Main causes and their symptoms
Table 1. The most common causes of abdominal pain in a child.
| Causes | Symptoms |
| Colic | The appearance of colic is most typical for patients aged 3-4 months. They are accompanied by a deterioration in the child’s well-being with pronounced anxiety, crying, bending of the legs, tension and constant changes in body position. After taking up a vertical position, covering the abdomen with a warm diaper or drinking dill water, the severity of symptoms decreases and the child calms down. |
| Flatulence | The development of flatulence is accompanied by anxiety in the child. Despite an initially good appetite, he may abruptly refuse food. Lies mostly with knees bent. Frequent regurgitation, seething in the abdomen and painful release of gases, followed by relief of well-being, also appear. |
| Dysentery | The appearance of dysentery is characterized by a pronounced deterioration in health. An increase in body temperature is accompanied by increasing intoxication, weakness, and even loss of consciousness. Intestinal symptoms are expressed by single vomiting and frequent frequent stools, which are initially green in color with mucus or streaks of blood. After 2-3 illnesses, stool becomes extremely scanty. There may only be rumbling and tenesmus. |
| Viral infection | Children over five years of age are most often exposed to the development of viral infection. The disease is characterized by the appearance of symptoms of intoxication with dehydration, weakness, lethargy and loss of appetite. The temperature rises slightly. Dyspeptic symptoms are characterized by frequent bowel movements and vomiting, which do not bring relief. The stool is profuse with undigested pieces of food and an unpleasant odor. The patient may also be bothered by constant rumbling in the abdomen, flatulence and the appearance of cracks in the anus. The most dangerous signs of dehydration are those that develop within a short period of time. |
| Constipation and diarrhea | The development of constipation is manifested by the appearance of heaviness in the lower abdomen and an aching pain syndrome. The last bowel movement is noted several days ago. Symptoms of intoxication have not yet developed. Diarrhea is manifested by frequent bowel movements, which do not always bring relief. In this case, rumbling in the abdomen and spasmodic pain may develop. Due to frequent bowel movements, irritation develops in the rectal area. |
| Lactose intolerance | The disease is characterized by the appearance of pain half an hour after eating. They are spasmodic in nature, accompanied by flatulence, colic, severe bloating and regurgitation. |
| Gastritis stomach ulcers | Pathologies are manifested by initially aching pain, which can change to acute pain in the upper abdomen. In addition, nausea, vomiting, loss of appetite and weakness occur. |
| Parasites | The most common cause of abdominal pain in a child is roundworms. Symptoms may resemble colic, but are much less severe. However, they are regular. Headaches, flatulence and itching in the anus may occur, occurring mainly in the evening or at night. |
| Dyspepsia | Symptoms of dyspepsia develop one or two hours after eating and are accompanied by abdominal pain, flatulence, increased frequency of stools with an unpleasant odor, undigested food particles, and mucus. In addition, loss of appetite, frequent regurgitation and vomiting are possible. |
| Appendicitis | The disease is accompanied by the appearance of aching pain in the right iliac region or lower abdomen with an increase in temperature and an increase in intoxication. In the initial stages, one-time vomiting is possible. As the disease progresses, the pain becomes more intense and acute. |
| Pancreatitis | The development of pancreatitis is most typical for children aged 13-15 years. The patient is concerned about pain in the upper abdomen of a girdle and aching nature. Body temperature rises slightly. Vomiting and nausea occur, which intensify after eating, as well as dyspeptic symptoms caused by impaired enzyme production. |
| Intestinal obstruction | Obstruction is characterized by the appearance of diffuse pain in various parts of the abdomen, mainly in the umbilical region. Vomiting, passing gas or stool may occur once. As the disease progresses, bloating and intoxication with absence of bowel movements increases. |
| Intussusception | Intussusception is accompanied by the appearance of sharp paroxysmal pain in the abdomen, which intensifies after 10-15 minutes. The child behaves restlessly, screams, bends his legs to his stomach and breaks out in a cold sweat. Against the background of intestinal obstruction, vomiting, regurgitation and single passage of feces may occur. |
| Menstrual pain in girls | The development of menstrual pain is most often a concern in the first days of bleeding. There may be discomfort or pain that is aching in nature, radiating to the sacrum or coccyx. In addition, you may experience dizziness, weakness, decreased blood pressure, and cold, sticky sweat. |
| Crick | Sharp, paroxysmal pain that intensifies when walking may be associated with stretching of the muscles of the anterior abdominal wall. It may occur after physical strain, coughing or vomiting. The patient has a good appetite, no vomiting and no bowel movements. |
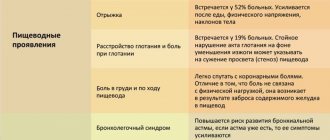
Symptoms of GERD:
regurgitation of gastric contents without previous nausea and any effort;
nausea followed by vomiting caused by contraction of the abdominal muscles and the patient’s effort;
chest pain, heartburn, crying, irritability and sleep disturbances;
episodes of aspiration and respiratory manifestations: chronic night cough, recurrent pneumonia, bronchial hyperreactivity of non-allergic origin;
bleeding from the upper gastrointestinal tract;
chronic esophagitis, esophageal ulcer, Barrett's esophagus, Sandifer's syndrome, including hiatal hernia, reflux esophagitis, torticollis, voluntary "squirming" movements of the head and neck, anemia;
refusal to eat;
erosion of tooth enamel;
increased dystonia and spasticity;
growth stagnation, anemia, hypoproteinemia associated with eating disorders or refusal to eat [17].
Respiratory symptoms, which are common in children with cerebral palsy, can also exacerbate the symptoms of GERD. Despite the high prevalence of GERD among children with cerebral palsy, the symptoms of the disease are not very specific, and children in this group cannot always express their complaints. Therefore, GERD in children with cerebral palsy is often diagnosed already at the stage of erosive esophagitis or esophageal ulcers or in the case of recurrent aspiration pneumonia. Aspiration pneumonia and refusal to eat, often found in GERD, can be a serious obstacle to effective nutritional support for children with cerebral palsy and are unfavorable prognostic factors. Therefore, GERD is another “red flag” when assessing the health status of children with cerebral palsy [2].
Diagnosis of GERD is based on a combination of clinical manifestations and data from instrumental methods. It is necessary to note the extreme importance of the clinical diagnosis of GERD in patients with cerebral palsy due to the high prevalence of this pathology, as well as due to the difficulties of organizing and conducting endoscopic examination and pH impedance measurements. The physician must evaluate the benefit/risk ratio of the examination and the need for concomitant sedation of the patient during the examination. Given the high prevalence of GERD and the vulnerability of this group of patients, in the presence of an appropriate clinical picture, a trial of treatment with proton pump inhibitors without endoscopic confirmation of reflux esophagitis is considered acceptable, subject to careful monitoring [25]. Nevertheless, esophagogastroduodenoscopy is the method of choice for diagnosing the depth and localization of damage to the esophageal mucosa. Biopsy is important to confirm or exclude other non-reflux causes of esophagitis, as well as in cases of suspected Barrett's transformation. Gastroesophageal scintigraphy is performed to confirm pulmonary microaspiration [2].
According to a study by G. Caltepe et al., alkaline reflux was more often diagnosed in children with cerebral palsy based on the results of intraesophageal pH impedance measurements [19]. The advantage of pH impedansometry is the ability to diagnose both acidic, weakly acidic and alkaline reflux, which allows you to choose the right tactics for patient management [20].
In children with persistent gastrostasis, to exclude intestinal obstruction, it is necessary to conduct an X-ray contrast examination of the esophagus and stomach with barium and/or ultrasound of the abdominal organs. In addition, patients with cerebral palsy and severe neurological deficits are at risk for developing superior mesenteric artery syndrome, since the combination of scoliosis and malnutrition leads to a decrease in the fat layer in the retroperitoneal area around the third - horizontal - part of the duodenum, which normally protects against compression the superior mesenteric artery in the area of the aorto-mesenteric angle [21].
Treatment of GERD in children with cerebral palsy includes lifestyle changes, diet therapy, medication and surgical treatment.
The effect of nutritional intervention on GERD in children with cerebral palsy has been studied in several studies. Thus, R. Miyazawa et al. noted the positive effect of the use of a food thickener, pectin, on the severity of GERD symptoms in 18 children with cerebral palsy [22]. V. Khoshoo et al. Children with cerebral palsy who were fed exclusively through a gastrostomy tube were divided into 2 groups. 1st was fed a casein-dominant formula and 2nd was fed a whey protein-based formula. A significant reduction in the number of episodes and duration of reflux was recorded in a group of children receiving a whey protein-based formula, which may be due to faster gastric emptying [23].
Antisecretory drugs are considered first-line therapy in children with cerebral palsy with signs of GERD. It is known that PPIs are superior in effectiveness to H2-histamine receptor blockers both in the treatment of erosive esophagitis and in reducing the symptoms of GERD [20]. However, PPIs do not affect the volume or number of reflux episodes, so symptoms such as nausea persist despite therapy. As with all cases where long-term use of PPIs is contemplated, special attention should be paid to side effects such as pulmonary and gastrointestinal infections and micronutrient malabsorption.
The effectiveness and safety of the use of prokinetics, in particular metoclopramide, domperidone and erythromycin, in the treatment of GERD in children with cerebral palsy have not been studied. Therefore, routine administration of drugs from this group to children with cerebral palsy is not recommended.
Monitoring the effectiveness of GERD therapy in patients with cerebral palsy is carried out using instrumental diagnostic methods (mainly EGDS). When there is a need for long-term PPI therapy, the “gold standard” for monitoring the effectiveness of treatment is intraesophageal pH impedance measurements, with or without esophageal pH measurements.
Indications for surgical treatment of GERD in children with cerebral palsy are: a) repeated episodes of apnea, bradycardia, recurrent pneumonia; b) Barrett's esophagus; c) the need for gastrostomy in combination with indications a) and b).
The high prevalence of dysphagia (severe, with the inability to eat by mouth, due to stenosis or stricture of the esophagus) and GERD in children with cerebral palsy often leads to complications, namely, impaired nutritional status, weight deficiency with micronutrient deficiency, an increased incidence of aspiration pneumonia and high mortality in this group of patients [17, 18]. The nutritional status and adequate nutrition of the child play an important pathogenetic role. If it is impossible to meet the child’s basic needs for energy and nutrients naturally, and if therapy aimed at correcting dysphagia and GERD is ineffective, there is a need to switch to enteral nutrition.
There have been no prospective randomized studies comparing the effectiveness and safety of feeding children with cerebral palsy through a nasogastric tube and gastrostomy tube. A Cochrane review comparing the effectiveness of gastrostomy feeding tubes and gastrostomy tube feedings in adult patients found benefits of gastrostomy tube feedings, namely a lower incidence of complications, less discomfort with feeding and increased social activity. There were no significant differences in mortality rates associated with aspiration and aspiration pneumonia. Thus, the placement of a gastrostomy tube is more effective and safer than the use of a nasogastric tube [24]. A prospective cohort study, including a 12-month follow-up of 57 children with neurological disorders, including cerebral palsy, fed through a gastrostomy tube, showed a significant improvement in weight curves, health status and quality of life, and a significant reduction in the time of one feeding. In addition, feeding through a gastrostomy tube did not lead to an increase in the frequency of episodes of respiratory infections.
Stomach ache - first aid
If you experience abdominal pain associated with poisoning, ensure you drink plenty of fluids. To do this, use only clean drinking water, as well as liquids that prevent the development of dehydration.
In order to remove toxins, it is allowed to use enterosorbents, for example, activated carbon. They will reduce the severity of diarrhea and also help remove the source of infection and toxins.
If the cause is unclear, as well as the persistence of symptoms with deterioration of well-being, you should not self-medicate. In the near future, you need to call an ambulance or go to a medical facility yourself.
Recommended video:
First aid before the doctor arrives
The main activities that should be carried out by others or parents before the ambulance arrives include:
- Avoid taking medications, in particular those with an analgesic effect. This will make it difficult to make a diagnosis in the future.
- Constant monitoring of body temperature. When the temperature rises to 38 degrees, measurements must be taken every 15-20 minutes and the resulting values recorded.
- Provide plenty of fluids. If vomiting, loose stools and abdominal pain occur, it is allowed to take pure still water, as well as solutions that can replenish the loss of fluid from the bloodstream, preventing dehydration. It is forbidden to give your child juices, lemonades, coffee or tea.
- Providing peace. The child must be put to bed so that he can take a position that is comfortable for him and relieves pain. Avoid eating.
Prevention of abdominal pain in children
Preventive measures aimed at reducing the severity of pain in children include:
- Normalization of nutrition. Restoring the diet, as well as selecting the optimal diet, helps prevent the development of abdominal pain, which can be functional in nature. To do this, you need to adhere to a regular diet with maximum limitation of snacks, as well as the consumption of salty, smoked, spicy and fried foods. Preference should be given to fermented milk products, fruits, vegetables, meat and poultry, as well as various cereals. It is important to avoid long breaks between meals.
- Creating a favorable psycho-emotional environment at home. Parents need to provide a psychologically comfortable environment for the child’s life, protecting him from quarrels, scandals, showdowns, as well as other adverse factors.
- Regulation of sleep and rest patterns. To prevent the development of pain, prevent a decrease in immunity, it is necessary to restore full sleep, eliminate excessive stress, and also normalize the work and rest regime.
- Compliance with personal hygiene rules. A prerequisite for reducing the incidence of abdominal pain is hand washing. This procedure is mandatory before eating, after coming from outside, visiting the toilet, and after contact with animals.
- Timely treatment of diseases occurring in acute or chronic form. This will prevent a decrease in immunity.
Functional pain—how to help your child?
The development of functional pain is common in children aged 7 to 15 years. This condition is accompanied by a pronounced deterioration in well-being, but even with a thorough diagnosis and a complete examination of the patient, the cause cannot be determined. Their appearance is not associated with the presence of pathology of a surgical or infectious nature.
Suspected causes that may cause functional pain include:
- Overwork.
- Exposure to severe stress or nervous tension.
- Functional dyspepsia or impaired stomach function, accompanied by painful digestion.
- Irritable bowel syndrome, which is associated with disruption of the digestive tract without organic pathology.
- Abdominal migraine. The appearance of pain is accompanied by a sharp deterioration in health with the development of nausea, vomiting and pallor of the skin.
Recommended video:
Despite the fact that functional pain does not pose a threat to the life and health of the patient, it can significantly impair the quality of life. Therefore, to alleviate the child’s condition, it is necessary:
- Create a calm atmosphere and provide care from loved ones to reduce the severity of stress. Eliminating negative reactions will help the nervous system recover, relieving tension.
- Dieting. Daily consumption of cereal products, fresh vegetables and fruits, as well as dried fruits, while simultaneously eliminating fast food, spicy, smoked and salty foods, alleviates symptoms and also normalizes the functioning of the digestive tract.
- Choose the right medications. If the functional nature of the pain is confirmed, there is no need to endure the pain syndrome. The child is allowed to take antispasmodics or mild non-steroidal anti-inflammatory drugs.
- Keeping a disease diary. It is important for the child to record the observations that he notes during the development of pain. This will help eliminate the cause of the disorders by comparing medical history data, reactions to medications, as well as the conditions under which the pain subsides.
Constipation
Constipation is a serious comorbid condition in children with cerebral palsy. The pathogenesis of constipation in children with cerebral palsy is complex and includes both functional and organic components.
R. Veugelers et al. conducted a study of constipation in 152 children with neurological disorders and formulated the following definition of constipation: the presence of hard, stone-like stools in more than 25% of bowel movements, frequency of bowel movements less than 3 times per week, stool palpated through the anterior abdominal wall, regular use of laxatives or passing stool only after a cleansing enema. This definition is based on the Rome III Revision Criteria and the diagnostic criteria for functional constipation in adults with disabilities [25].
Currently, the Rome IV revision criteria are used to diagnose functional constipation in children [26].
Can I give painkillers?
Taking painkillers for abdominal pain in a child of unknown etiology is prohibited by specialists. These drugs reduce the severity of pain, thereby distorting the clinical picture of the disease.
In the future, upon admission to the hospital, it will be more difficult to make a diagnosis and select the necessary diagnostic and treatment tactics. Therefore, if abdominal pain occurs, it is necessary to urgently contact a medical institution without self-medicating.
Despite the fact that the causes of abdominal pain in children can be varied, self-treatment is not allowed. This is associated with a high risk of complications and threat to the patient’s life.
Introduction
Cerebral palsy (CP) is a group of stable disorders of motor development and postural maintenance leading to motor defects caused by non-progressive damage and/or anomaly of the developing brain in the fetus or newborn child [1].
Motor disorders in cerebral palsy are often combined with sensory disorders, decreased cognitive function, speech and behavioral disorders, epilepsy and neuro-orthopedic complications. In addition, frequent companions of cerebral palsy are gastroenterological problems, which can be divided into difficulties associated with nutrition and the pathology of the gastrointestinal tract (GIT). Nutritional disorders in children with cerebral palsy include: varying degrees of weight deficiency, growth impairment, micronutrient deficiency, osteopenia and obesity [2]. Among the gastroenterological manifestations, the most common are dysphagia, gastroesophageal reflux disease (GERD) and constipation. According to various estimates, the prevalence of gastrointestinal pathology among children with cerebral palsy reaches 70%, and nutritional status disorders are detected on average in half of children with cerebral palsy. The reason for such a high prevalence of gastroenterological problems is structural disorders of not only the central, but also the peripheral nervous system [3]. In the most severe and uncorrected cases, there is an inability to take food by mouth, which leads to unreasonably long tube feeding, cachexia, severe micronutrient deficiency, and a decrease in the rehabilitation potential and quality of life of the child with cerebral palsy and his family. In recent years, special attention has been paid to the assessment, prevention and treatment of gastroenterological diseases and nutritional disorders in children with neurological diseases, in particular cerebral palsy. The relevance of this area is confirmed by the results of the work of experts from the European Society of Pediatric Gastroenterologists, Hepatologists and Nutritionists (ESPGHAN), who in 2021 released “Clinical guidelines for the assessment and treatment of gastrointestinal and nutritional complications in children with neurological disorders” [2]. This document reflects the main problems and their possible solutions today.
Let's consider the main gastroenterological disorders that are most often observed in children with cerebral palsy, and methods for their correction.