Chest pain is a very common symptom that causes great concern. After all, we all know that this is how diseases of the cardiovascular system manifest themselves. But in reality, this symptom may indicate other disorders in the body, in particular pathologies of the gastrointestinal tract, respiratory system and even the spine. In any case, such a sign cannot be ignored, especially with acute pain, since extremely dangerous conditions, for example, pulmonary embolism and myocardial infarction, can manifest themselves in this way. With them, the patient’s life directly depends on the urgency of providing qualified medical care. Let's look at the main causes of chest pain and their distinctive signs.
Diseases of the cardiovascular system
Pathologies of the heart and blood vessels still remain among the most common, which is largely due to the lifestyle of modern people. The most common causes of chest pain are:
- angina pectoris;
- myocardial infarction;
- pericarditis.
Angina pectoris
Angina pectoris is one of the clinical forms of coronary heart disease (CHD). It is a consequence of a decrease in the amount of oxygen entering the heart muscle (myocardium) due to impaired blood flow in the arteries (ischemia). This may be the result of the development of atherosclerosis of the coronary arteries, which leads to a decrease in their lumen, spasm of blood vessels or thrombosis and other disorders. The consequence in all cases is a deficiency of oxygen in the myocardium, which provokes the occurrence of characteristic symptoms:
- dull, pressing or pulling pain behind the sternum (sometimes it is localized in the region of the heart), tending to radiate to the left shoulder and the inner surface of the left arm, less often to the neck, right arm and stomach and passes when physical activity stops and the transition to a calm state, so attacks usually last less than 5 minutes;
- dyspnea;
- increased diastolic (lower) blood pressure.
A distinctive sign of angina pectoris is the occurrence of an attack during physical activity, transition from heat to cold, especially in strong winds. But the most pathognomonic symptom is the rapid elimination of pain after taking nitroglycerin.
Myocardial infarction
Myocardial infarction is a condition that requires emergency medical attention. It is a consequence of the progression of coronary artery disease, and in some cases the disease begins with it. This is a severe complication of myocardial ischemia, in which foci of necrosis, i.e., tissue death, form in it. This most often results from rupture of an atherosclerotic plaque. This triggers a whole chain of changes, the result of which is occlusion (blocking) of the coronary artery, which leads to the cessation of nutrition of the corresponding section of the myocardium and the development of ischemic necrosis.
Myocardial infarction is accompanied by severe, excruciating pain behind the sternum, which in nature can be either pressing, bursting or squeezing, or burning, stabbing, or felt like a blow to the heart. It is in many ways similar to an attack of angina, but is much stronger and more often accompanied by a fear of death. The pain is localized in the area behind the sternum and usually spreads to the left, less often it covers the entire surface of the chest and radiates to the stomach, reminiscent of appendicitis, exacerbation of gastric ulcer, etc.
Pain during myocardial infarction radiates to the left shoulder, forearm, hand, and more often it radiates to the little finger and ring finger. They can also radiate to the right hand or to the stomach area, under the shoulder blades, the left side of the neck, jaw, or ear.
The attack can last 15-30 minutes, but more often it drags on for several hours up to 24 hours. In addition to chest pain, this may be accompanied by:
- decreased blood pressure;
- nausea, vomiting;
- shortness of breath;
- severe weakness, combined with increased emotional arousal due to fear of death;
- dizziness;
- cold sweat;
- feeling of heartbeat;
- headache;
- pallor, marbling of the skin;
- tremor.
Shortly before the onset of pain, the following may be observed:
- varying degrees of chest discomfort or pain, as with angina pectoris, but occurring against the background of complete calm or with little physical activity;
- dyspnea;
- weakness;
- dizziness.
Myocardial infarction differs from an attack of angina pectoris in the severity of pain and the duration of its persistence. Also, during a heart attack, taking nitroglycerin leads to only a slight improvement or has no effect at all.
Pericarditis
Pericarditis is a disease accompanied by inflammation of the pericardial sac. Most often, its development is caused by concomitant disorders (viral, bacterial, fungal infections, in particular tuberculosis and borreliosis, as well as metastatic lesions, metabolic disorders), although it can also be a consequence of exposure to ionizing radiation, trauma, or occur in the absence of visible signs. causes (idiopathic pericarditis).
There are acute and chronic pericarditis. In the first case, the following are observed:
- pressing pain in the chest in the area of the heart of varying degrees of intensity, sometimes radiating to the left arm;
- increased pain when taking a deep breath, coughing and swallowing;
- reduction of pain when taking a sitting position, slightly leaning forward, and intensification in a supine position.
With chronic pericarditis, moderate chest pain and shortness of breath are observed. Often, patients previously noticed an increase in body temperature, weakness, muscle discomfort and other typical symptoms of infectious diseases.
With pericarditis, pain is relatively constant, and its severity increases gradually. Taking nitroglycerin does not eliminate the ailment, although NSAIDs (ibuprofen and others) help improve well-being.
Treatment
Help before diagnosis
To eliminate tingling in the chest, you need to know its cause. You can only use non-drug methods on your own. A stabbing sensation of discomfort in the chest is often provoked by stress and overwork, so a person should avoid these factors as much as possible. Physical activity is necessary, but it needs to be dosed so as not to stretch the muscles and cause pain. Stitching pain in the chest is a reason to see a doctor.
Conservative therapy
Tingling in the chest is predominantly of mild or moderate intensity, and therefore does not require the use of analgesics. For painful symptoms, painkillers are used to temporarily relieve the condition. The basis of treatment is etiotropic therapy, which eliminates the cause of tingling. Drugs are selected based on the type of pathology. The following medications are used:
- Anti-inflammatory drugs
. Necessary for a wide range of conditions: from myocarditis and pericarditis to inflammation of the costal cartilages. Representatives of the group of nonsteroidal anti-inflammatory drugs have an additional analgesic effect and quickly relieve unpleasant symptoms. For serious illnesses, therapy is enhanced with corticosteroids. - Medicines affecting the central nervous system
. Recommended for cardioneurosis, depression, intercostal neuralgia. Treatment begins with light sedatives, which, if necessary, are supplemented with antidepressants and tranquilizers. - Antiarrhythmic drugs
. The heart rate is normalized, so the tingling in the chest and the feeling of a sinking heart disappear. Cardiologists select medications of several classes, taking into account the type of arrhythmia and its severity, the presence or absence of other lesions of the cardiovascular system. - Antibiotics
. Used for bronchopulmonary diseases caused by infections. For the treatment of confirmed tuberculosis, special antibiotics taken over long courses are needed. The inclusion of antimicrobial agents in the treatment regimen is justified for rheumatic carditis, acute cholecystitis, and gastritis caused by H. pylori. - Iron supplements
. Prescribed for anemia to increase hemoglobin levels and eliminate symptoms (stabbing sensations in the chest, dizziness, weakness). When red blood counts are low, blood transfusions are indicated, which quickly normalize well-being.
Physiotherapy methods are effective as an addition to pharmacological treatment and can successfully relieve discomfort. For stabbing pain, hydrotherapy, laser therapy, and magnetic therapy are used. Cognitive-behavioral psychotherapy methods can help eliminate the emotional and neurological causes of tingling in the chest. Biofeedback therapy is useful to enhance stress resistance.
Gastrointestinal pathologies
Diseases of the gastrointestinal tract, or more precisely the esophagus, can also provoke the appearance of chest pain. In such cases, they often radiate to the back, to the right and left of the sternum, and in most cases they are associated with food intake and are associated with swallowing disorders.
Swallowing problems are called dysphagia.
Most often, patients with complaints of chest pain are diagnosed with:
- esophageal diverticulum;
- gastroesophageal reflux disease (GERD);
- hiatal hernia;
- spasm of the esophagus (esophagospasm).
Esophageal diverticulum
A diverticulum of the esophagus is a protrusion of its wall with the formation of a kind of “pocket” in which food accumulates. Clinical manifestations of the disease usually occur when the size of the diverticulum is more than 2 cm. In such cases, periodic pain in the sternum and back is observed, as well as regurgitation of chewed food. Sometimes the body temperature also rises to subfebrile levels.
GERD
GERD is a chronic disease accompanied by the reflux of stomach contents into the esophagus, and in some cases, the contents of the duodenum. This causes irritation of the mucous membrane and its inflammation.
With GERD, chest pain is localized in the center and left, which often causes concern in patients. In some cases, they spread to other parts of the sternum. The intensity of pain can vary from mild discomfort to quite severe pain. Their appearance is associated with food, but sometimes they also occur after smoking, and some patients complain of chest pain when they lie down, including at night.
Also with GERD the following may be observed:
- heartburn that occurs when the body bends forward or in a lying position;
- belching of air or food;
- feeling of heaviness, bloating;
- fast saturation;
- dysphagia or pain when swallowing.
A characteristic feature of GERD is the onset of all symptoms directly during or immediately after eating. Also a pathognomonic manifestation is improvement in well-being after taking antacids and changing body position to vertical and walking.
Hiatal hernia
A hiatal hernia means a displacement into the chest cavity of those anatomical structures that should normally be located underneath it, in particular the abdominal segment of the esophagus, the cardia of the stomach, or even intestinal loops. With age, the risk of developing pathology progressively increases; as a result, it is found in 69% of people over 70 years of age.
A diaphragmatic hernia is not always accompanied by chest pain. In fact, very often it is asymptomatic and is discovered by chance during an examination regarding complaints of other disorders of the gastrointestinal tract. But in about 50% of cases, a hiatal hernia leads to pain in the central abdomen just below the ribs, spreading along the esophagus or radiating to the area between the shoulder blades and the back. Less often, they are encircling in nature or localized only behind the sternum, thereby resembling the clinical picture of pancreatitis or angina pectoris, myocardial infarction.
Another symptom of the disease may be heart rhythm disturbances. This leads to fairly frequent diagnostic errors, and therefore the prescription of treatment that does not lead to improvement. To avoid this, it is important to trace the conditions for the onset of pain. The presence of a diaphragmatic hernia is indicated by:
- the appearance of pain after eating, during physical activity, coughing and lying down;
- reduction or complete disappearance of discomfort after belching, taking a deep breath, changing body position, or after the patient drinks a glass of water;
- increased pain when bending forward;
- the occurrence of swallowing disorders, especially when consuming liquid and puree foods, very cold or, conversely, very hot drinks, as well as when rushing while eating.
A hernia is dangerous due to strangulation. In this case, severe cramping pain occurs in the chest, radiating to the back. This is accompanied by nausea, vomiting, often with blood, as well as increased heart rate, decreased blood pressure and shortness of breath.
Also, the disease is often complicated by the development of GERD. Therefore, the characteristic signs of reflux are subsequently added to the existing symptoms.
Esophagospasm
The spasm occurs at the junction of the esophagus and the stomach. This is accompanied by symptoms very similar to those of angina pectoris. The pain can be quite severe. They are localized in the heart area, but can radiate to the neck, lower jaw and shoulders, but unlike angina, they appear during meals and can persist not only for several minutes, but also for hours. This is accompanied by dysphagia and a feeling of difficulty passing food, which can quickly subside after drinking warm drinks, in particular tea or water.
Esophagospasm has a reflex origin and usually accompanies other diseases of the gastrointestinal tract, including GERD, peptic ulcer of the stomach and duodenum, hiatal hernia, cholecystitis, etc.
But esophagospasm can be relieved by taking nitroglycerin, since the esophagus is also formed by smooth muscle fibers.
Diagnostics
Complaints of pain in the sternum are grounds for visiting a general practitioner. The specialist carries out a primary examination to determine the cause of chest pain: collecting data on the time of onset and dynamics of development of the disorder, conducting standard laboratory and clarifying instrumental methods. The greatest diagnostic value is:
- Electrocardiography
. An ECG is necessary to confirm or exclude an ischemic cause of chest pain. Disturbances in the functioning of the heart are indicated by expansion and deformation of the ventricular complexes, changes in the length of intervals, and their shift relative to the isoelectric axis. To exclude pathology of the heart valve apparatus, echocardiography is prescribed. - Radiography
. On a standard x-ray, the OGK looks for signs of widening of the mediastinum and displacement of organs from the center of the sternum. An indirect sign of bronchitis is increased bronchial pattern and deformation of the roots of the lungs. For a detailed study of the identified tumor or granulomatous neoplasm, spiral CT of the chest cavity is used. - Gastroscopy
. Pain that is felt in the middle of the sternum after eating is an indication for endoscopic examination of the esophagus and stomach. In the case of GERD, upon examination, a specialist notices hyperemia and swelling of the esophageal mucosa, erosion or ulcer of the esophagus. The EGDS method is informative for diagnosing destructive processes and ruptures of the esophagus. - Lab tests
. To exclude myocardial infarction, a troponin test is recommended to determine the level of creatine phosphokinase. Multiple bacteriological culture of sputum is necessary if tuberculous lesions of the mediastinal organs are suspected. A standard clinical blood test can detect leukocytosis and the presence of immature cells.
Electrocardiography is a method of differential diagnosis of chest pain
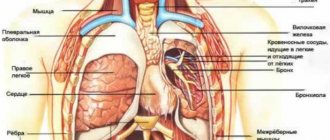
Diseases of the respiratory system
Pathologies of the pleura and pleural cavity, as well as the lungs themselves, can provoke pain in the chest. A distinctive feature of these diseases is the presence of a connection between pain and breathing: it increases with inhalation and decreases with exhalation. This causes an involuntary decrease in breathing rate - it becomes frequent and superficial. Most often, chest pain in such situations is caused by pneumonia, pleurisy, pleural empyema and tumors of the bronchopulmonary localization and pleura.
Pneumonia
Pneumonia is inflammation of the lungs that occurs as a result of damage to the lung tissue by a variety of bacteria, viruses or fungi. Most often, it is a consequence of acute respiratory infections, including infection with a new strain of coronavirus, which is accompanied by a deterioration in the patient’s condition after a temporary improvement.
As a result, pneumonia has typical symptoms characteristic of most respiratory infections:
- rapid increase in body temperature to 38 °C and above;
- chills;
- headache;
- decreased appetite;
- cough is initially dry, and then with sputum, less often hemoptysis;
- dyspnea;
- superficial or deep pain in the chest, which tends to intensify with coughing and breathing;
- muscle weakness, joint discomfort;
- general weakness, depression.
Today, diagnosing pneumonia is not difficult and is usually detected during the initial examination of the patient.
Pleurisy
Pleurisy is inflammation of the pleural layers covering the surface of the lungs and chest wall. This is accompanied by the formation of fibrinous deposits or the accumulation of liquid exudate in the cavity formed by two layers of the pleura. This may be a consequence of an infectious lung infection, in particular tuberculosis, although it also occurs with bacterial, viral and fungal infections of other origins. Also, pleurisy can develop against the background of rheumatism, after myocardial infarction, as well as with gastrointestinal pathologies and in some other cases.
There are dry and exudative pleurisy, and the second form is often a consequence of untimely treatment of dry pleurisy. In such cases the following are observed:
- intermittent chest pain, aggravated by deep breathing, coughing, swallowing, and in some cases, by tilting the body in the opposite direction;
- pain radiating to the stomach, shoulder;
- severe, prolonged hiccups;
- lag of the affected half of the chest when breathing;
- dry cough;
- dyspnea;
- weakness, decreased performance;
- increase in body temperature to subfebrile values;
With pleurisy, there is often a friction noise between the layers of the pleura, which resembles the creaking of snow underfoot. Moreover, if you place your palm on your chest, you can feel their friction.
With exudative pleurisy, pain is present at the beginning of the development of the disease and at the end. But after a sufficient volume of exudate accumulates in the pleural cavity, they disappear. The remaining symptoms are generally similar to those of dry pleurisy.
Empyema of the pleura
Pleural empyema, in fact, is one of the variants of the course of pleurisy, but unlike other forms, it is characterized by the accumulation of pus in the pleural cavity. It can be a consequence of pneumonia (pneumonia), the formation of tumors, cysts, bronchiectasis and other disorders of the lungs, less often in the abdominal organs.
The pathology is characterized by:
- chest pain;
- dyspnea;
- fever;
- chills;
- decreased appetite;
- forced position of the body (lying on the sore side).
The development of pleural empyema requires hospitalization in the surgical department.
Tumors of the lungs and pleura
There are many types of benign and malignant neoplasms that can affect the lungs, bronchi and pleura. They are often accompanied by recurrent pleurisy with constantly increasing pain on the affected side. But direct chest pain caused by a neoplasm, especially a malignant one, occurs after it reaches a large size. This significantly worsens the prognosis, although today there are methods for treating even large tumors that were previously considered inoperable.
Spine pathologies
When chest pain appears, it is difficult to immediately suspect its cause in the development of spinal diseases. Nevertheless, osteochondrosis of the thoracic region and intercostal neuralgia can also make themselves felt in a similar way.
Osteochondrosis of the thoracic spine
Osteochondrosis is the process of dehydration of intervertebral discs and the occurrence of degenerative changes in them. Damage to the thoracic region is much less common than to the cervical or lumbar, and the symptoms are largely reminiscent of angina pectoris and gastrointestinal pathologies. Therefore, patients are often falsely diagnosed with other diseases, and treatment that does not bring results is prescribed.
The risk of developing osteochondrosis directly depends on lifestyle. Therefore, if previously it was mainly found in older people, today it is often detected in young people. Prolonged, regular sitting increases the likelihood of dehydration and progressive degeneration of the discs in the thoracic spine. Therefore, it is most often diagnosed in people who are forced to sit for a long time at a computer, behind the wheel of a car, at a machine, etc.
Osteochondrosis of the thoracic region can manifest itself:
- constant dull pain between the shoulder blades;
- girdle pain localized at the level of the armpits;
- pain in the heart and behind the sternum;
- burning sensation in the back.
A characteristic feature is the occurrence of painful sensations after prolonged sitting, at the end of the working day.
The main danger of osteochondrosis is its steady progression, especially in the absence of comprehensive treatment. As a result, over time, the affected disc, which is a dense cartilage with a jelly-like internal content, becomes deformed and bulges, usually towards the spinal canal. This is called protrusion. Subsequently, it can transform into an intervertebral hernia, which means the final rupture of the outer dense ring of the disc, through which the jelly-like internal contents (nucleus pulposus) can exit into the spinal canal. This is dangerous due to the infringement of the spinal roots passing here and even the spinal cord itself, which will lead to disruptions in the functioning of the internal organs innervated by them, shooting pains, numbness and other sensitivity disorders.
Intercostal neuralgia
Intercostal neuralgia is a consequence of damage to the peripheral nerves passing through the tissues in the area of the intercostal spaces. This may be due to their mechanical compression, herpetic infection, hypothermia, exposure to toxic substances, injuries and other factors.
With intercostal neuralgia, the pain is lumbago-like or burning. They spread along the ribs to the sternum. They can be either short-term or last for hours or even days. When touching the skin in the intercostal spaces, changing body position, walking, deep breathing, coughing, the pain intensifies.
Treatment of thoracic osteochondrosis and its prevention
Conservative treatment of osteochondrosis in the thoracic spine is intended to stop or at least slow down degenerative changes, restore normal back mobility and eliminate symptoms that cause discomfort to the patient.
Therapeutic treatment of thoracic osteochondrosis involves the simultaneous use of:
- medications
(chondroprotectors, neuroprotectors, muscle relaxants, anti-inflammatory drugs, analgesics); - methods of physiotherapeutic complex
; - therapeutic exercises
; - orthopedic regime
.
Patients are also advised to change their diet and lifestyle.
In case of severe irreversible changes in the intervertebral joints , in which pain and nerve conduction disorders are not relieved by medications,
surgery is recommended for patients
. It helps stop the death of nerve tissue and prevent life-threatening or disabling consequences of thoracic osteochondrosis. Depending on the situation, complete or partial resection of the intervertebral disc or its replacement with an artificial one, narrowing of the spinal canal or other surgery may be indicated.
Treatment of thoracic osteochondrosis
Physiotherapy
The objectives of physiotherapy for osteochondrosis of the thoracic region are to reduce pain and inflammation, relieve spasms, strengthen the muscle corset, restore the function of the nerve roots and normal blood circulation.
To relieve the symptoms of thoracic osteochondrosis, the following are successfully used:
- Magnetic therapy
is one of the most effective anti-inflammatory techniques. Improves metabolic processes in tissues and relieves swelling. - Laser therapy
. Promotes biological activation of regenerative processes. Helps eliminate the consequences of trophic disorders and relieve inflammation. - Drug electrophoresis
. Allows you to restore tissue nutrition and relieve inflammation - the effect of the procedure depends on the medications used. - Medicinal phonophoresis
. Ensures deep penetration of the active ingredients of medications into soft tissues. - Massotherapy
. Helps relax muscles, eliminate tension and improve the supply of nutrients to the tissues of the spine. In the early stages, it eliminates the main symptom of thoracic osteochondrosis - a feeling of pain in the sternum - in a few sessions. - Acupuncture
. Stimulation of muscles and nerve endings helps relieve pain, restore sensitivity and eliminate swelling. - Ultrahigh frequency therapy
. Increases the permeability of capillary walls, improves blood flow and ensures the flow of protective cells into the site of inflammation. - Shock wave therapy
. It starts the processes of restoration of bone and cartilage tissue, prevents the deposition of calcium salts on the vertebral surfaces. - Balneotherapy
. As a rule, mud and ozokerite applications are used, less often paraffin. Radon and hydromassage baths are also recommended for patients. They help improve metabolism and restore sensitivity in affected tissues. - Amplipulse therapy
. It has a neurostimulating, analgesic and trophic effect, activates metabolic processes, and facilitates breathing. - Kinesiotherapy
(physical therapy, massage, traction therapy, kinesiotaping). Allows you to strengthen ligaments and skeletal muscles, restore mobility in the back and eliminate even persistent spasticity. Prevents the formation of osteophytes and narrowing of the canals in which the spinal roots are located.
In addition to physical therapy sessions, for the treatment of thoracic osteochondrosis, patients may be recommended an orthopedic corset, which allows them to relieve the load on the spine.
Exercise therapy and massage
Therapeutic exercises and massage help strengthen the back muscles and relieve stress on the spine. With daily sessions, they help achieve stable drug-free remission, increase range of motion, and eliminate neurological manifestations of the disease. These treatment methods also prevent complications of osteochondrosis.
. For example, congestion in the lungs (with thoracic osteochondrosis it is difficult to breathe deeply), due to which patients are susceptible to pneumonia, as well as coronary heart disease.
Dosed physical activity helps relieve compression of the nerve roots, improve blood circulation and nutrition of the intervertebral discs. The optimal frequency and duration of gymnastic classes is determined by the exercise therapy instructor. As a rule, 3-4 exercises of 10-15 minutes a day are enough.
.
The exercises recommended for the treatment of thoracic osteochondrosis include the following:
- Stand straight, feet together, hands at your sides. As you exhale, raise your arms up and bend back, then inhale deeply. Lower your arms and lean forward, slightly arching your back in a dome-shaped manner (to do this, lower your head and shoulders as you exhale).
- Sit on a chair and, while inhaling, place your hands behind your head. Bend back and rest your shoulder blades on the back of the chair, exhaling.
- Get on all fours and arch your back. After maintaining the position for 3 seconds, bend your back with a crampon.
- Lying on the floor on your stomach, place your palms on the floor and, raising yourself on your arms, try to move your head as far back as possible, lifting your chest off the floor.
- Lie on your stomach and extend your arms at your sides. Perform the “yoke” exercise, trying to simultaneously raise your head and legs.
- Sit on the floor and stretch your legs in front of you. Reach the fingers of your right hand to the toe of your left foot and vice versa.
- Do a plank exercise (about 30 seconds).
- Perform hangs on the horizontal bar (or, in the absence of a horizontal bar, secure your fingers on the door frame and try to stretch your back as much as possible).
Bends to the side while raising your arm will also be helpful. All exercises should be performed 8 to 10 times
.
To treat thoracic osteochondrosis, various massage techniques are used, incl. acupressure and vacuum massage. For self-massage at home, patients are recommended the following movements:
- stroking the cervical-collar, scapular and axillary areas
; - squeezing with the thumb and index finger
(grabbing the skin and soft tissues); - trituration
; - kneading
(it should be done extremely carefully, it is advisable to entrust this technique to a specialist).
Massage should not be performed during exacerbations of the disease or during severe inflammation.
Drug treatment of thoracic osteochondrosis
To treat the symptoms of thoracic osteochondrosis, the following groups of drugs are used:
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- help relieve pain, calm inflammation and disperse swelling. They can be used both systemically (in the form of tablets, capsules and injections) and locally (in the form of ointments, gels, creams, compresses and solutions for medicinal electrophoresis). - Hormonal drugs
- to eliminate acute and chronic neurological pain. Used in cases where NSAIDs demonstrate insufficient effectiveness. - Muscle relaxants
are prescribed to reduce muscle tone and eliminate spasms of skeletal muscles. This helps alleviate pain and has a positive effect on tissue trophism. - Blood circulation correctors
- strengthen the walls of blood vessels and improve blood circulation in small capillaries that nourish the periosteum and other structural elements of the vertebral joints. Reduce discomfort and reduce the risk of complications. - Neuroprotectors
- to preserve and restore sensitivity during compression of nerve roots and relieve neurological symptoms. This group also includes cholinesterase inhibitors, which improve nerve impulse transmission and help restore normal muscle tone.
For structural restoration of tissues affected by the degenerative process, the following are used in the treatment of thoracic osteochondrosis:
- chondroprotectors (Artracam)
are essential bioactive substances that trigger the processes of regeneration of cartilage and bone tissue. Serves to prevent the growth of osteophytes and narrowing of the spinal canal. They help a weakened body grow stable and resilient cartilage cells. Taking Artracam significantly improves the shock-absorbing properties of intervertebral discs, making them more elastic and resistant to damage; - vitamin complexes
- help normalize metabolic processes and prevent excess oxidation in tissues.
To relieve excruciating pain that interferes with the patient’s daily activities, the doctor may recommend a medical blockade with anesthetics. Diuretics are used to eliminate swelling and relieve compressed nerves and blood vessels.
Prevention of thoracic osteochondrosis
To prevent symptoms of thoracic osteochondrosis, you should:
- Take care to maintain healthy posture. This is facilitated by walking, swimming and therapeutic exercises to strengthen the muscles of the back, chest, abs, and shoulder complex.
- When working sedentarily, properly arrange your workplace and perform physical warm-up whenever your back and neck begin to become stiff (ideally, bend to the sides, stretch, and rotate your shoulders every 2 hours).
- Avoid back injuries and promptly seek help from an orthopedic traumatologist, even in the case of a seemingly insignificant bruise. Other diseases of the musculoskeletal system should not be triggered, especially in the joints of the lower extremities.
- If possible, unload the spine during the day (to do this, just lie on the floor for 40 minutes).
- Protect yourself from hypothermia and stress.
- Take chondroprotectors to protect joints for at least 3 months a year. Regardless of the strength of the muscular corset, the human spine is anatomically not adapted to vertical loads, and therefore requires additional support.
- Adjust weight if it is overweight. In addition to maintaining a low-carb diet, you should eat a diet high in vitamins and minerals. In the spring-autumn period they can be taken in tablet form.
- Sports activities that involve jumping from heights or lifting heavy weights should be limited.
- It is advisable to sleep on a semi-rigid bed, and for prolonged sitting, choose hard furniture. This helps maintain muscle tone and relieve stress on the spine. If possible, you should purchase an orthopedic mattress and shoe insoles.
- Do not lift loads weighing more than 10 kg. The load should be distributed evenly, with muscle tension and without transferring to one side. If necessary, use a special sports corset. It is undesirable to hold loads in outstretched arms for a long time.
- Women should avoid wearing high-heeled shoes. The optimal heel height is 2-4 cm.
These recommendations will also be useful for those who are already sick - they will have a beneficial effect on the condition of the spine and will help to significantly slow down pathological changes.
And remember: the main thing in the prevention of thoracic osteochondrosis is consistent adherence to healthy habits.
Let chest pain never bother you!
Tactics for determining the cause of chest pain
When discomfort or chest pain occurs, patients often initially turn to a therapist, which is very rational. At the appointment, the doctor initially finds out the nature of the complaints. Much attention is paid to:
- localization of pain (left, right, center or girdling, deep or superficial);
- intensity (the severity of painful sensations is not always equivalent to the existing threat);
- character (squeezing, pressing, dull, aching, stabbing, shooting, etc.);
- conditions of occurrence (during physical activity, eating, transition from heat to cold, at rest, when taking a horizontal position, etc.);
- conditions of termination (after rest, when walking, after eating, drinking, drinking nitroglycerin, when lying on the sick or healthy side, after belching, vomiting);
- duration;
- accompanying symptoms;
- irradiation (in the left arm, neck, jaw, between the shoulder blades, in the stomach, etc.);
- the duration of the pain.
The doctor must find out whether there have been recent injuries to the chest or spine. Mention of such episodes makes it possible to simplify diagnosis and quickly determine the cause of chest pain.
Physical examination
The second stage of diagnosis is a physical examination. It involves sequential execution:
- examination of the skin and mucous membranes for rashes, color changes, and signs of cyanosis;
- assessment of pulse in the radial and femoral arteries;
- blood pressure measurements;
- palpation of the chest, muscles, spinous processes of the vertebrae, identifying symptoms of radicular syndrome;
- percussion (tapping) of the chest;
- auscultation of the heart and lungs (heart sounds are assessed, murmurs, wheezing in the lungs, the sound of pleural friction are detected);
- palpation of the abdomen;
- examination of the lower extremities for signs of varicose veins, thrombophlebitis.
The suspected cause of pain can be detected at any stage of the examination. As a result, the patient receives an appointment for laboratory and instrumental diagnostics.
Prevention recommendations
- Warm up more often, do physical exercise, swimming, yoga or fitness;
- Try to keep your back straight while walking and sitting;
- Avoid drafts, hypothermia, do not swim for a long time even in warm water;
- Avoid excessive physical exertion and lift heavy objects;
- Avoid sharp turns and bends;
- Avoid stressful situations, overwork;
- Monitor your diet and weight;
- Give up bad habits: smoking and alcohol;
- Get a preventative checkup every year.