There are different types of cells in the blood. One of them are monocytes. These are large cells that literally absorb bacteria, damaged structures of their own body and destroy them. An increase in the level of monocytes is a normal reaction of the body during an infectious disease or inflammatory process. But often an excess of monocytes can also indicate pathology. To reliably establish the cause, it is necessary to carry out appropriate diagnostics.
What are monocytes in the blood
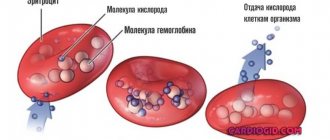
Monocytes are a type of leukocyte - white blood cells. These are large formations with large nuclei. They are involved in protecting the body from inflammatory processes. Monocytes can penetrate the walls of blood vessels, leaving the blood and rushing to the site of inflammation. They destroy bacteria, viruses, as well as dead cells of their own body. It turns out that monocytes perform an important sanitary function.
This is especially important during infectious diseases. For example, if a person is sick with the flu, at this moment many cells of the oropharynx and nasal cavity are destroyed. Then monocytes will arrive in large numbers to the appropriate areas and digest the dead parts of the cells. In this case, the tissues will recover faster, which will contribute to overall recovery.
The role of monocytes and eosinophils in the body
Among the five main types of white blood cells, these blood cells serve as the fighting soldiers of the immune system in the fight against foreign invasions: pathogenic bacteria, viruses, foreign proteins, any foreign bodies in the body. Mature monocytes and eosinophils are respectively called macro- and microphages, for their ability to capture, absorb, digest large and small foreign objects, called phagocytosis.
Both immune agents are produced by the bone marrow, circulate in the blood for some time, and then penetrate into the tissues, where they finally mature. Moreover, in eosinophils this process proceeds much faster, and mature bodies are able to react to any foreign invasion instantly. Macrophages mature for more than 100 hours, so their highest concentration is observed on the 3rd day of the disease.
Monocytes are the largest blood cells capable of neutralizing a large number of foreign objects. Like eosinophils, they move to the site of inflammation, where they fight foreign substances or altered cells.
Phagocytosis is the main weapon of macrophages; they not only take an active part in the body’s immune response, but are also involved in “cleaning up” after the battle: they neutralize damaged, dead blood cells, cell membranes, fragments of damaged tissue, and bacteria. Therefore, an increased concentration of monocytes is observed long enough after the acute phase of the disease, until all negative consequences for the body are completely neutralized.
Unlike monocytes, phagocytosis for eosinophils is not the main function. A distinctive feature of eosinophils is the ability to quickly respond to the presence of parasites or allergens. Mature forms are concentrated in integumentary tissues that are in direct contact with external irritants: skin, mucous membranes of the stomach, intestines, respiratory tract, and genitourinary system. This ensures a quick response to any pathogen. Blood contains them an order of magnitude less.
Cytotoxins secreted by eosinophils neutralize parasites and their larvae that have entered the bloodstream or are located in the mucous membranes. By releasing histamine and other inflammatory mediators, eosinophils themselves can provoke an immediate reactive immune response to the allergen and even anaphylactic shock.
The balance of monocytes, eosinophils and basophils in combination with the indicators of lymphocytes and neutrophils (leukocyte formula), which does not exceed normal limits, indicates the full function of the human immune system. An increase in the absolute or percentage number of certain types of leukocytes may indicate pathology of hematopoiesis, or disease of other systems and organs.
What does it mean if monocytes are elevated?
In a normal state, the number of monocytes in the blood is as follows (per 1 liter of blood):
- for adults: from 0.04 to 0.08*109 cell units;
- for children: from 0.05 to 1.1 * 109 cell units.
If we talk about the norm in relative terms, then the number of monocytes should be 1% -10% of the total mass of leukocytes. Moreover, for children the optimal range is from 2% to 7%, and for adults – from 1% to 8%. If the concentration is greater than the specified values, this indicates increased monocytes in the blood. This disorder is called monocytosis.
Why are eosinophils and monocytes needed?
Let's talk a little about eosinophils and monocytes. They, of course, perform different functions, and when their numbers are increased, it is necessary to find out which subpopulation is increased the most. And the most important thing is whether this increase is related to each other, or whether the patient is experiencing two independent pathological processes. The doctor, when he interprets the analysis, must understand that any changes in the leukocyte formula do not clearly indicate any disease, that is, they do not have specificity.
They can be caused by a variety of diseases, and the blood can react with different populations of cells in the same way. On the other hand, with the same disease in different patients, the blood can react in different ways.
It should not be forgotten that the assessment of a subpopulation of leukocytes has certain characteristics. The age of the patient must be taken into account. It is very important to remember that any deviation can be absolute or relative. With an absolute deviation, the number of monocytes and eosinophils increases, since more of them are simply actually produced. If this deviation is relative, then in reality there are exactly the same number of them, but in a given blood sample there are more of them, since there are fewer of them elsewhere. Therefore, in order to get a complete picture of the real number of leukocyte subpopulations, it is necessary to know not only their number per liter, but also as a percentage.
Monocytes
Monocytes in a typical blood smear always look like large cells, their nucleus resembles a bean or legume, without any constrictions and without segments. Monocytes do not live long in the blood, no more than a day, and then the pool of released monocytes rushes into the tissue. It enters the tissue through the endothelium, or the inner wall of capillary vessels, through active movement. In the tissue, the monocyte turns into special cells - macrophages, and are forever lost from the systemic circulation. They live in tissues for a very long time, up to several years, which is several times longer than the lifespan of any blood cells in blood vessels.
Tissue macrophages are active defenders, and in tissues they do the same thing as neutrophils in blood plasma. They recognize, capture and destroy all foreign microorganisms, including fungi; tissue macrophages have a high degree of phagocytosis. They actively appear in foci of tissue inflammation, where they also destroy all microbes, damaged cells, as well as their dead brothers - leukocytes. Macrophages are the most active cells capable of phagocytosis in our body, and their task in the area of inflammation is complete cleansing, elimination of the pathogen, destruction of tissue detritus and pus and preparation of the area for restoration or tissue regeneration. However, monocytes can not only be beneficial, but sometimes they also support pathological, autoimmune inflammation, such as in rheumatoid arthritis.
Therefore, the number of monocytes in the blood is the tip of the iceberg, a huge part of them is in the tissues, and therefore it is, of course, impossible to judge the state of macrophages by the monocytes that are in the bloodstream.
Read more about monocytes in our article Monocytes in the blood: functions, normal, causes of abnormalities.
Eosinophils
Eosinophils are cells of which there are very few in the blood, fewer of them, perhaps, only basophils. Yes, eosinophils are also capable of phagocytosis, but still their role is different. They are particularly good at recognizing parasitic antigens and engaging in various allergic cellular reactions.
Not a single neutrophil can compare with eosinophils in their ability to recognize and bind antigens of multicellular parasites. These primarily include various flatworms, roundworms and tapeworms. These are pinworms and roundworms, the cat fluke - the causative agent of opisthorchiasis and the liver fluke, the causative agents of diphyllobothriasis and taeniasis, that is, the broad tapeworm, and the pork tapeworm. These cells also remain in the blood for a very short period of time, literally a few hours, and then are transported to the tissues in order to restore order there, just like monocytes.
For more complete information, read the articles - Eosinophils: age norm and causes of deviations and Eosinophilia in adults.
The main reasons for the increase in monocytes in the blood
The main causes of monocytosis include:
- Infectious processes of bacterial origin, including syphilis, brucellosis, tuberculosis, endocarditis.
- Viral infections – hepatitis, mononucleosis.
- Diseases of the hematopoietic organs - leukemia.
- Malignant tumors.
- Rheumatism.
- Systemic lupus erythematosus.
- Recovery from infectious diseases.
- Previous surgical interventions.
- Entry of non-infectious substances (mainly through the lungs).
Important!
An increased level of monocytes does not always indicate a disorder. In some cases, this is a normal physiological state, for example, after eating, at the end of the menstrual cycle, and also in children under 7 years of age.
Monocytosis in children
An increase in monocytes in childhood is also often associated with infectious pathologies, mainly of a viral nature. If monocytosis is diagnosed based on a blood test, this means that the body is actively fighting disease-causing processes.
Also, a similar condition is observed with helminthic lesions - enterobiasis, ascariasis and others. After the destruction of helminths, the content of monocytes returns to normal. The cause may also be associated with tuberculosis, but such pathologies are rare. Monocytosis can be observed due to oncological processes. The most common are leukemia and lymphogranulomatosis.
Other common reasons:
- poisoning;
- allergic reactions;
- inflammation in the gastrointestinal tract;
- autoimmune pathologies;
- rheumatoid type arthritis;
- Crohn's disease;
- infections due to surgical interventions.
Deviations from reference values
Let us name those conditions in which the population of monocytes in the blood plasma significantly increases. These are all acute and chronic inflammatory diseases. These are furunculosis, streptoderma, arthritis, purulent inflammation of the subcutaneous tissue and phlegmon.
Since monocytes are tissue protectors, they surround various specific granulomas, which are infectious and inflammatory in nature. The most well-known specific granulomatous inflammation is tuberculosis infection and syphilis. Therefore, monocytes can be elevated in the blood for a long time in these diseases, as well as in the subacute course of bacterial endocarditis.
They can be increased in various forms of sarcoidosis, which also occurs as a type of granulomatous inflammatory process. It is interesting that sarcoidosis is a non-contagious disease, and granulomas, although inflammatory, are non-infectious in nature, but tissue macrophages are actively involved in its formation.
This is an autoimmune pathology, which is also inflammatory in nature, it is a state of convalescence after an acute infectious pathology, for example, after typhoid fever or dysentery. These are various malignant neoplasms and growing tumor tissues. Of the malignant neoplasms, the growth of monocytes is most typical for cancer of the stomach, mammary glands, and ovaries, as well as lymph nodes.
The cause of high monocytes can be oncohematological diseases, when the hematopoietic germ in the red bone marrow that produces granulocytes is affected. Finally, there is acute poisoning with organophosphates and tetrachloroethane.
Eosinophils, in addition to various allergic diseases and parasites, also increase upon the administration of many medications. They react with an increase in allopurinol, beta-blockers, heparin and many antibiotics.
There is a sharp increase in the number of eosinophils in various skin diseases. Their growth increases with eczema, atopic dermatitis, systemic pathology, for example, autoimmune diseases. Their growth also increases with malignant neoplasms in tissues and with damage to the red bone marrow. Rare causes include volatile eosinophilic infiltrates, or Loeffler's disease. The number of eosinophils increases in the initial period of various acute infections: scarlet fever, gonorrhea, tuberculosis and infectious mononucleosis.
What are the common reasons for both monocytes and eosinophils to increase at the same time? This:
- autoimmune pathology, or systemic connective tissue diseases;
- malignant neoplasm of lymph nodes;
- sarcoidosis;
- the oncohematological process and myeloblastic leukemia also lead to a joint increase in these populations.
Therefore, if a patient’s blood has repeatedly and consistently elevated monocytes and eosinophils, then it is necessary to be extremely wary of the risk of tuberculosis and sarcoidosis, be examined by an oncologist, and also pass all the necessary tests for autoimmune pathology, and consult a rheumatologist.
These steps will be correct, and depending on the clinical symptoms, epidemiological history, and data from instrumental and laboratory studies, the specialist can certainly make the correct diagnosis.
Symptoms of monocytosis
An increased content of monocytes can be reliably determined only by the results of a blood test. In this case, the disorder manifests itself with certain symptoms:
- apathy, decreased or lack of appetite;
- weight loss for no specific reason;
- high fatigue, general weakness of the body without an objective reason;
- depression;
- high level of anxiety, even panic states;
- emotional overexcitation for no specific reason;
- aversion to meat, aversion to it (occurs suddenly);
- bloating;
- constipation;
- diarrhea;
- discharge of large volumes of mucus with feces;
- dry cough that lasts for a long time (sometimes with blood discharge);
- muscle pain in the back area;
- pain in the legs;
- skin rash;
- rash in the genital area.