Make an appointment by phone: +7 (343) 355-56-57
+7
- About the disease
- Cost of services
- Sign up
- About the disease
- Prices
- Sign up
A concussion is a form of traumatic brain injury. In which short-term memory loss may occur, brain dysfunction is reversible. Usually the cause is various traumatic situations. In case of injury, the protective fluid is not able to prevent the impact of brain tissue on the bone tissue of the skull. The injury requires hospitalization and consultation with a specialist.
Possible symptoms of a concussion
- Brief confusion or loss of consciousness. With a strong blow, the moment of injury disappears from memory.
- Dizziness even at rest, and when turning, bending or other changes in body position, the symptom intensifies.
- Severe headache, nausea and vomiting.
- Double vision, inability to concentrate on one point.
- Increased sensitivity to light and sounds.
- Impaired coordination of movements.
- Reaction inhibition - the victim gives an answer to the question after some time.
- Pale skin, weakness, sweating.
Important! A concussion is not always accompanied by visible head injuries, so the absence of wounds does not exclude brain injury.
Brain contusion (concussion) - symptoms and treatment
A patient with suspected traumatic brain injury should receive medical attention as soon as possible. Since it is impossible to reverse brain damage resulting from trauma, treatment measures should be aimed at stabilizing the patient's condition and preventing secondary damage.
Conservative treatment of brain contusions
In the setting of traumatic illness, decreased or increased intracranial pressure, decreased blood oxygen saturation, high temperature, and increased blood glucose levels can have a detrimental effect on the brain. In this regard, the main directions of therapy for people with severe bruises are identified [4]:
- breathing support (ventilators, oxygen mask);
- correction of blood circulation and infusion therapy (medication);
- treatment of intracranial hypertension;
- neuroprotection - protection of neurons from damage, carried out with medications.
Basic therapy. For victims with severe TBI, an open airway is created by removing saliva, blood and vomit. Sedatives and muscle relaxants are used as needed (designed to relax muscles, block nerve impulses and reduce pain.). Correction of elevated body temperature is necessary (using antipyretic drugs and/or physical conditioning methods) [4].
The development of convulsive syndrome in persons with a brain contusion is considered dangerous and requires immediate response. Seizures are always accompanied by rapid intracranial hypertension, an increase in the volume of intracranial hematomas, increased oxygen consumption in the brain, its blood supply and increased cerebral edema [13]. Prophylactic use of anticonvulsants (according to multicenter studies) in people with TBI reduces the likelihood of seizures in the acute period, but does not reduce the risk of their occurrence in the long-term period.
All persons with a cerebral contusion require prevention of thromboembolic complications (deep vein rhombosis of the lower extremities and pulmonary embolism), which involves the use of compression stockings, increased physical activity and anticoagulant therapy whenever possible. Mortality in thrombosis of the veins of the lower extremities reaches 9-50% [7].
It is also necessary to control blood glucose levels and prevent complications from the gastrointestinal tract (stress ulcers, gastrointestinal bleeding). The main reason for the development of stress ulcers is the release of catecholamine hormones during injury, which are produced in response to stress, insufficient blood supply to the upper gastrointestinal tract and disruption of its self-regulation.
Respiratory support. Indications for respiratory support [3][10]:
- depression of the level of wakefulness to stupor or coma;
- lack of own breathing;
- acutely developed breathing rhythm disturbances, pathological type of breathing (Cheyne-Stokes, Kussmaul);
- tachypnea (rapid shallow breathing) more than 30 respiratory movements per minute;
- clinical signs of hypoxemia (lack of oxygen in the blood) and/or hypercapnia (excess carbon dioxide): partial pressure of oxygen in arterial blood (PaO2) less than 60 mm Hg. Art.; hemoglobin saturation with arterial blood oxygen (SaO2) is less than 90%; partial pressure of carbon dioxide in arterial blood (PaCO2) more than 55 mm Hg. Art.;
- status epilepticus (epileptic seizures do not stop for more than 30 minutes);
- maxillofacial trauma combined with trauma to the facial skeleton, cranio-orbital region (near the orbit and adjacent areas) and/or chest.
The main task of respiratory support is to maintain normal carbon dioxide tension (PaCO2 - 30-35 mm Hg) and the necessary oxygenation of blood in the arterial bed (PaO2 more than 100 mm Hg) [6][7].
If the duration of mechanical ventilation is more than 48 hours after the start of breathing support, a tracheostomy should be performed (an operation to create an external opening in the wall of the trachea to establish breathing). When a brain contusion is combined with trauma to the facial skeleton and chest, it is preferable to perform a tracheostomy immediately upon admission of the victim to the hospital [10].
Correction of blood circulation and infusion therapy. More than half of patients with a decrease in wakefulness to stupor and coma are in a state of dehydration upon admission to the hospital. Causes include bleeding, insufficient fluid intake, overheating, vomiting and/or diabetes insipidus. Performing adequate infusion therapy (intravenous administration of medicinal solutions and drugs using a dropper) makes it possible to achieve a normal total blood volume, normalize cardiac output and the delivery of blood and oxygen to the brain.
The injured brain is extremely sensitive to low blood pressure (below 90 mm Hg), which a healthy brain tolerates normally. Therefore, the management of patients with severe TBI involves maintaining blood pressure (BP should be at least 90 mm Hg), which is necessary for adequate brain perfusion (providing it with oxygen and glucose) in conditions of edema [4][5][6] [7][9]. However, aggressive attempts to maintain blood pressure using vasopressors (vasoconstrictors) should be avoided due to the risk of respiratory distress syndrome (pulmonary edema with difficulty breathing) and cerebral edema [4][7].
Treatment of intracranial hypertension. To select adequate treatment tactics, it is necessary to distinguish between intracranial and extracranial causes of high ICP. The former include intracranial hematomas, bruises, edema and/or cerebral ischemia, epileptic seizures, and meningitis. The second is a lack of oxygen supply, inadequate sedation or ventilation, impaired venous outflow from the cranial cavity, increased intrathoracic and intra-abdominal pressure [1][3]. All these reasons can accompany brain contusion.
Sedation and analgesia are first-line interventions for the treatment of intracranial hypertension [4][7]. The head of the bed must be raised by 30-40° to improve venous outflow from the cranial cavity. To treat increased intracranial pressure and protect the brain from secondary damage, craniocerebral hypothermia (lowering brain temperature) is used. It is sufficient to carry out moderate hypothermia (T = 30-31 °C) [1][4]. The use of hyperbaric oxygenation (saturation of the patient with oxygen under high pressure) is pathogenetically justified in persons with brain contusion, since this method increases the oxygen tension in arterial blood and improves oxygen saturation of the brain.
To reduce intra-abdominal pressure, drugs are used that improve intestinal motility and normalize the function of the gastrointestinal tract [4][6]. If intracranial hypertension is not responsive to drug therapy, decompressive craniotomy is indicated.
Neuroprotection. Currently, the use of neuroprotective drugs is a promising direction in the treatment of brain contusions [9]. Based on their mechanism of action, neuroprotectors are divided into several types:
- Calcium channel blockers (Nimodipine, Breinal, Dilceren, Nimopin, Nimotop). They reduce the entry of calcium ions into the cell, reduce the level of damage and death of nerve cells under the influence of neurotransmitters and prevent apoptosis (programmed cell death).
- Antioxidants and antihypoxants (Actovegin, polyethylene glycol superoxide dismutase, Solcoseryl, Neurox, Mexidol, Armadin, Cytoflavin, Neurocard, Astrox, Meksifin, tocopherol, Methostabil, ascorbic acid, Ascovit, Nootropil, Piracetam, Noocetam, Melatonin, Cavinton, Vinpocetine, Cohen winter Q10). These drugs are nitrogen synthase antagonists, they prevent the formation of free radicals, restore the activity of antioxidant enzymes, accelerate glycolysis (the process of glucose oxidation), increase resistance to hypoxia and improve cerebral blood flow.
- NMDA receptor antagonists (Memantine, Memantal, Memorel, Noodzheron, Akatinol, Memikar, Mirvedol, Memaneurin). Reduce the damaging effects of glutamate.
- Blockers of the inflammatory and immune response (Cycloferon, COX-2 inhibitors, CD11 and CD18 antibodies). Reduce the severity of the inflammatory reaction.
- Stabilizers of cell membranes: intermediate products of phosphatidylcholine synthesis (Recognan, citicoline, Ceraxon, Proneuro, Quinelle, Neuropol, Neurocholin, Noocil, Ceresil Canon), magnesium and potassium preparations (magnesium sulfate, Aspangin, Pamaton, Asparkam, Panaspar, Panangin).
- Drugs that improve synaptic transmission (precursors for acetylcholine synthesis - Cereton, Cerepro, Gleatser, Holitylin, Delecit, Gliatilin).
- Apoptosis blockers (caspase-3 inhibitors, calpain inhibitors).
- Drugs with a neuron-specific neurotrophic effect (Cortexin, Cerebrolysate, Cerebrolysin).
- Immunosuppressants (cyclosporine A). Suppress the immune response.
Nutrition for severe brain contusion . With serious damage, patients, as a rule, cannot eat on their own, so early nutritional support (i.e., the introduction of nutrients into the body) is necessary. Such support should match the patient's protein and energy needs. Basic energy metabolism in patients with severe brain contusion corresponds to 20-25 kcal/kg per day [4][6].
Surgical treatment of brain contusions
Some patients with severe traumatic brain injury are transported to the operating room after a head CT scan. The purpose of surgery for severe brain contusion is to remove massive intracranial hematomas or correct elevated ICP.
Not all patients with TBI require emergency intervention. Since the size of a brain contusion and the volume of an intracranial hematoma may increase during the first hours/days after injury, dynamic monitoring is recommended. Treatment of such patients is carried out in an intensive care unit. If neurological disorders increase or intracranial pressure increases (if an ICP monitoring sensor was installed), a control CT scan is performed. If a significant increase in the volume of the hematoma or displacement of the brain is diagnosed, the safest option will be surgical intervention to prevent brain death.
Before surgery, the hair over the affected area of the brain is shaved. After cutting the scalp and removing the skin flap, the bone is cut out. The bone is removed and the underlying dura mater is opened with the utmost care. The doctor removes the hematoma or brain contusion. In the presence of severe cerebral edema, plastic surgery of the dura mater is performed using a patch from one’s own tissue or artificial replacement material. This is necessary to prevent further displacement of the brain. In such cases, the bone is not put back in its original place.
Before “closing” the wound, it is possible to install an ICP sensor if it has not been installed previously. Upon completion of the operation, the patient is transferred to the intensive care unit for intensive treatment measures aimed at combating cerebral edema and preventing infectious and thromboembolic complications.
Decompressive craniotomy is the most aggressive treatment for intracranial hypertension [3][9]. It is used when conservative therapy is ineffective. The main goal of decompressive trephination is to increase intracranial volume. As a result, the pressure in the cranial cavity is reduced and the blood supply to the brain is normalized.
Decompressive trepanation includes infratemporal and bifrontal decompression, temporal lobectomy and hemicraniectomy. They are carried out in cases of pronounced displacement of brain structures and persistent intracranial hypertension in patients with clinical and CT signs of brain compression.
Possible postoperative complications. In the long-term postoperative period of TBI, epilepsy is registered in 13% of patients, and post-traumatic hydrocephalus in 11% [3]. Post-traumatic epilepsy occurs due to the formation of a pathological focus in the brain. Post-traumatic hydrocephalus is caused by impaired circulation (formation of adhesions) and absorption of cerebrospinal fluid.
First aid for concussion
- If one or more symptoms are present, immediately call an ambulance or take the victim to a doctor.
- Treat a wound on the head if it appears as a result of an impact.
- For an hour or until the doctor arrives, it is important not to fall asleep, but to remain at rest.
- If you lose consciousness, lay the person on his side, bend his knees, and put his hands under his head.
- If symptoms of a concussion do not immediately appear, it is recommended to rest and not begin vigorous activity.
Classification of pathology
The disease occurs in three degrees of severity, which are divided into:
- Mild form - passes without short-term loss of consciousness. The patient experiences spatial disorientation, cephalalgia, dizziness, and nausea. Symptoms are recorded within 20 minutes after the injury and can be supplemented by an increase in temperature up to 38 degrees. Subsequently, the signs of pathology spontaneously disappear and the condition stabilizes.
- Moderate – the injury does not cause fainting and manifests itself with a standard clinical picture. Unlike a mild concussion, symptoms last more than 20 minutes, and the disease can provoke short-term memory loss. Retrograde amnesia is characterized by the absence of events that occurred a few minutes before the TBI.
- Severe – manifested by short-term fainting. Events are erased from memory under the influence of retrograde amnesia, clinical signs of a concussion persist for several weeks. The condition is accompanied by sleep and appetite disturbances, nausea, problems with orientation in space, cephalgia, and fatigue.
Recommendations for the treatment of concussions
If hospitalization is not required, with the permission of a doctor, a mild concussion can be treated at home:
- Bed rest and rest are required, no work. Long sleep is very important.
- You cannot read, watch TV, play computer games or use gadgets.
- Under no circumstances should you play sports.
- You are allowed to listen to music, but not through headphones.
- You can use herbal sedative drops or herbal infusions.
- In your diet, you should give preference to dairy and plant products, limit salt intake - to prevent increased pressure, including intracranial pressure.
If the patient seeks medical help in a timely manner and all recommendations are followed, recovery will occur quickly and without complications.
Diagnostic methods
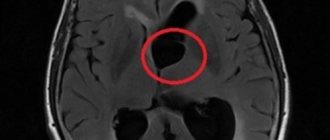
To determine the nature and extent of disorders, methods such as CT and MRI are used. During a diagnostic CT study, abnormalities are detected - areas of hemorrhage, damage to parenchyma (nervous tissue), fractures of the bone structures of the skull. Computed tomography is considered the most informative method for identifying indications for emergency surgery.
Other advantages of CT: the ability to examine patients in a state of psychomotor agitation, and quick results. Neuroimaging is mandatory for patients:
- Children under 16 years of age.
- Patients with signs of intoxication.
- Patients with a blurred, erased clinical picture.
- Patients taking anticoagulants on an ongoing basis (as part of a program for the treatment of chronic vascular pathologies).
With a mild concussion, changes in the structure of the brain matter are detected in 15% of cases. If, during the initial examination of the patient, neurological symptoms of a focal type are observed, morphological changes in the nervous tissue are detected with a frequency of 50% of cases.
An MRI study is more sensitive to detecting axonal damage of a diffuse type, changes in the structure of the parenchyma, and hematomas of subdural (under the dura mater) localization. MRI reveals hemorrhagic disorders that are associated with axonal damage.
Danger can lurk at every step
In adults, a concussion often occurs against the background of alcohol intoxication: either he lost his balance, or he actively got involved in a fight, or he got into an accident. Alcohol in such cases becomes a factor that aggravates the patient’s condition and complicates early diagnosis,
because it obscures the clinical signs of the underlying pathology. It is difficult to figure out: lethargy and other manifestations are a consequence of intoxication or indicate the development of symptoms of a concussion. True, there are other options when an adult, completely sober person receives a TBI in transport, on the road, or at work due to circumstances beyond his control.
Head bruises often plague children and teenagers in games due to carelessness (slamming a book or briefcase on the head, other fun) or overestimation of capabilities when spending leisure time, because you really want to show off your adult prowess by riding an “iron horse” or jumping on roofs and fences.
Meanwhile, I would like to remind you that a concussion can occur without a blow. Sharp braking of a vehicle or attempts to maintain balance in winter ice sometimes also result in a known diagnosis.
Everyone knows that there are frequent cases of TBI and injury to other parts of the body among those for whom “sport is their life.” Chess does not sharpen an athletic figure and does not add physical strength, but “a person strives for perfection”, so he searches for new types of sports exercises, borrowing them from his peers overseas. What this could lead to - further.
The signs of a concussion in a child who can already speak and knows his “I” are practically no different from those in adults. But recognizing the symptoms of a concussion in infants can be very difficult even for a healthcare worker,
unless he is a pediatric neurologist, therefore, if this pathology is suspected, it is better for parents not to try to take responsibility and make a diagnosis on their own. The baby should be immediately shown to a doctor who is able to distinguish the normal behavior of the baby from the behavior of a sick child.
Clinical picture
A concussion is characterized by short-term depression of consciousness and single vomiting. Primary symptoms after a mild traumatic brain injury - increased breathing, changes in pulse and blood pressure - usually disappear quickly. However, if the patient has a history of hypertension or hypertensive reactions, blood pressure may persistently increase. This is due to the stress factors that accompany the injury.
Body temperature with mild traumatic brain injury remains within normal limits. Vasomotor reactions are possible (pallor, then redness of the face). People who have suffered a concussion are characterized by vegetative phenomena: flushing of the face, anxiety, sleep disturbances, sweating. In some cases, pain occurs when moving the eyes.