breath, you should consult a doctor. The multidisciplinary team of doctors at the Yauza Clinical Hospital will help you correctly prescribe and conduct an examination, establish the cause, and prescribe effective treatment.
Neurogenic respiratory disorders: hyperventilation syndrome
History of the study of hyperventilation syndrome (HVS). The first clinical description of HVS was by Da Costa (1842), who summarized his observations of soldiers participating in the Civil War. He observed breathing disorders and various associated unpleasant sensations in the heart area, calling them “soldier’s heart”, “irritable heart”. The connection between pathological symptoms and physical activity was emphasized, hence another term - “effort syndrome”. In 1918, Lewis proposed another name, “neurocirculatory dystonia,” which is still widely used by therapists. Manifestations of HVS such as paresthesia, dizziness, and muscle spasms have been described; a connection between increased breathing (hyperventilation) and muscular-tonic and tetanic disorders has been noted. Already in 1930, it was shown that pain in the heart area with Da Costa syndrome is not only associated with physical activity, but also with hyperventilation as a result of emotional disturbances. These observations were confirmed during the Second World War. Hyperventilation manifestations were noted in both soldiers and civilians, which indicated the importance of psychological factors in the genesis of HVS.
Etiology and pathogenesis. In the 80–90s of the twentieth century, it was shown that HVS is part of the structure of the psychovegetative syndrome [1]. The main etiological factor is anxiety, anxiety-depressive (less often, hysterical) disorders. It is mental disorders that disrupt normal breathing and lead to hyperventilation. The respiratory system, on the one hand, has a high degree of autonomy, on the other, a high degree of learning ability and a close connection with the emotional state, especially anxiety. These features underlie the fact that HVS is in most cases of psychogenic origin; extremely rarely it is caused by organic neurological and somatic diseases - cardiovascular, pulmonary and endocrine.
Complex biochemical changes play an important role in the pathogenesis of HVS, especially in the calcium-magnesium homeostasis system. Mineral imbalance leads to an imbalance in the respiratory enzyme system and contributes to the development of hyperventilation.
The habit of breathing incorrectly is formed under the influence of cultural factors, past life experiences, as well as stressful situations suffered by the patient in childhood. The peculiarity of childhood psychogenies in patients with HVS is that they often involve respiratory dysfunction: children witness dramatic manifestations of attacks of bronchial asthma, cardiovascular and other diseases. In the past, patients themselves often have an increased load on the respiratory system: running, swimming, playing wind instruments, etc. In 1991, I. V. Moldovanu [1] showed that with HVS there is instability of breathing, a change in the ratio between the duration of inspiration and exhale.
Thus, the pathogenesis of HVS appears to be multilevel and multidimensional. A psychogenic factor (most often anxiety) disrupts normal breathing, resulting in hyperventilation. An increase in pulmonary and alveolar ventilation leads to stable biochemical changes: excessive release of carbon dioxide (CO2) from the body, the development of hypocapnia with a decrease in the partial pressure of CO2 in the alveolar air and oxygen in the arterial blood, as well as respiratory alkolosis. These shifts contribute to the formation of pathological symptoms: impaired consciousness, autonomic, muscular-tonic, algic, sensory and other disorders. As a result, mental disorders increase and a pathological circle is formed.
Clinical manifestations of HVS. HVS can be paroxysmal in nature (hyperventilation crisis), but more often hyperventilation disorders are permanent. HVS is characterized by a classic triad of symptoms: respiratory disorders, emotional disturbances and muscular-tonic disorders (neurogenic tetany).
The first are represented by the following types:
- "empty breath";
- violation of breathing automaticity;
- labored breathing;
- hyperventilation equivalents (sighs, coughing, yawning, sniffling).
- Emotional disorders are manifested by feelings of anxiety, fear, and internal tension.
Muscular-tonic disorders (neurogenic tetany) include:
- sensory disturbances (numbness, tingling, burning);
- convulsive phenomena (muscle spasms, “obstetrician’s hand”, carpopedal spasms);
- Chvostek syndrome II–III degree;
- positive Trousseau test.
In the first type of respiratory disorder - “empty breath” - the main sensation is dissatisfaction with inhalation, a feeling of lack of air, which leads to deep breaths. Patients constantly lack air. They open the vents and windows and become “air maniacs.” Respiratory disorders intensify in agoraphobic situations (subway) or social phobia (exam, public speaking). Breathing in such patients is frequent and/or deep.
In the second type - a violation of the automaticity of breathing - patients have a feeling of stopping breathing, so they continuously monitor the act of breathing and are constantly involved in its regulation.
The third type - shortness of breath syndrome - differs from the first option in that breathing is felt by patients as difficult and performed with great effort. They complain of a “lump” in the throat, failure of air to pass into the lungs, and constriction of breathing. This variant is called "atypical asthma." Objectively, increased breathing and irregular rhythm are noted. The act of breathing uses the respiratory muscles. The patient looks tense and restless. Examination of the lungs does not reveal any pathology.
The fourth type - hyperventilation equivalents - is characterized by periodically observed sighs, coughing, yawning, and sniffling. These manifestations are sufficient to maintain prolonged hypocapnia and alkalosis in the blood.
Emotional disturbances in HVS are mainly of an anxious or phobic nature. The most common disorder is generalized anxiety disorder. It, as a rule, is not associated with any specific stressful situation - the patient experiences various mental (feelings of constant internal tension, inability to relax, anxiety over trifles) and somatic manifestations for a long time (more than 6 months). Among the latter, respiratory disorders (usually “empty breath” or hyperventilation equivalents - coughing, yawning) may form the core of the clinical picture - along with, for example, algic and cardiovascular manifestations.
Respiratory disturbances reach a significant degree during a panic attack, when a so-called hyperventilation crisis develops. Disorders of the second and third types are more common - loss of automatic breathing and difficulty breathing. The patient experiences a fear of suffocation and other symptoms characteristic of a panic attack. To diagnose a panic attack, four of the following 13 symptoms must be observed: palpitations, sweating, chills, shortness of breath, suffocation, pain and discomfort in the left side of the chest, nausea, dizziness, a feeling of derealization, fear of going crazy, fear of death, paresthesia, waves heat and cold. An effective method for relieving a hyperventilation crisis and other symptoms associated with respiratory failure is breathing into a paper or plastic bag. In this case, the patient breathes his own exhaled air with a high content of carbon dioxide, which leads to a decrease in respiratory alkalosis and the listed symptoms.
Agoraphobia is often the cause of HVS. This is fear that arises in situations that the patient regards as difficult to help him. For example, a similar condition can occur in the subway, store, etc. Such patients, as a rule, do not leave home unaccompanied and avoid these places.
A special place in the clinical picture of HVS is occupied by an increase in neuromuscular excitability, manifested by tetany. Tetanic symptoms include:
- sensory disorders in the form of paresthesia (numbness, tingling, crawling, buzzing, burning sensations, etc.);
- convulsive muscular-tonic phenomena - spasms, contractions, tonic convulsions in the hands, with the phenomenon of “obstetrician’s hand” or carpopedal spasms.
These manifestations often occur in the picture of a hyperventilation crisis. In addition, increased neuromuscular excitability is characterized by Chvostek's symptom, a positive Trousseau cuff test and its variant, the Trousseau-Bahnsdorff test. The characteristic electromyographic (EMG) signs of latent muscle tetany are essential in the diagnosis of tetany. An increase in neuromuscular excitability is caused by the presence in patients with HVS of a mineral imbalance of calcium, magnesium, chlorides, and potassium, caused by hypocapnic alkalosis. There is a clear connection between increased neuromuscular excitability and hyperventilation.
Along with the classic manifestations of HVS, paroxysmal and permanent, there are other disorders characteristic of the psychovegetative syndrome as a whole:
- cardiovascular disorders - pain in the heart, palpitations, discomfort, chest compression. Objectively, lability of pulse and blood pressure, extrasystole are noted, and on the ECG - fluctuation of the ST segment; acrocyanosis, distal hyperhidrosis, Raynaud's phenomenon;
- disorders of the gastrointestinal tract: increased intestinal motility, belching of air, bloating, nausea, abdominal pain;
- changes in consciousness, manifested by a feeling of unreality, lipothymia, dizziness, blurred vision, in the form of fog or a grid before the eyes;
- algic manifestations, represented by cephalgia or cardialgia.
So, to diagnose hot water supply, confirmation of the following criteria is necessary:
- The presence of polymorphic complaints: respiratory, emotional and muscular-tonic disorders, as well as additional symptoms.
- Absence of organic nervous and somatic diseases.
- Presence of psychogenic history.
- Positive hyperventilation test.
- Disappearance of symptoms of hyperventilation crisis when breathing into a bag or inhaling a mixture of gases (5% CO2).
- Presence of tetany symptoms: Chvostek's sign, positive Trousseau test, positive EMG test for latent tetany.
- Change in blood pH towards alkalosis.
Treatment of hot water supply
Treatment of hot water supply is comprehensive and is aimed at correcting mental disorders, teaching proper breathing, and eliminating mineral imbalances.
Non-drug methods
- The essence of the disease is explained to the patient, they are convinced that it is curable (the origin of the symptoms of the disease, especially somatic ones, and their relationship with the mental state are explained; they are convinced that there is no organic disease).
- It is recommended to quit smoking and drink less coffee and alcohol.
- Breathing exercises are prescribed to regulate the depth and frequency of breathing. To carry it out correctly, several principles must be observed. First, switch to diaphragmatic abdominal breathing, during which the “inhibitory” Hering-Breuer reflex is activated, causing a decrease in the activity of the reticular formation of the brain stem and, as a result, muscle and mental relaxation. Secondly, maintain certain relationships between inhalation and exhalation: inhalation is 2 times shorter than exhalation. Thirdly, breathing should be rare. And finally, fourthly, breathing exercises should be carried out against the background of mental relaxation and positive emotions. At first, breathing exercises last for several minutes, then for quite a long time, forming a new psychophysiological breathing pattern.
- For severe hyperventilation disorders, breathing into a bag is recommended.
- Autogenic training and breathing-relaxation training are shown.
- Psychotherapeutic treatment is highly effective.
- Among the instrumental non-drug methods, biofeedback is used. The feedback mechanism with the objectification of a number of parameters in real time allows you to achieve more effective mental and muscle relaxation, as well as regulate your breathing pattern more successfully than with autogenic training and breathing-relaxation training. The biofeedback method has been successfully used for many years in the Clinic of Headache and Autonomic Disorders named after. acad. A. Veina for the treatment of hyperventilation disorders, panic attacks, anxiety and anxiety-phobic disorders, as well as tension headaches.
Medicinal methods
Hyperventilation syndrome refers to psychovegetative syndromes. Its main etiological factor is anxiety, anxiety-depressive and phobic disorders. Psychotropic therapy has priority in its treatment. In the treatment of anxiety disorders, antidepressants are more effective than anxiolytic drugs. Patients with anxiety disorders should be prescribed antidepressants with pronounced sedative or anxiolytic properties (amitriptyline, paroxetine, fluvoxamine, mirtazapine). The therapeutic dose of amitriptyline is 50–75 mg/day; to reduce side effects: lethargy, drowsiness, dry mouth, etc., the dose should be increased very slowly. Selective serotonin reuptake inhibitors have better tolerability and fewer unwanted side effects. The therapeutic dose of fluvoxamine is 50–100 mg/day, paroxetine is 20–40 mg/day. Their most common unwanted side effects include nausea. To prevent it or more successfully overcome it, it is also recommended to prescribe the drug at half the dosage at the beginning of therapy and take it with meals. Given the hypnotic effect of fluvoxamine, the drug should be prescribed in the evening; Paroxetine has less pronounced hypnogenic properties, so it is often recommended to take it with breakfast. The four-cyclic antidepressant mirtazapine has a pronounced anti-anxiety and hypnotic effect. It is usually prescribed at bedtime, starting with 7.5 or 15 mg, gradually increasing the dose to 30–60 mg/day. When prescribing balanced antidepressants (without pronounced sedative or activating effects): citalopram (20–40 mg/day), escitalopram (10–20 mg/day), sertraline (50–100 mg/day), etc., their combination is possible for a short period of 2–4 weeks with anxiolytics. The use of such a “benzodiazepine bridge” in some cases makes it possible to accelerate the onset of action of psychotropic therapy (this is important, given the delayed effect of antidepressants by 2-3 weeks) and to overcome the increase in anxiety symptoms that temporarily arise in some patients at the beginning of therapy. If the patient has hyperventilation crises during an attack, along with breathing into the bag, anxiolytics should be taken as abortive therapy: alprazolam, clonazepam, diazepam. The duration of psychotropic therapy is 3–6 months, if necessary up to 1 year.
Psychotropic drugs, along with a positive therapeutic effect, also have a number of negative properties: unwanted side effects, allergization, development of addiction and dependence, especially to benzodiazepines. In this regard, it is advisable to use alternative means, in particular, means that correct mineral imbalance, which is the most important symptom-forming factor in hyperventilation disorders.
As agents that reduce neuromuscular excitability, drugs that regulate calcium and magnesium metabolism are prescribed. The most commonly used are ergocalciferol (vitamin D2), Calcium-D3, as well as other medications containing calcium for 1–2 months.
The generally accepted view is that magnesium is an ion with clear neurosedative and neuroprotective properties. Magnesium deficiency in some cases leads to increased neuro-reflex excitability, decreased attention, memory, convulsive attacks, impaired consciousness, heart rhythm, sleep disorders, tetany, paresthesia, and ataxia. Stress - both physical and mental - increases the need for magnesium in the body and causes intracellular magnesium deficiency. A state of stress leads to depletion of intracellular magnesium reserves and its loss in the urine, since an increased amount of adrenaline and norepinephrine promotes its release from cells. Magnesium sulfate has been used in neurological practice for a long time as an antihypertensive and anticonvulsant. There are studies on the effectiveness of magnesium in the treatment of the consequences of acute cerebrovascular accident [2] and traumatic brain injury [4], as an additional remedy for epilepsy, and the treatment of autism in children [3, 7].
Magne B6 contains magnesium lactate and pyridoxine, which additionally potentiates the absorption of magnesium in the intestine and its transport into cells [6]. The implementation of the sedative, analgesic and anticonvulsant effects of magnesium-containing drugs is based on the property of magnesium to inhibit excitation processes in the cerebral cortex [5]. Prescribing Magne B6 both as monotherapy, 2 tablets 3 times a day, and in complex therapy in combination with psychotropic drugs and non-drug treatment methods, leads to a decrease in the clinical manifestations of HVS.
For questions regarding literature, please contact the editor.
E. G. Filatova, Doctor of Medical Sciences, Professor of MMA named after. I. M. Sechenova, Moscow
Complications after difficulty breathing
People suffering from shortness of breath are limited in daily and social activities. This affects independence and reduces social significance. As it progresses, anxiety and worry arise. Sleep disturbance occurs and depression develops. Chronic heart failure is especially dangerous.
Metabolism and gas exchange disorders in the body can lead to dangerous complications:
- decrease in blood pressure;
- pulmonary edema;
- persistent breathing problems;
- attacks of suffocation against the background of cardiac cardiac asthma.
As the disease progresses, the following disorders are observed:
- blueness of the limbs and lips (cyanosis);
- suffocating cough at night;
- gurgling sensation in the heart area;
- the appearance of profuse cold sweat;
- development of pulmonary emphysema;
- discharge of sputum with traces of blood;
- decreased elasticity of lung tissue and blood vessels.
Pulmonary edema and heart failure are very serious and dangerous pathologies for human health. If shortness of breath occurs at rest, you should immediately seek medical help.
VSD in faces
This page contains excerpts from patient histories, covering the main complaints with which people turn to us for help. This is done with the goal of showing how different and “complex” the symptoms of vegetative-vascular dystonia can be. And how closely it is sometimes “fused” with disturbances in the functioning of organs and systems. How it “disguises” itself as “heart”, “pulmonary”, “stomach”, “gynecological” and even “psychiatric” problems that people have to live with for years...
To learn more
Prognosis and prevention
Dyspnea does not fall into the category of systemic diseases. This is a sign of the development of cardiac or pulmonary pathology. The problem can only be dealt with by treating the underlying disease. With dystrophic changes as a result of the development of cardiac pathologies, survival rate decreases to 60%. Only early diagnosis and timely treatment can guarantee a favorable outcome.
To relieve the symptoms of shortness of breath or for prevention purposes, it is recommended to adhere to the following rules:
- Perform simple exercises to train the respiratory system and increase muscle tone, unless there are contraindications.
- Avoid contact with allergens that may worsen the condition.
- Prevent seasonal infections.
- Stop smoking.
- Control body weight.
The main condition for preventive measures is strict compliance with all recommendations of the attending physician.
Shortness of breath may make it difficult to eat. Here are some practical tips for saving energy and getting the most out of your food:
- eat in small portions;
- try to breathe calmly and evenly while eating;
- Frozen convenience foods, ready-made meals, or take-out and delivery can make life easier;
- it is recommended to limit the amount of products that cause gas formation;
- You can keep a food diary to determine which foods worsen your overall condition.
In some cases, acupressure and/or acupuncture can help. Before deciding to prescribe procedures, you should definitely consult your doctor. Both practices focus on stimulating hot spots to optimize energy flow and release blockages.
Dyspnea at rest is a rare phenomenon that accompanies severe and advanced diseases. This phenomenon usually appears during physical activity. Pay attention to whether you have difficulty breathing when climbing stairs or walking quickly. If you notice a lack of oxygen, be sure to make an appointment with your doctor for consultation.
Why us
- Doctors. We receive specialists of the highest qualification category, holders of academic degrees, with extensive experience in leading Russian clinics.
- Individual approach. The doctor will develop an individual examination and treatment plan for each patient in accordance with the cause of development and clinical picture of the disease.
- Complexity. The therapists at our clinic work in close collaboration with other specialists - cardiologists, hematologists, psychotherapists. This provides effective treatment for shortness of breath of various origins.
- Expert equipment. All studies are carried out using modern equipment and are highly accurate.
- Comfort. All consultations, studies and treatment are carried out within our hospital, which allows our patients to save energy and time.
You can see prices for services