Pharmacological properties of the drug Depakin
An anticonvulsant, effective in various forms of epilepsy. It is believed that valproate increases the concentration of GABA in the central nervous system by inhibiting the enzyme GABA transferase. The main mechanism of its action is probably due to the enhancement of GABAergic synaptic transmission. In experimental and clinical studies, two mechanisms of the anticonvulsant action of valproate have been identified: • the first is a direct pharmacological effect associated with the concentration of valproate in the blood plasma and brain; • the second is apparently indirect, probably due to metabolites of valproate that remain in the brain, or to modifications of transmitters, or a direct effect on the membrane. The most likely hypothesis is that GABA levels increase after valproate administration. Valproate reduces the duration of the intermediate sleep phase and at the same time increases the slow-wave sleep phase. The bioavailability of sodium valproate when administered orally is about 100%. The volume of distribution is predominantly limited to blood and extracellular fluid. Valproate penetrates into the cerebrospinal fluid and brain. The concentration of valproic acid in the CSF approximately corresponds to the concentration in the blood plasma. The half-life is approximately 8–20 hours and is usually shorter in children. The drug crosses the placenta and is found in small quantities in breast milk (1–10% of the serum concentration). The minimum concentration of valproate in blood serum required for a therapeutic effect is 40–50 mg/l, this concentration ranges from 40–100 mg/l. When the concentration of valproate in the blood serum is above 200 mg/l, a reduction in the dose of the drug is necessary. When administered orally, a steady-state concentration in the blood plasma is achieved quickly - after 3-4 days. Binding to plasma proteins is strong and dose dependent. The valproate molecule can be dialyzed, but only its free form (approximately 10%) is excreted. Sodium valproate is primarily excreted in the urine, after metabolism by glucuroconjugation and beta-oxidation. Unlike other antiepileptic drugs, valproate does not accelerate either its own catabolism or the catabolism of other substances, such as estroprogestogens and oral anticoagulants. This is due to the lack of an inducing effect on enzymes, including cytochrome P450. Compared to the enteric-coated form, Depakine Chrono (sustained release form) in equivalent doses is characterized by the absence of a delay in absorption after administration; prolonged absorption; identical bioavailability; peak total plasma concentration and free substance concentration (Cmax) are lower (decrease in Cmax is about 25%, but with a relatively stable plateau phase from 4 to 14 hours after administration); as a result of using the same dose twice a day, the fluctuation in plasma concentration is reduced by half; more linear correlation between doses and blood concentrations (total and free substance).
Compound
| Long-acting granules | 1 sachet |
| Depakine® Chronosphere™ 100 mg | |
| active substances: | |
| sodium valproate | 66.66 mg |
| valproic acid | 29.03 mg |
| (total in terms of sodium valproate - 100 mg) | |
| excipients: solid paraffin - 101.26 mg; glycerol dibehenate - 106.05 mg; silicon dioxide colloidal aqueous* | |
| Depakine® Chronosphere™ 250 mg | |
| active substances: | |
| sodium valproate | 166.76 mg |
| valproic acid | 72.61 mg |
| (total in terms of sodium valproate - 250 mg) | |
| excipients: solid paraffin - 253.32 mg; glycerol dibehenate - 265.3 mg; silicon dioxide colloidal aqueous* | |
| Depakine® Chronosphere™ 500 mg | |
| active substances: | |
| sodium valproate | 333.3 mg |
| valproic acid | 145.14 mg |
| (total in terms of sodium valproate - 500 mg) | |
| excipients: solid paraffin - 506.31 mg; glycerol dibehenate - 530.25 mg; silicon dioxide colloidal aqueous* | |
| Depakine® Chronosphere™ 750 mg | |
| active substances: | |
| sodium valproate | 500.06 mg |
| valproic acid | 217.75 mg |
| (total in terms of sodium valproate - 750 mg) | |
| excipients: solid paraffin - 759.64 mg; glycerol dibehenate - 795.55 mg; silicon dioxide colloidal aqueous* | |
| Depakine® Chronosphere™ 1000 mg | |
| active substances: | |
| sodium valproate | 666.6 mg |
| valproic acid | 290.27 mg |
| (total in terms of sodium valproate - 1000 mg) | |
| excipients: solid paraffin - 1012.63 mg; glycerol dibehenate - 1060.5 mg; silicon dioxide colloidal aqueous* | |
| * Added by splashing after the melt cooling process and expressed as a percentage of the other four components: 0.7% (approximate amount absorbed on the granules - 0.56%) |
Indications for use of the drug Depakin
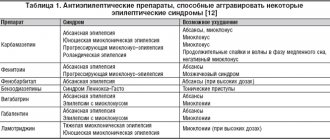
Treatment of generalized or focal epilepsy, especially with the following types of seizures: absences, myoclonic, tonic-clonic, atonic, mixed; for focal epilepsy: simple or combined seizures, secondary generalized seizures, specific syndromes (Vest, Lennox-Gastaut); prevention of seizures during fever in children or in the presence of risk factors for seizure recurrence. Depakine Chrono is also used for the treatment and prevention of manic syndrome in bipolar affective disorders in adults.
Nosological classification (ICD-10)
- F31 Bipolar affective disorder
- G25.3 Myoclonus
- G40 Epilepsy
- G40.0 Localized (focal) (partial) idiopathic epilepsy and epileptic syndromes with seizures with focal onset
- G40.1 Localized (focal) (partial) symptomatic epilepsy and epileptic syndromes with simple partial seizures
- G40.2 Localized (focal) (partial) symptomatic epilepsy and epileptic syndromes with complex partial seizures
- G40.3 Generalized idiopathic epilepsy and epileptic syndromes
- G40.4 Other types of generalized epilepsy and epileptic syndromes
- G40.6 Grand mal seizures, unspecified [with or without petit mal seizures]
- G40.8 Other specified forms of epilepsy
- G40.9 Epilepsy, unspecified
- R56.0 Convulsions during fever
Use of the drug Depakine
The dose is set taking into account the patient’s age, body weight and individual sensitivity to the drug. The optimal dose is determined depending on the clinical effect. Determination of the concentration of valproic acid in the blood plasma is carried out in addition to clinical observation in cases where it is not possible to achieve adequate control of seizures, or in cases of threat of side effects. The effective concentration of the drug in the blood is usually 40-100 mg/l (300-700 µmol/l). The drug is taken orally, preferably during meals, without chewing the tablets. The daily dose is recommended to be taken in one or two doses. One-time use is possible for well-controlled epilepsy. When replacing the enteric immediate-release form of valproate, which provided disease control, with a sustained-release form, the daily dose should be maintained. At the beginning of treatment for patients not taking other antiepileptic drugs, the dose is increased after 2-3 days to reach the optimal dose within approximately 1 week. The optimal dose in patients who are already taking antiepileptic drugs replaced by Depakine is achieved gradually, over about 2 weeks. In this case, the dose of the previous drug is gradually reduced, and then its use is stopped. If it is necessary to use other antiepileptic drugs, they are added gradually. The initial daily dose is usually 10–15 mg/kg, then it is gradually increased to the optimal dose, which is usually 20–30 mg/kg. However, if the seizures do not stop, the dose can be increased. Careful monitoring of patients receiving the drug in doses above 50 mg/kg is necessary. For children weighing over 6 kg, the average daily dose is approximately 30 mg/kg (it is better to use the syrup form). For children under 1 year of age, it is recommended to divide the daily dose into 2 doses, for children over 1 year - into 3 doses. For adolescents and adults, the average daily dose is 20–30 mg/kg. In elderly patients, the dose is set taking into account the clinical situation.
Use during pregnancy and breastfeeding
Risk associated with developing epileptic seizures during pregnancy
During pregnancy, the development of generalized tonic-clonic epileptic seizures, status epilepticus with the development of hypoxia may pose a particular risk for both the mother and the fetus, due to the possibility of death.
Risk associated with the use of Depakine® Chronosphere™ during pregnancy
Experimental reproductive toxicity studies conducted in mice, rats and rabbits have demonstrated that valproic acid is teratogenic.
Congenital malformations
Available clinical data have demonstrated a higher incidence of minor and severe malformations, in particular, congenital neural tube defects, craniofacial deformities, malformations of the limbs and CVS, hypospadias, and multiple malformations affecting different organ systems in children born to mothers who took valproic acid during pregnancy, compared with their frequency when taking a number of other antiepileptic drugs during pregnancy. Thus, the risk of congenital malformations in children born to mothers with epilepsy who received valproic acid monotherapy during pregnancy was approximately 1.5, 2.3, 2.3 and 3.7 times higher compared with phenytoin monotherapy , carbamazepine, phenobarbital and lamotrigine, respectively.
Data from a meta-analysis that included registry and cohort studies showed that the incidence of congenital malformations in children born to mothers with epilepsy who received valproic acid monotherapy during pregnancy was 10.73% (95% CI 8.16– 13.29%). This risk is greater than the 2–3% risk of major congenital malformations in the general population. This risk is dose-dependent, but it is not possible to establish a threshold dose below which such a risk does not exist.
Mental and physical development disorders
It has been shown that prenatal exposure to valproic acid may have adverse effects on the mental and physical development of exposed children. This risk appears to be dose-dependent, but it is not possible to establish a threshold dose below which such a risk does not exist. The exact gestational period for the risk of developing these effects has not been established, and risk is possible throughout pregnancy.
Studies of preschool children exposed in utero to valproic acid have shown that up to 30–40% of these children had early developmental delays (such as delayed gait and speech delays), as well as lower intellectual abilities, poor language skills (intrinsic speech and speech understanding) and memory problems.
Intelligence quotient (IQ) scores measured in children aged 6 years with a history of prenatal exposure to valproic acid were on average 7 to 10 points lower than in children exposed prenatally to other antiepileptic drugs. Although the role of other factors that could adversely affect the intellectual development of children exposed to valproic acid in utero cannot be ruled out, it is clear that in such children the risk of intellectual impairment may be independent of maternal IQ. Data on long-term outcomes are limited.
There is evidence that children exposed to valproic acid in utero have an increased risk of developing autistic spectrum disorders (approximately 3- to 5-fold increased risk), including childhood autism. Limited evidence suggests that children exposed to valproic acid in utero are more likely to develop attention-deficit/hyperactivity disorder (ADHD).
Both valproic acid monotherapy and combination therapy containing valproic acid are associated with adverse pregnancy outcomes, but combination antiepileptic therapy containing valproic acid has been reported to be associated with a higher risk of adverse pregnancy outcome compared with valproic acid monotherapy (i.e. e. the risk of developing disorders in the fetus is less when using valproic acid in monotherapy).
Risk factors for fetal malformations are: a dose of more than 1000 mg/day (however, a lower dose does not eliminate this risk) and the combination of valproic acid with other anticonvulsants.
In connection with the above, the drug Depakine® Chronosphere™ should not be used during pregnancy and in women of childbearing potential unless absolutely necessary, i.e. its use is possible in situations where other antiepileptic drugs are ineffective or the patient cannot tolerate them.
The question of the need to use the drug Depakine® Chronosphere™ or the possibility of refusing its use should be resolved before starting use or reviewed if a woman taking Depakine® Chronosphere™ is planning a pregnancy.
Women of childbearing potential should use effective methods of contraception during treatment with Depakine® Chronosphere™.
Women of childbearing potential should be informed of the risks and benefits of using valproic acid during pregnancy.
If a woman is planning or has been diagnosed with pregnancy, the need for treatment with valproic acid should be re-evaluated depending on the indication:
- if bipolar disorder is indicated, discontinuation of treatment with valproic acid should be considered (see below);
- if epilepsy is indicated, the question of continuing treatment with valproic acid or its discontinuation is decided after reassessing the benefit-risk ratio. If, after reassessing the balance of benefit and risk, treatment with valproic acid must still be continued during pregnancy, it is recommended to use it in the lowest effective daily dose, divided into several doses. It should be noted that during pregnancy, the use of extended-release dosage forms of the drug is more preferable than other dosage forms.
If possible, even before pregnancy, you should additionally start taking folic acid (at a dose of 5 mg/day), because Folic acid may reduce the risk of neural tube defects. However, currently available data do not support its preventive effect against congenital malformations caused by valproic acid.
Special prenatal diagnostics, including detailed ultrasound, should be carried out on an ongoing basis (including in the third trimester of pregnancy) to identify possible defects in the formation of the neural tube or other malformations of the fetus.
Risk to newborns
Isolated cases of hemorrhagic syndrome have been reported in newborns whose mothers took valproic acid during pregnancy. This hemorrhagic syndrome is associated with hypofibrinogenemia and/or decreased levels of other coagulation factors. The development of afibrinogenemia, which could be fatal, has also been reported. This hemorrhagic syndrome should be distinguished from vitamin K deficiency caused by phenobarbital and other inducers of microsomal liver enzymes.
Therefore, in newborns whose mothers were treated with valproic acid during pregnancy, coagulation tests should be performed (determining the number of platelets in peripheral blood, plasma concentration of fibrinogen, coagulation factors and coagulogram).
Cases of hypoglycemia have been reported in newborns whose mothers took valproic acid during the third trimester of pregnancy.
Cases of hypothyroidism have been reported in newborns whose mothers took valproic acid during pregnancy.
Newborns whose mothers took valproic acid in the last trimester of pregnancy may experience withdrawal symptoms (including agitation, irritability, hyperreflexia, tremors, hyperkinesia, muscle tone disorders, tremor, seizures and feeding difficulties).
Breastfeeding period
Excretion of valproic acid into breast milk is low, its concentration in milk is 1–10% of the concentration in serum.
There are limited clinical data on the use of valproic acid during breastfeeding, and therefore the use of the drug during this period is not recommended.
Based on the literature data and limited clinical experience, the issue of breastfeeding can be considered during monotherapy with Depakin® Chronosphere™, but the side effect profile of the drug, especially the hematological disorders it causes, should be taken into account.
Fertility. Due to the possibility of developing dysmenorrhea, amenorrhea, polycystic ovaries, an increase in the concentration of testosterone in the blood, a decrease in fertility in women is possible (see “Side effects”). In men, valproic acid can reduce sperm motility and impair fertility (see “Side Effects”). These fertility problems have been found to be reversible after cessation of treatment.
Side effects of the drug Depakin
Allergic reactions (exanthematous rash), in extremely rare cases - toxic epidermal necrosis, Stevens-Johnson syndrome, erythema multiforme, confusion, very rarely - stupor or lethargy, sometimes leading to transient coma (may be isolated or associated with an increased frequency of seizures during duration of therapy; their severity decreases after discontinuation or when the dose of the drug is reduced; most often, such effects occur during complex treatment, especially with phenobarbital, or after a sharp increase in the dose of valproate); very rarely - reversible dementia associated with reversible cerebral atrophy, which disappears several weeks or months after discontinuation of the drug, rarely - reversible parkinsonism; nausea, vomiting, stomach pain, diarrhea (often appear at the beginning of treatment in some patients, they usually go away on their own within a few days without stopping the drug); moderate hyperammonemia, which does not cause changes in liver function and does not require discontinuation of the drug (in case of hyperammonemia associated with neurological symptoms, further examination of the patient is necessary; the risk of hyperammonemia increases when using the drug in patients with a deficiency of carbamide cycle enzymes; cases of hyperammonemia accompanied by stupor and coma in such patients); decreased fibrinogen levels or increased bleeding time, usually without associated clinical symptoms; often - thrombocytopenia, rarely - anemia, macrocytosis and leukopenia, extremely rarely - pancytopenia; hair loss, mild hand tremors and drowsiness (transient in nature and/or dependent on the dose of the drug) ; vasculitis; headache; weight gain; rarely - hearing loss (both reversible and irreversible); reversible Fanconi syndrome; rarely - impaired renal function, peripheral edema, amenorrhea and irregular menstrual cycle; liver dysfunction (rare reports). Conditions for the occurrence of liver dysfunction With complex anticonvulsant therapy, a group at increased risk of developing hepatitis includes infants and children under 3 years of age with severe epilepsy, especially associated with brain damage, mental retardation and/or metabolic or degenerative diseases of genetic origin. In children over 3 years of age, the incidence of such complications is significantly reduced. In the vast majority of cases, severe reactions from the liver are observed during the first 6 months of treatment, usually between the 2nd and 12th weeks, and more often with complex antiepileptic treatment. Pancreatitis. In extremely rare cases, when taking valproate, severe forms of pancreatitis were noted, which in some cases led to death. Children under 3 years of age are at particular risk. This risk decreases with age. Risk factors may include severe epileptic seizures, neurological impairment, or anticonvulsant therapy. Liver disorders associated with pancreatitis increase the risk of death. Possible signs of liver dysfunction Early diagnosis is based primarily on clinical examination. First of all, the symptoms that may precede jaundice should be taken into account, especially in patients at risk: • nonspecific symptoms, usually appearing suddenly: asthenia, anorexia, fatigue, drowsiness, sometimes accompanied by repeated vomiting and abdominal pain; • recurrence of epileptic seizures. It is recommended to inform the patient (or the child’s parents) that if such clinical symptoms appear, it is necessary to urgently consult a doctor for advice and immediately conduct a clinical examination, including a liver function test. Detection of liver dysfunction It is necessary to check liver function before starting treatment and periodically during the first 6 months of treatment, especially in patients at risk . The most important are tests reflecting the protein-synthetic function of the liver and especially the prothrombin index. If an abnormally low level of prothrombin is detected, especially accompanied by a significant decrease in the level of fibrinogen and blood clotting factors, an increase in the level of bilirubin and transaminases, treatment with valproate should be suspended. If salicylates were included in the treatment regimen, then, as a precaution, their use should also be stopped (since salicylates use the same metabolic pathways as valproate).
Special instructions for the use of the drug Depakin
The active substance Depakine in the human body is converted into valproic acid, so other drugs that undergo the same transformation should not be used simultaneously in order to avoid an overdose of valproic acid (for example, divalproate, valpromide). Early diagnosis of liver damage when using the drug is based primarily on clinical examination. Great attention should be paid to symptoms that may precede jaundice, especially in patients at risk: nonspecific symptoms, usually appearing suddenly - asthenia, anorexia, fatigue, drowsiness, sometimes accompanied by repeated vomiting and abdominal pain; increased frequency of epileptic seizures. It is recommended to inform the patient (or the child's parents) that if such clinical symptoms appear, it is necessary to urgently consult a doctor for advice and immediately conduct a clinical examination, including a liver function test. When treated with Depakine, as with other antiepileptic drugs, especially at the beginning of treatment, a slight isolated and temporary increase in the level of liver enzymes may be observed, without any clinical symptoms. In this case, it is recommended to conduct a more complete laboratory examination (including, in particular, determination of the prothrombin index) in order to revise the dose, if necessary, and repeat the tests in accordance with changes in parameters. For children under 3 years of age, the use of valproate as monotherapy is recommended, after establishing the effectiveness of its therapeutic action, since these patients represent a risk group for developing liver disease or pancreatitis . Concomitant use of valproate with salicylates should be avoided in children under 3 years of age due to the risk of developing liver disease. Before starting therapy or surgery, in case of spontaneous hematomas or bleeding, it is recommended to conduct a blood test (determine the blood count, including platelet count, bleeding time and coagulation tests) . In patients with renal failure, it may be necessary to reduce the dose. Since monitoring plasma concentrations of the drug may lead to erroneous conclusions, the dose should be adjusted according to clinical response . Acute abdominal pain and gastrointestinal symptoms such as nausea, vomiting and/or anorexia require immediate medical attention. In case of pancreatitis, Depakin should be discontinued. If a deficiency of carbamide cycle enzymes is suspected, metabolic studies should be performed before starting treatment with Depakin, due to the risk of hyperammonemia. In children with unexplained hepatodigestive symptoms (anorexia, vomiting, cases of cytolysis), a history of lethargy or coma, with mental retardation, cases of death of a newborn or child in the family history, before starting treatment with Depakine, it is necessary to conduct a metabolic study, especially ammonemia during fasting and after administration food. Although dysfunction of the immune system rarely occurs during treatment with Depakine, the possible benefits of its use must be compared with the potential risks when prescribing the drug to patients with systemic lupus erythematosus. Patients should be warned about the possibility of weight gain at the beginning of treatment, and, to avoid this, the need to follow a diet. Children under the age of 6 years are not recommended to use Depakine Chrono due to the risk of it entering the respiratory tract when swallowed. The use of an antiepileptic drug may sometimes be accompanied by the resumption or development of new types of seizures in the patient, regardless of the spontaneous fluctuations observed in some epileptic conditions. In relation to Depakine Chrono, this primarily concerns modification of concurrent antiepileptic treatment or pharmacokinetic interactions, toxicity (hepato- or encephalopathy) and overdose. Pregnancy period . When using any antiepileptic drugs in women with epilepsy, the overall incidence of congenital defects in children born to them is 2–3 times higher than among the general population (about 3%). Although an increase in the number of children with congenital defects has been observed with the use of combination therapy, the respective role of the disease itself and the drugs taken by the mother has not yet been established. The most common malformations are cleft lip and malformations of the cardiovascular system. Sudden interruption of antiepileptic treatment may worsen the course of the mother's illness and lead to detrimental consequences for the fetus. Experimental studies on mice, rats and rabbits showed the teratogenic effect of the drug. Cases of facial dysmorphia have been described. Multiple malformations, especially of the limbs, were rarely noted. The frequency of such effects has not yet been precisely established. Along with this, Depakine predominantly causes a disorder in the development of the neural tube: myelomeningocele, vertebral bifida. The incidence of such complications is 1–2%. In some cases, facial dysmorphia and malformations of the limbs (especially shortening of the limbs) were observed. The frequency of such complications has not yet been precisely established. If a woman taking Depakine is planning a pregnancy, the indications for antiepileptic treatment should be reconsidered. During pregnancy, effective antiepileptic treatment with Depakin should not be interrupted; monotherapy is recommended in the minimum effective dose, which is divided into several doses per day. The validity of preventing developmental disorders of the neural tube using folic acid has not yet been confirmed. Therefore, regardless of whether the patient takes foliates or not, a special prenatal examination of the patient is necessary in order to identify disorders of the neural tube or other abnormalities of fetal development during the first months of pregnancy. In newborns whose mothers took Depakine during pregnancy, hemorrhagic syndrome may occur, probably associated with hypofibrinogenemia, which may be caused by a decrease in coagulation factors. Afibrinogenemia, which can be fatal, has been observed. However, this syndrome must be distinguished from a decrease in vitamin K-dependent factors caused by the use of phenobarbital and other enzyme inducers. Therefore, in pregnant women before childbirth, as well as in newborns, it is necessary to analyze the platelet count, the level of fibrinogen in the serum, and coagulation tests to determine coagulation factors. Birth trauma may increase the risk of bleeding. Breastfeeding period . Excretion of valproate into breast milk is low. To date, only one case of thrombocytopenia in a three-month-old child is known, which manifested itself after stopping breastfeeding. There is no evidence of any significant adverse clinical symptoms in children who were breastfed while their mother was using Depakine. Therefore, you can consider the possibility of breastfeeding while taking the drug as monotherapy, taking into account the possibility of its side effects, especially hematological and liver dysfunction. Impact on the ability to drive a car and perform work that requires increased attention . The patient should be warned about the possibility of drowsiness, especially in the case of combined anticonvulsant therapy or a combination of Depakine with benzodiazepines.
Depakine chrono 500 mg No. 30 tablets
Depakine chrono 500 mg No. 30 tablets
Trade name Depakine Chrono International nonproprietary name Valproic acid Dosage form Film -coated tablets, prolonged action, divisible, 500 mg Composition One tablet contains active substances: sodium valproate 333 mg, valproic acid 145 mg, excipients: hypromellose 4000 (3000 mPa.s), ethylcellulose 20 mPa.s, sodium saccharinate, colloidal silicon dioxide anhydrous, colloidal silicon dioxide aqueous, shell composition: hypromellose (6 mPa.s), macrogol 6000, talc, titanium dioxide (E171), polyacrylate 30% dispersion or dry extract . Description Tablets are oblong in shape with hemispherical edges, almost white in color with a biconvex surface, film-coated, scored on both sides, practically odorless or with a slight odor. Pharmacotherapeutic group Antiepileptic drugs. Fatty acid derivatives. ATC code N03AG01 Pharmacological properties Pharmacokinetics The bioavailability of valproate in the blood when taken orally is close to 100%. The drug is distributed mostly into the systemic circulation and into the extracellular fluid. Valproate penetrates into the cerebrospinal fluid and brain tissue. The half-life is 15-17 hours. For a therapeutic effect, a minimum serum concentration of 40-50 mg/l is required, ranging from 40-100 mg/l. If higher plasma concentrations are required, the benefits must be weighed against the risk of adverse effects, especially dose-related ones. Despite this, if concentrations persist at levels above 150 mg/l, the dose should be reduced. Steady-state concentrations in blood plasma are achieved within 3-4 days. Binding to blood proteins is dose-dependent and saturable. Valproate is metabolized by glucuron conjugation and beta-oxidation, then excreted, mainly in the urine. Can be dialyzed; however, hemodialysis is effective only on the free fraction of valproate in the blood (approximately 10%). Valproate does not induce enzymes involved in the cytochrome P450 metabolic system. Unlike most other antiepileptic drugs, it does not accelerate either its own degradation or that of other substances such as estrogen-progestogens and oral anticoagulants. When compared with the gastroresistant dosage form of valproate, the extended release dosage form at the same doses is characterized by the disappearance of the absorption lag period, prolonged absorption, identical bioavailability, lower total maximum concentration and plasma concentration of free substance (Cmax lower by approximately 25% with a relatively stable plateau 4–14 hours after administration); this "peak-flattening" effect provides a more constant and more evenly distributed concentration of valproic acid over a 24-hour period: after administration of the same dose twice daily, the amplitude of fluctuations in plasma concentrations is reduced by half, a linear relationship between dose and plasma concentration (total and free substance) is more pronounced. Pharmacodynamics Depakine Chrono acts primarily on the central nervous system. The anticonvulsant effect of Depakine Chrono is manifested against various types of convulsive seizures of epilepsy in humans. Depakine Chrono has two types of anticonvulsant action: the first type is a direct pharmacological effect associated with the concentrations of Depakine Chrono in plasma and brain tissues, the second type of action is indirect and is probably associated with valproate metabolites located in brain tissues, or with changes neurotransmitters or direct effects on the membrane. The most widely accepted hypothesis relates to the level of gamma-aminobutyric acid (GABA), which increases after the use of Depakine Chrono. Depakine Chrono reduces the duration of the intermediate phase of sleep while simultaneously increasing its slow-wave component. Indications for use : treatment of epilepsy in adults and children as monotherapy or in combination with other antiepileptic drugs for both generalized seizures (clonic, tonic, tono-clonic, absence, myoclonic and atonic seizures; Lennox-Gastaut syndrome) and focal epilepsy (focal seizures with or without secondary generalization) - treatment of manic syndrome in adults with bipolar disorders and prevention of relapses, manic episodes in which were amenable to treatment with Depakin Chrono. Method of administration and dosage Depakine Chrono is a prolonged-release dosage form of Depakine with a reduced maximum plasma concentration, providing a more even plasma concentration over a 24-hour period. Based on the amount of active substance, this medicinal product is intended for use by adults and children weighing more than 17 kg. This dosage form is not suitable for children under 6 years of age (respiratory hazard). Directions for use : For oral administration. The daily dose should be taken 1 time per day or divided into 2 doses per day, preferably taken with meals. Once daily dosing is possible if epilepsy is well controlled. The tablet is swallowed whole, without biting or chewing. Dosage for generalized and focal epilepsy The initial daily dose is 10-15 mg/kg, then the dose is increased to the optimal (see “Start of treatment”). Average dose: 20 - 30 mg/kg per day. However, if seizures cannot be treated with these doses, then with strict monitoring of the patient, the dose can be increased. For children 6 years and older: the average dose is 30 mg/kg per day. For adults: average dose 20 - 30 mg/kg per day. In elderly patients, the dose should be adjusted according to the clinical condition. The daily dose should be prescribed based on age and body weight, taking into account the wide range of individual sensitivity to valproate. The exact relationship between the daily dose, blood concentration and therapeutic effect has not been established: the dose is selected based on clinical response. In cases of uncontrolled seizures or suspected adverse reactions, measurement of plasma levels of valproic acid may be necessary along with clinical monitoring. The therapeutic effect is usually observed at concentrations of 40-100 mg/l (300 - 700 µmol/l). Initiation of treatment For patients in whom adequate control of seizures is achieved using immediate-release dosage forms of Depakine, the daily dose remains unchanged when replacing it with Depakine Chrono. For patients already under treatment and taking another antiepileptic drug, Depakin Chrono is administered gradually, so that after approximately 2 weeks the optimal dose is reached; then, if necessary, reduce concomitant treatment depending on the effectiveness of treatment. For patients not taking other antiepileptic drugs, it is advisable to increase the dose in stages, every 2-3 days, in order to achieve the optimal dose after about one week. If necessary, additional prescription of other antiepileptic drugs is carried out gradually. Dosage for the treatment of mania in bipolar disorders The recommended starting dose is 20 mg/kg/day. This dose should be increased as soon as possible to achieve the minimum therapeutic dose that will provide the desired clinical effect. This effect can generally be obtained at plasma valproate levels between 45 and 125 mcg/mL. The recommended maintenance dose for bipolar disorders is 1000 - 2000 mg per day. In exceptional cases, the dose can be increased to a maximum of 3000 mg per day. The dose is selected based on individual clinical response. The duration of the course is determined individually by the doctor. Dosage for the prevention of relapse of mania in bipolar disorders To avoid relapse, the dose to be prescribed should be the lowest dose that provides adequate control of the acute symptoms of mania in the individual patient. The maximum daily dose of 3000 mg should not be exceeded. Side effects - congenital, familial or genetic disorders, due to teratogenic risk (see section "Special Instructions") - bone marrow aplasia and true erythrocyte aplasia - agranulocytosis - dose-dependent thrombocytopenia observed without any clinical consequences In asymptomatic thrombocytopenia, only Reducing the dose of this drug, if possible, based on platelet counts and while the epilepsy is effectively controlled, will usually result in resolution of the thrombocytopenia. - temporary and (or) dose-dependent undesirable effects: minor postural tremor and drowsiness - confusion or convulsions - stupor or lethargy, sometimes leading to temporary coma (encephalopathy), either isolated or associated with a paradoxical increase in seizures with valproate, regressing upon cessation treatment or after dose reduction Such conditions occur most often with drug polytherapy (especially with phenobarbital or topiramate) or after a sharp increase in the dose of valproate. - hyperammonemia, occurring with neurological symptoms (up to coma) and requiring additional tests - headache - the appearance of gastrointestinal disorders at the beginning of treatment (nausea, vomiting, stomach pain, diarrhea), which usually resolve after a few days without discontinuation drug - temporary and/or dose-dependent hair loss - skin reactions such as exanthematous rash - syndrome of inappropriate secretion of antidiuretic hormone (SIAD) - weight gain, which is a risk factor for polycystic ovary syndrome - careful monitoring of patients' body weight is necessary - Quincke's edema , drug rash syndrome with eosinophilia and systemic symptoms (LSESS syndrome) or hypersensitivity syndrome - liver disease - amenorrhea, menstrual irregularities Often - especially with drug polytherapy, isolated moderate hyperammonemia without changes in laboratory tests of liver function, which does not require Changes in the drug Sometimes - ataxia Rarely - reversible Parkinson's syndrome Very rarely - cognitive impairment with a latent and progressive onset, which can progress to complete dementia and is reversible several weeks or months after discontinuation of treatment - pancreatitis, requiring premature cessation of treatment, sometimes fatal outcome - enuresis and urinary incontinence - hyponatremia - mild peripheral edema In exceptional cases - reversible and irreversible hearing loss - Lyell's syndrome, Stevens-Johnson syndrome and erythema multiforme - kidney damage - decreased fibrinogen levels or increased bleeding time, usually without associated clinical symptoms, when taking large doses of Depakine Chrono has an inhibitory effect on the second phase of platelet aggregation. Less frequently reported cases of anemia, macrocytosis, leukopenia and, in exceptional cases, pancytopenia. Contraindications - history of hypersensitivity to valproate, divalproate, valpromide or any of the components of the drug - acute and chronic hepatitis - cases of severe hepatitis in the patient's personal or family history, including those caused by drugs - hepatic porphyria - combined use with mefloquine - combined use with St. John's wort - children under 6 years of age Drug interactions The simultaneous use of drugs that provoke seizures or drugs that reduce the threshold of brain excitability should be taken into account with all seriousness due to the severity of the potential danger. These include most antidepressants (imipramines, selective serotonin reuptake inhibitors), antipsychotics (phenothiazines and butyrophenones), mefloquine, chloroquine, bupropion and tramadol. Contraindicated combinations Mefloquine (an antimalarial drug) increases the metabolism of valproic acid and may cause seizures. Therefore, during combination therapy, epileptic seizures may occur. St. John's wort poses a risk of reducing the concentration of valproic acid in the blood plasma and its therapeutic effectiveness. Combinations not recommended Lamotrigine: increased risk of severe skin reactions (Lyell's syndrome). In addition, it is possible to increase the concentration of lamotrigine in the blood plasma (its metabolism is slowed down by sodium valproate). If the combination proves necessary, close clinical monitoring is required. Combinations requiring special precautions Aztreonam, imipenem, meropenem cause the risk of seizures due to a decrease in the concentration of valproic acid in the blood serum. Clinical observation, determination of drug concentrations in blood plasma and, possibly, a revision of the dosage of valproic acid during treatment with antibacterial drugs and after their discontinuation are required. Carbamazepine: Depakine Chrono causes an increase in plasma concentrations of the active metabolite of carbamazepine with signs of overdose. In addition, a decrease in plasma concentrations of valproic acid is possible as a result of carbamazepine stimulation of hepatic metabolism. Clinical monitoring, determination of plasma concentrations and, if necessary, dose adjustment of both anticonvulsants are recommended. Felbamate causes an increase in the concentration of valproic acid in the blood serum, risk of overdose. Clinical monitoring and laboratory monitoring and, possibly, a revision of the dosage of Depakine Chrono during treatment with felbamate and after its discontinuation are necessary. Phenobarbital (and by extrapolation - primidone): increased phenobarbital in blood plasma with signs of overdose in children. In addition, plasma concentrations of valproic acid are reduced due to increased hepatic metabolism under the influence of phenobarbital. Therefore, clinical monitoring is recommended during the first 15 days of combination treatment, with immediate reduction of the phenobarbital dose if signs of drowsiness occur. If necessary, determine the plasma levels of both drugs in the blood. Phenytoin (and by extrapolation - fosphenytoin): changes in the concentration of phenytoin in the blood plasma. In addition, there is a risk of decreased plasma concentrations of valproic acid as a result of phenytoin enhancing its metabolism in the liver. Therefore, clinical monitoring, measurement of plasma concentrations and dose adjustment of both anticonvulsants is recommended. Topiramate: There is a risk of developing hyperammonemia or encephalopathy, usually associated with valproic acid, when administered concomitantly with topiramate. It is necessary to strengthen clinical and laboratory monitoring of ammonemia at the beginning of treatment if symptoms indicating it appear. Rifampicin: Risk of seizures due to increased hepatic metabolism of valproate by rifampicin. Clinical and laboratory monitoring is recommended, and dose adjustment of the anticonvulsant drug is possible during treatment with rifampicin and after its discontinuation. Zidovudine: there is a risk of increased adverse reactions to zidovudine, in particular hematological effects, due to decreased metabolism under the influence of valproic acid. Regular clinical and laboratory monitoring is necessary. Blood counts should be checked to detect anemia during the first two months of use of the combination. Combinations that should be taken into account Nimodipine (for oral and, by extrapolation, injection): risk of increasing the hypotensive effect of nimodipine due to an increase in its concentration in the blood plasma (valproic acid suppresses its metabolism). Other forms of interaction Oral contraceptives: Depakine Chrono does not have an enzyme-inducing effect and, therefore, does not reduce the effectiveness of estrogen-progestogen hormonal contraceptives. Special instructions In rare cases (regardless of the spontaneous fluctuations observed in some types of epilepsy), after taking an antiepileptic drug, an increase in seizures or the development of a new type of seizures is possible. This may be the result of a pharmacokinetic interaction between two or more antiepileptic drugs used simultaneously, toxicity (due to liver dysfunction or encephalopathy), or overdose. Since this drug is converted into valproic acid in the body, it should not be used simultaneously with other drugs that are subjected to the same transformation in order to avoid overdose of valproic acid (for example, sofa, valPapromide). Disorders of the liver function Conditions: There are exceptional cases of liver damage with severe and sometimes death. An increased risk group is made up of babies and children under 3 years old with severe epilepsy associated with damage to the brain, mental retardation and (or) congenital disorders of metabolism or degenerative disease. At the age of older than 3 years, the frequency of such complications is significantly reduced. In the vast majority of cases, such a liver damage is observed in the first 6 months of treatment, usually between 2 and 12 weeks, and, as a rule, during political therapy with antiepileptic agents. Signs-subjects: early diagnosis is based mainly on the clinical picture of the disease. In particular, you should pay attention to two types of symptoms that can precede the development of jaundice, especially in patients with the risk group (see “conditions of occurrence”):-firstly, non-specific systemic features, as a rule, with sudden appearance, such as asthenia, anorexia, a breakdown, drowsiness, sometimes accompanied by repeated vomiting and abdominal pain; -Secondly, relapses of epileptic seizures, despite the exact observance of treatment. It is recommended to inform the patient or his family, if this is a child, that they should urgently consult a doctor in the case of a clinical picture of this type. In addition to a physical examination, a laboratory analysis of the liver function should be carried out immediately. Identification: during the first 6 months of treatment, periodic control of the liver function is necessary. Among the standard tests, analyzes that reflect the state of protein synthesis and, in particular, prothrombin time (PV) are most important. When confirming pathologically low PV indicators, especially if there are other deviations from the norm in laboratory indicators (a significant decrease in the level of fibrinogen and blood coagulation factors, an increase in bilirubin levels, increasing transaminase activity), it is necessary to stop treatment (and as a precaution is a precautionary to stop treatment Salicylate derivatives, if any are prescribed simultaneously, since their metabolism is carried out in the same way). Pancreatitis is known extremely rare cases of pancreatitis, sometimes death. Pancreatitis can be observed regardless of the age of the patient and the duration of treatment, while young children are at risk to the highest degree. Pancreatitis with an adverse outcome, is usually observed in young children and in patients with a severe form of epilepsy, with brain damage or against the background of polytherapy with antiepileptic agents. The risk of fatal outcome is higher with pancreatitis against the background of liver failure. With the appearance of acute abdominal pain, nausea, vomiting and/or anorexia should take into account the possibility of the development of pancreatitis; In the case of increasing the levels of pancreatic enzymes, treatment should be canceled and prescribed another necessary treatment. The risk of suicide suicide thoughts and behavior were observed in patients treated with antiepileptic agents according to some indications. The meta-analysis of data obtained in randomized, placebo controlled clinical studies of antiepileptic agents also showed a slight increase in the risk of suicidal thoughts and behavior. The reasons for this risk are unknown, the available data does not allow excluding risk increased in connection with the use of valproat. Therefore, careful monitoring of signs of suicide thoughts and behavior in patients is necessary, appropriate treatment may be required. Patients (and people caring for them) should seek medical help if suicide thoughts and behavior take place. Interaction with other drugs, the simultaneous use of this drug with lamotridigin is not recommended. Precautions when using before starting treatment should be laboratory analysis of the liver function, then, during the first 6 months, repeatedly repeated, especially in patients with risk group. As in cases with most antiepileptic agents, one can observe an isolated, temporary and moderate increase in transaminases without any clinical symptoms, especially at the beginning of treatment. In such cases, it is recommended to conduct a more complete laboratory examination (in particular, the determination of prothrombin time) in order to revise the dosage if necessary; The tests are repeated depending on the results. For children under 3 years of age, the use of sodium valproate is recommended only as monotherapy after weighing therapeutic benefits/risk of pancreatitis and the development of pancreatitis in patients of this age group. In addition, not all dosage forms are applicable in children: see the section “Method of application and dose”. Before starting treatment, as well as before any surgical surgery and in cases of hematoma or spontaneous bleeding, it is recommended to do a blood test (a general blood test, including the number of platelets, bleeding time and blood coagulation indicators). Avoid the simultaneous appointment of salicylate derivatives for children due to possible hepatotoxicity and the risk of bleeding. With renal failure, an increase in the concentrations of valproic acid in the blood should be taken into account and, in connection with this, it is necessary to reduce the dose. Patients with a deficiency of enzymes of the urea cycle is not recommended for this drug. In such patients, several cases of hypermonyia are described, flowing with a stupor or coma. In children with an anamnesis of liver and gastrointestinal disorders of unclear etiology (anorexia, vomiting, cases of cytolysis) with episodes of lethargy or coma, delayed mental development or with cases of death of a newborn child or baby in a family history, before starting treatment with a valPatom, it is necessary Conduct an examination of metabolism, in particular, the presence of ammonium on an empty stomach and after eating. Despite the recognition that this drug causes disorders of the immune system only in exceptional cases, in patients with systemic red luster, the ratio of benefit and risk should be weighed. When starting treatment, the patient should be informed of a possible increase in weight and appropriate measures, mainly dietary, which he should be taken to minimize such an effect. Pregnancy should also be excluded in women of childbearing age and apply effective contraception before starting treatment. Pregnancy is not recommended for the intake of depakin chrono during pregnancy, as well as women of childbearing age, who do not use effective contraception. The risk of defects of development caused by Walproat is 3-4 times higher in pregnant women taking this drug than the risk found in the total population, which is 3%. Most often, the observed malformations are defects in the closing of the nervous tube (approximately 2-3%), face dysmorphia, crevice of the face, craniostenosis, heart defects, malformations of the kidneys and urinary tract and deformation of the limbs. Doses exceeding 1000 mg/day, and combining with other anticonvulsants are important risk factors for the formation of development of development in the fetus. Modern epidemiological data do not indicate a decrease in the general coefficient of mental development of children with the exposition of sodium in utero. However, such children describe some decrease in verbal abilities and /or more frequent appeal to speech therapy or for additional classes. In addition, several cases of autism and related violations are recorded in children who have undergone sodium in intrauterine valPriat. Additional studies are needed to confirm or refute these results. When planning pregnancy, if a pregnancy is planned, you should certainly solve the issue of the use of other therapeutic drugs. If the use of sodium valproate is inevitable (i.e. there is no other alternative), it is recommended to prescribe the minimum effective daily dose. The dosage forms of prolonged release should be used or - if this is impossible, distribute the daily dose into several tricks. This is necessary in order to avoid peaks of maximum concentrations of valproic acid in the blood plasma. Currently, there are no data confirming the effectiveness of additional intake of folic acid by women who are exposed to sodium valproata during pregnancy. However, given its favorable action in other conditions, you can offer additional taking folic acid at a dose of 5 mg/day 1 month before conception and within 2 months after it. An examination aimed at identifying malformations should be the same for everyone, regardless of whether a pregnant woman accepts folic acid or not. During pregnancy: if the choice of another drug is absolutely impossible, and you need to continue treatment with sodium valproat, it is recommended to prescribe a minimum effective dose. It should be avoided if possible doses exceeding 1000 mg/day. Regardless of the intake of folic acid, the examination for the presence of malformations in the fetus is necessary for all pregnant women. Before childbirth, a coagulogram should be made, in particular, the number of platelets, the level of fibrinogen and the time of blood coagulation (activated partial thromboplastin time, APTV). Newborn depicin chrono can cause the development of hemorrhagic syndrome in newborns not associated with vitamin K deficiency. Normal indicators of mother hemostasis do not exclude the possibility of pathology in a newborn. Therefore, in a newborn, the number of platelets, the level of fibrinogen and activated partial thromboplastin time (ACTS) should be determined. Newborns also recorded cases of hypoglycemia in the first week of life. lactation is released with breast milk in a small amount. However, in connection with the data on reduced verbal abilities in young children, patients should be advised to abandon breastfeeding. The peculiarity of the influence on the ability to drive a vehicle or potentially dangerous mechanisms of the patient should be warned of the danger of drowsiness, specially in the case of combined anticonvulsive therapy or combination of depicin chrono with drugs capable of increasing drowsiness. An overdose symptoms: a coma with muscle hypotension, hyporeflexia, myosa, violation of the respiratory function and metabolic acidosis. Rare cases of intracranial hypertension that occurs due to edema of the brain are described. Treatment: gastric lavage, maintaining effective diuresis, monitoring the condition of the cardiovascular and respiratory systems. In very severe cases, if necessary, extremenal dialysis can be performed. As a rule, the prognosis of such poisoning is favorable. Despite this, several cases of death have been recorded. The form of release and packaging of 30 tablets in a polypropylene container with a plastic traffic jam and a drainage. For 1 container, along with instructions for medical use in the state and Russian languages, they are invested in a cardboard pack. Storage conditions Store at a temperature not exceeding 25°C in a dry place. Keep out of the reach of children! The shelf life of 3 years is not used after the expiration date indicated on the packaging. Conditions for dispensing from pharmacies By prescription
Interactions of the drug Depakine
The simultaneous use of Depakine with drugs that can cause seizures or reduce the seizure threshold, depending on the possible risk, is not recommended or contraindicated. These drugs include most antidepressants (tricyclics, selective serotonin uptake inhibitors), antipsychotics (phenothiazines and butyrophenones), mefloquine, bupropion and tramadol. Contraindicated combinations Mefloquine - risk of epileptic seizures in patients with epilepsy with increased metabolism of valproic acid and the convulsant effect of mefloquine. St. John's wort is a risk of reducing the concentration of valproic acid in the blood plasma and the effectiveness of the drug. Combinations not recommended Lamotrigine - increased risk of severe skin reactions (toxic epidermal necrolysis syndrome). An increase in the concentration of lamotrigine in the blood plasma due to a slowdown in its metabolism in the liver under the influence of valproate. If such a combination is necessary, careful monitoring of the patient is required. Combinations that require special caution when using Carbamazepine - the concentration of the active metabolite of carbamazepine in the blood plasma increases, signs of its overdose appear. The concentration of valproic acid in the blood plasma decreases due to increased metabolism in the liver under the influence of carbamazepine. With simultaneous use, it is necessary to clinically monitor the patient, determine the concentration of valproic acid and carbamazepine in the blood plasma, and review the dosage of the drugs. Carbapenems, monobactams (meropenem, panipenem, aztreonam, imipenem) - the risk of seizures due to a decrease in the concentration of valproic acid in the blood serum. It is recommended to clinically monitor the patient, determine the concentration of drugs in the blood plasma and, possibly, review the dosage of Depakine during treatment with an antibacterial drug and after its discontinuation. Felbamate - increased concentration of valproic acid in blood serum and risk of overdose. Clinical and laboratory monitoring is necessary; it is possible to review the dosage of Depakine during treatment with felbamate and after its discontinuation. Phenobarbital, primidone - an increase in the concentration of phenobarbital or primidone in the blood plasma with the appearance of signs of overdose, especially in children; a decrease in the concentration of valproic acid in the blood plasma due to an increase in its metabolism in the liver under the influence of phenobarbital or primidone. Clinical monitoring of the patient is necessary during the first 15 days of combined treatment and immediate reduction of the dose of phenobarbital or primidone if signs of sedation appear; determination of drug levels in blood plasma. Phenytoin - there is a danger of reducing the concentration of valproic acid in the blood plasma due to increased metabolism in the liver under the influence of phenytoin. It is recommended to clinically monitor the patient's condition, determine the level of drugs in the blood plasma and, possibly, change their doses. Topiramate - there is a risk of hyperammonemia or encephalopathy under the influence of valproic acid taken in combination with topiramate. Strict clinical monitoring of the patient's condition is necessary to detect ammonemia during the first month of treatment and when symptoms appear that indicate its occurrence. Combinations that should be taken into account Nimodipine (oral and parenteral) - increased hypotensive effect of nimodipine due to an increase in its concentration in the blood plasma (weakening of metabolism by valproic acid). Other forms of interactions Oral contraceptives - valproate does not have an enzyme-reducing effect, and therefore does not reduce the effectiveness of gestoprogestogens in women taking hormonal contraceptives.
Contraindications
hypersensitivity to sodium valproate, valproic acid, semisodium valproate, valpromide or any of the components of the drug;
acute hepatitis;
chronic hepatitis;
a history of severe liver disease (especially drug-induced hepatitis) in the patient and/or his close blood relatives;
severe liver damage with a fatal outcome when using valproic acid in close blood relatives of the patient;
severe dysfunction of the liver or pancreas;
hepatic porphyria;
established mitochondrial diseases caused by mutations in the nuclear gene encoding the mitochondrial enzyme γ-polymerase (POLG), such as Alpers-Huttenlocher syndrome, and suspected diseases caused by defects in γ-polymerase in children under 2 years of age (see "Special Instructions" );
patients with established disorders of the carbamide cycle (urea cycle) (see “Special Instructions”);
hemorrhagic diathesis, thrombocytopenia;
combination with mefloquine;
combination with St. John's wort preparations;
children's age up to 6 months.
With caution: history of liver and pancreas diseases; pregnancy; congenital enzymopathies; inhibition of bone marrow hematopoiesis (leukopenia, thrombocytopenia, anemia); renal failure (dose adjustment required); hypoproteinemia (see “Pharmacokinetics”, “Dosage and Administration”); simultaneous use of several anticonvulsants (due to an increased risk of liver damage); simultaneous use of drugs that provoke seizures or lower the seizure threshold, such as tricyclic antidepressants, SSRIs, phenothiazine derivatives, butyrophenone derivatives, chloroquine, bupropion, tramadol (risk of provoking seizures); simultaneous use of antipsychotics, MAO inhibitors, antidepressants, benzodiazepines (possibility of potentiating their effects); simultaneous use of phenobarbital, primidone, phenytoin, lamotrigine, zidovudine, felbamate, acetylsalicylic acid, indirect anticoagulants, cimetidine, erythromycin, carbapenems, rifampicin, nimodipine, rufinamide (especially in children), protease inhibitors (lopinavir, ritonavir), cholestyramine (due to pharmacokinetic interactions at the level of metabolism or communication with plasma proteins may change the plasma concentrations of either these drugs and/or valproic acid, for more details see “Interaction”); simultaneous use of carbamazepine (risk of potentiation of the toxic effects of carbamazepine and a decrease in plasma concentrations of valproic acid); simultaneous use of topiramate or acetazolamide (risk of encephalopathy); existing deficiency of carnitine palmitoyltransferase (CPT) type II (higher risk of developing rhabdomyolysis when taking valproic acid).
Overdose of the drug Depakine, symptoms and treatment
Clinical manifestations of a significant overdose usually occur in the form of coma of varying severity with muscle hypotonia, hyporeflexia, miosis and respiratory depression. Possible intracranial hypertension due to cerebral edema. Emergency care in a hospital should include gastric lavage (effectively within 10–12 hours after taking the tablets), osmotic diuresis, and constant monitoring of the functions of the cardiovascular and respiratory systems. In severe cases, dialysis or exchange transfusion is indicated. There are reports of the successful use of naloxone as an antidote for acute drug poisoning. With a significant overdose, death is possible, but the prognosis is usually favorable.