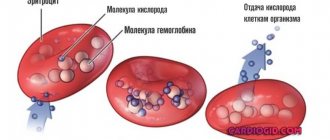
Monocytes are one of the types of white blood cells. Their functionality is of great importance for ensuring and maintaining the health of the human body.
They perform such important functions as antitumor, antiviral and others. However, often after taking blood tests you can hear from the doctor that the level of monocytes is increased. Unfortunately, few people know what this statement means and how to correct the situation.
And, most importantly, does such a phenomenon pose any danger in the body.
general information
Monocytes are cells belonging to the group of white blood cells. In healthy people, they make up about 3–8% of all white blood cells and are the largest blood cells found in the human bloodstream. Monocytes circulating in the blood have the ability to move from blood vessels to tissues, where they turn into macrophages, that is, phagocytic cells. Their main task is to fight bacteria and other microorganisms present in the body and produce substances that regulate the immune system.
A test that measures the number of monocytes in the blood is called a complete blood count with smear. If the result of this test shows an increased number of monocytes in your blood, you should consult your doctor as soon as possible, because such abnormalities can be caused not only by infections, but also by inflammatory, autoimmune or cancerous diseases.
blood test for monocytes in a child
Causes of monocytosis in children
If, after a thorough blood test, it turns out that the child’s monocytes are higher than normal, you need to sound the alarm. There are many reasons for this disorder.
The most common, as in cases with adults, is the onset of the development of an infectious disease. As a rule, this is not difficult to understand, since the baby begins to have a runny nose, cough, or some other manifestation.
However, cases in which monocytes increase, on the contrary, during the recovery period after suffering a serious illness are not uncommon. In such situations, this phenomenon is considered the norm and only indicates that the body is working.
Monocytes often increase after surgery. If none of the above applies to the baby, then most likely there are blood diseases.
ONLINE REGISTRATION at the DIANA clinic
You can make an appointment by calling the toll-free phone number 8-800-707-15-60 or filling out the contact form. In this case, we will contact you ourselves.
Monocytes - what are they and what are their functions?
Monocytes, also referred to as MONO in blood counting, are one type of non-granular leukocytes, that is, agranulocytes. Monocytes are produced in the bone marrow and are the largest of all white blood cells. Monocytes present in the blood have the ability to move from blood vessels to surrounding tissues and organs, where they transform into macrophages.
Monocytes are highly migratory and can reach very distant areas of the body. Their surface is covered with receptors to which substances produced by the immune system - chemokines - can bind. As a result, these cells are activated in areas where inflammation occurs and they can cross cell membranes and reach different areas of the body to fight pathogens. Monocytes also have the ability to produce substances that regulate the immune system, such as tumor necrosis factor (TNF), interferon, and interleukins. Moreover, they skillfully carry out the process of phagocytosis of pathogenic microorganisms and dead cells.
Monocytosis often occurs against the background of infectious diseases
Changes in blood monocyte levels are most often the result of infection or bone marrow disorders. Elevated monocytes can be the result of bacterial, viral or fungal diseases, as well as malignant hematopoietic diseases such as leukemia and lymphoma. In turn, a decrease in the number of these cells can be the result of HIV infection, which leads to the destruction of monocytes and a sharp decrease in the body's immunity.
Determination of the level of monocytes in an adult , which are part of a blood test, should be carried out prophylactically, preferably once a year. It is especially recommended when the patient develops frequent, recurring infections and problems with the immune system, or when hematological diseases are suspected.
If the result of a basic blood test shows a change in the level of monocytes, a manual blood smear should be added to it, that is, an assessment of the structure of white blood cells under a microscope. This will allow you to judge whether these cells are normal or not.
Biological role of monocytes
Monocytes are the largest phagocytes in our body. They perform the following functions in the body:
- Phagocytosis. Monocytes and macrophages have the ability to recognize and capture (absorb, phagocytose) foreign elements, including dangerous proteins, viruses, and bacteria.
- Participation in the formation of specific immunity and protection of the body from dangerous bacteria, viruses, fungi through the production of cytotoxins, interferon and other substances.
- Participation in the development of allergic reactions. Monocytes synthesize some elements of the complement system, due to which antigens (foreign proteins) are recognized.
- Antitumor protection (provided by the synthesis of tumor necrosis factor and other mechanisms).
- Participation in the regulation of hematopoiesis and blood clotting due to the production of certain substances.
Monocytes, along with neutrophils, belong to professional phagocytes, but have distinctive features:
- Only monocytes and their special form (macrophages) do not die immediately after absorbing a foreign agent, but continue to perform their immediate task. Losing a fight against dangerous substances is extremely rare.
- Monocytes live much longer than neutrophils.
- Monocytes are more effective against viruses, while neutrophils deal mainly with bacteria.
- Due to the fact that monocytes are not destroyed after a collision with foreign substances, pus does not form in places where they accumulate.
- Monocytes and macrophages are capable of accumulating in areas of chronic inflammation.
Preparing for analysis
Because the monocyte count is part of the blood test, the preparation for it is the same as for other basic laboratory tests.
The patient should present to the laboratory on an empty stomach with a minimum 12-hour break from eating. 2-3 days before the examination, it is worth limiting the amount of intense exercise and the use of stimulants. You must inform the referring physician about all medications and dietary supplements you are taking, as they may affect the results obtained.
How to determine
The level of monocytes is determined by a laboratory blood test to determine the percentage of vital cells. Capillary and venous blood is suitable for diagnosis.
Simultaneously with the level of phagocytes, the concentration of leukocytes is identified. A comparative analysis of qualitative blood parameters makes it possible to establish the severity of the infectious and inflammatory process that progresses in the female body.
Norm for children and adults
Reference ranges, which should include both the total number of monocytes in the blood and their percentage in the fraction of all leukocytes, are determined individually for each diagnostic laboratory. However, they most often fall into the following ranges:
- for children under 4 years of age: 0.05-1.1 thousand/µl (2-7% leukocytes),
- for children from 4 to 18 years: 0.1–0.8 thousand/µl (2–7%),
- for adults: 0.1–0.8 thousand/µl (1–8%).
Elevated monocytes in the blood of a child - what to do
When is the indicator normal?
So, you have a piece of paper in your hands with a summary of various parameters, including: leukocytes, erythrocytes, platelets, hemoglobin level and some others. We reach with our eyes the point “monocytes”. Normally, this figure in a healthy person ranges from 3 to 11%. If your level is higher, it means your body is fighting some kind of disease and you should visit your doctor for further testing. It should be noted that this parameter varies for different age groups and genders. And if in adult men and women the monocyte rate is approximately the same (3-10%), then for children there are some nuances. So, the optimal content of mononuclear phagocytes is:
- For newborns: 3-12%
- For babies up to two weeks: 5-15%
- From one month to a year: 4-10%
- Up to two years: 3-10%
- For children under 16 years old: 3-9%
Reasons for increased monocyte count
An elevated monocyte count in a child or adult can have various causes, and the interpretation of this result should always be made by a doctor, taking into account other blood parameters and blood smears.
The most common causes of an increase in the number of monocytes include:
- bacterial infections (for example, angina, tuberculosis, syphilis, Lyme disease, etc.),
- parasitic infections,
- viral (for example, mononucleosis) and protozoal infections,
- recovery from various types of infections,
- leukemia and lymphoma and other hematological diseases, such as multiple myeloma or myelodysplastic syndromes,
- cancer of the breast, ovaries, stomach and other organs, as well as tumor metastases,
- rheumatoid arthritis (RA), visceral systemic lupus and other collagen diseases,
- sarcoidosis,
- inflammatory bowel diseases and Crohn's disease,
- metabolic diseases,
- condition after removal of the spleen or other surgical procedures,
- alcoholic liver damage and other liver diseases,
- smoking,
- chronic stress,
- pregnancy,
- in infants - teething,
- taking certain medications, such as glucocorticosteroids.
Indications for the study
Monocytes (the norm for women by age, a table of clinical indicators is compiled based on the results of a diagnostic examination of the body) are large leukocytes that play a key role in the full functioning of the immune system.
Direct indications for testing the level of phagocytes are the presence of the following symptoms:
- frequent and unfounded intestinal disorders;
- increased body temperature without obvious signs of inflammation;
- tachycardia and disturbance of the rhythmic activity of the heart;
- dyspnea;
- dizziness and physical weakness;
- rapid fatigue after minor exertion;
- infectious and inflammatory skin diseases;
- chronic diseases of the nasopharynx, upper and lower respiratory tract;
- an allergic reaction that occurs in acute or chronic form.
The need for an analysis for the level of phagocytes in the blood serum is determined by the attending physician, who performs the initial examination of the patient.
What does a low monocyte count indicate?
A low monocyte count, also known as monocytopenia, may indicate HIV infection, immunodeficiency including Monomak syndrome, AIDS, bone marrow aplasia, leukemia or a consequence of chemotherapy or radiation therapy, severe stress, or certain medications.
If monocytopenia continues for a long time, it can lead to a decrease in all blood counts: red blood cells, leukocytes (white blood cells) and platelets. This condition is called pancytopenia.
Therefore, if there is any deviation from the norm in the monocyte test result, you should consult your doctor. If a history of infection is causing the change in monocyte count, the test should be repeated after 2 to 4 weeks.
In other cases, it may be necessary to complete the diagnosis with imaging tests, a urinalysis, and other blood tests such as CRP or ASO levels.
How and under what conditions is it produced?
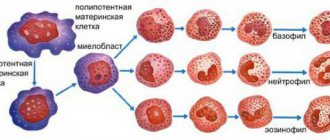
Previously, hematologists believed that phagocytes of this type are formed in the reticuloendothelial system. Recent scientific research has shown that monocyte synthesis occurs in bone marrow tissue.
Mature leukocytes, which have the most powerful phagocytic properties, are released into the bloodstream. The cells mature over the next 5 days, and then they become part of the peripheral blood.
The process of monocyte synthesis is inhibited during the period of taking drugs from the glucocorticoid group, as well as if a person is under constant stress for a long time. In this regard, immunity decreases, and the human body becomes more susceptible to infection by infectious, viral and fungal microorganisms.
Leukocyte formula (with mandatory microscopy of a blood smear) - counting the total number and different types of leukocytes, as well as studying their morphological features through microscopy of a peripheral blood smear.
Synonyms Russian
Leukoformula.
English synonyms
Leukocyte Differential Count, WBC Count Differential, Diff, Blood Differential, Differential Blood Count, White Blood Cell Differential.
Research method
Flow cytometry.
What biomaterial can be used for research?
Venous, capillary blood.
How to properly prepare for research?
- Eliminate alcohol from your diet for 24 hours before the test.
- Children under 1 year of age should not eat for 30-40 minutes before the test.
- Do not eat for 2-3 hours before the test; you can drink clean still water.
- Avoid physical and emotional stress for 30 minutes before the test.
- Do not smoke for 30 minutes before the test.
General information about the study
Leukocytes are a heterogeneous population of nucleated blood cells that are an essential part of the human immune system and play a role in inflammation, allergies and antitumor defense. There are five types of leukocytes, each of which performs its own specific functions: three types of granulocytes (eosinophils, basophils, neutrophils), monocytes and lymphocytes. The study of the leukocyte formula in a peripheral blood smear is a count of the number of different types of leukocytes and an assessment of their morphological properties. Both venous and capillary blood can be used for research.
Staining a blood smear with special dyes makes it possible to distinguish cells and intracellular structures; in addition, different types of leukocytes are not equally susceptible to certain dyes and are stained differently, which, together with differences in their morphological properties (shape of the nucleus, size and presence of intracellular granules), makes it possible to differentiate the main types of leukocytes when examining a smear using a microscope. Traditionally, the count is carried out per hundred cells and the resulting numbers are recorded as percentages. Knowing the total number of leukocytes, percentages can be converted into absolute values, which much more objectively reflect the state of the leukocyte population.
Granulocytes are so called because they contain granules in their cytoplasm, which contain biologically active substances necessary for leukocytes to perform their protective functions. There are three types of granulocytes:
- Mature neutrophils have a nucleus and granules segmented into 4-5 lobules, which turn purple when stained according to Romanovsky-Giemsa. Segmented neutrophils make up the bulk of peripheral blood leukocytes. In much smaller quantities in the blood, neutrophils of the previous stage of maturation can be found - band neutrophils (with a nucleus not yet divided into lobules). Cells of earlier stages of maturation (metamyelocytes, myelocytes and others) can appear in a blood smear in exceptional cases - for example, in severe infectious diseases, when the bone marrow throws out not yet mature cells to fight the infection (this is called a shift of the leukocyte formula to the left), and also in chronic myeloid leukemia.
- Eosinophils are involved in antiparasitic immunity and the development of allergic reactions. Their granules, which are orange-pink in color, contain mediators of allergy and inflammation. Eosinophils also differ from neutrophils in the structure of their nucleus - it is bilobed.
- Basophils are granulocytes that take an active part in immediate allergic reactions. They have an S-shaped non-segmented nucleus, which is often not visible due to large granules of intense blue color containing allergy mediators.
- Lymphocytes are cells with a large nucleus, practically devoid of cytoplasm. When stained according to Romanovsky-Giemsa, their nucleus is stained in an intense purple-violet color, and the cytoplasm is blue-blue. Lymphocytes participate in more complex immune reactions associated with the recognition of their own and foreign antigens and the production of antibodies. There are three classes of lymphocytes: T lymphocytes, B lymphocytes and NK cells (natural killer cells), but standard staining does not allow them to be distinguished; more technically complex methods are used for this (for example, immunophenotyping).
- Monocytes are relatively large leukocytes containing an unsegmented bean-shaped nucleus and, unlike lymphocytes, a large amount of cytoplasm. When stained according to Romanovsky-Giemsa, the nucleus acquires a purple-red color, and the cytoplasm becomes a cloudy bluish-gray. The main function of monocytes is phagocytosis, that is, the absorption and digestion of microorganisms, their own dying cells, etc.
The above types of leukocytes are found normally in a peripheral blood smear. In some diseases, cells that normally should not be in the smear may enter the blood from the bone marrow: for example, blasts are the morphological substrate of acute leukemia. In the conclusion to the study, the number and, if possible, morphological features of atypical cells must be indicated.
In addition to counting the number of cells, a laboratory diagnostic doctor, using microscopy of a blood smear, notes changes in the morphology of leukocytes:
- Toxogenic granularity of neutrophils - dark large coarse granules are present inside the cells, which are formed as a result of coagulation (“welding”) of the cytoplasmic protein under the influence of intoxication products.
- Vacuolization of the cytoplasm is also caused by severe intoxication, under the influence of which fatty degeneration occurs in the cell, and when the smear is fixed with alcohol, droplets of fat dissolve and the cells acquire a characteristic appearance.
- Knyazkova-Dele bodies are large pale blue areas of the cytoplasm of neutrophils, free from specific granules. Also found in inflammatory diseases, sepsis.
- Hypersegmentation of neutrophil nuclei - more than five segments in the nucleus of a segmented neutrophil. It may be a congenital feature (in which case it has no clinical significance), but a consequence of a deficiency of vitamin B12 or folic acid.
- Pelger's leukocyte anomaly is a congenital disorder of neutrophil maturation, manifested by a decrease in the segmentation of their nuclei. Mature neutrophils contain an unsegmented or two-segmented nucleus. This is not accompanied by a violation of the physiological properties of neutrophils.
- Botkin-Gumprecht shadows are dilapidated nuclei of leukocytes with remnants of nucleoli, obtained in the process of preparing a smear from tumor cells in chronic lymphocytic leukemia.
What is the research used for?
- To determine the number of individual types of leukocytes and their relationship with each other, assessing the morphological characteristics of leukocytes.
When is the study scheduled?
- If an infectious disease is suspected, as well as a pathology of bone marrow hematopoiesis.
- If the number of leukocytes deviates from the reference limits according to a blood test performed on a hematology analyzer.
What do the results mean?
Reference values
Leukocytes
| Age | Reference values |
| Less than 1 year | 6 - 17.5 *10^9/l |
| 1-2 years | 6 - 17 *10^9/l |
| 2-4 years | 5.5 - 15.5 *10^9/l |
| 4-6 years | 5 - 14.5 *10^9/l |
| 6-10 years | 4.5 - 13.5 *10^9/l |
| 10-16 years | 4.5 - 13 *10^9/l |
| More than 16 years | 4 - 10 *10^9/l |
Neutrophils
| Age | Reference values |
| Less than 1 year | 1.5 - 8.5 *10^9/l |
| 1-2 years | 1.5 - 8.5 *10^9/l |
| 2-4 years | 1.5 - 8.5 *10^9/l |
| 4-6 years | 1.5 - 8 *10^9/l |
| 6-8 years | 1.5 - 8 *10^9/l |
| 8-10 years | 1.8 - 8 *10^9/l |
| 10-16 years | 1.8 - 8 *10^9/l |
| More than 16 years | 1.8 - 7.7 *10^9/l |
Lymphocytes
| Age | Reference values |
| Up to 1 year | 2 - 11 *10^9/l |
| 1-2 years | 3 - 9.5 *10^9/l |
| 2-4 years | 2 - 8 *10^9/l |
| 4-6 years | 1.5 - 7 *10^9/l |
| 6-8 years | 1.5 - 6.8 *10^9/l |
| 8-10 years | 1.5 - 6.5 *10^9/l |
| 10-16 years | 1.2 - 5.2 *10^9/l |
| More than 16 years | 1 - 4.8 *10^9/l |
Monocytes
| Age | Reference values |
| Up to 1 year | 0.05 - 1.1 *10^9/l |
| 1-2 years | 0.05 - 0.6 *10^9/l |
| 2-4 years | 0.05 - 0.5 *10^9/l |
| 4-16 years | 0.05 - 0.4 *10^9/l |
| More than 16 years | 0.05 - 0.82 *10^9/l |
Eosinophils
| Age | Reference values |
| Up to 1 year | 0.05 - 4 *10^9/l |
| 1-6 years | 0.02 - 0.3 *10^9/l |
| 2-4 years | 0.02 - 0.5 *10^9/l |
Basophils: 0 - 0.8 *10^9/l.
Blood smear microscopy
Neutrophils - rods: 0 - 5%.
Neutrophils - segment.
| Age | Reference values |
| Up to 1 year | 16 — 45 % |
| 1-2 years | 28 — 48 % |
| 2-5 years | 32 — 55 % |
| 5-7 years | 38 — 58 % |
| 7-8 years | 41 — 60 % |
| 8-12 years | 43 — 60 % |
| 12-16 years old | 45 — 60 % |
| More than 16 years | 47 — 72 % |
Lymphocytes, %
| Age | Reference values |
| Up to 1 year | 45 — 75 % |
| 1-2 years | 37 — 60 % |
| 2-4 years | 33 — 55 % |
| 4-6 years | 33 — 50 % |
| 6-8 years | 30 — 50 % |
| 8-10 years | 30 — 46 % |
| 10-16 years | 40 — 45 % |
| More than 16 years | 19 — 37 % |
Monocytes, %
| Age | Reference values |
| Up to 1 year | 4 — 10 % |
| 1-2 years | 3 — 10 % |
| More than 2 years | 3 — 12 % |
Eosinophils, %
| Age | Reference values |
| Up to 1 year | 1 — 6 % |
| 1-2 years | 1 — 7 % |
| 2-4 years | 1 — 6 % |
| More than 4 years | 1 — 5 % |
Basophils,%: 0 - 1%.
An increased level of neutrophils can be observed during acute bacterial infections, intoxications and myeloproliferative diseases.
Neutropenia can be caused by severe infection, sepsis, toxic effects on the bone marrow (cytostatics, ionizing radiation, myelotoxic drugs), aplastic anemia, as well as congenital diseases (Kostmann's neutropenia, cyclic neutropenia).
The most common causes of eosinophilia are allergic diseases, parasitic infections, and myeloproliferative diseases.
An increase in basophils may indicate allergic reactions or myeloproliferative diseases.
Absolute lymphocytosis occurs in viral infections, including infectious mononucleosis and cytomegalovirus infection, chronic lymphocytic leukemia.
to a decrease in the number of lymphocytes .
Monocytosis is possible with infections, granulomatous diseases (tuberculosis, brucellosis, sarcoidosis), blood tumors, systemic connective tissue diseases.
Possible complications
Potential complications from too high or low monocyte levels depend on what disease is causing the change in blood cellular composition.
In general, the following consequences are possible:
- critical decrease in the protective functions of the immune system;
- tuberculosis of the lungs, bones, lymph nodes;
- development of various types of anemia;
- dysfunction of the bone marrow;
- death if the pathology is associated with the presence of malignant neoplasms.
The norm of monocytes in the body in women is determined by testing blood in a biochemical laboratory. Based on the results of the analysis, a detailed table of the concentration of vital cells is compiled, taking into account the patient’s age and concomitant diseases of the body.
Monocytes themselves are an integral part of the human immune system, perform a bactericidal function, prevent infectious and parasitic invasions, and take part in suppressing the inflammatory process.
Article design: Vladimir the Great