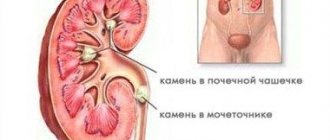
Ureteral stones and renal colic
Terrible pain in the lumbar region with nausea, vomiting, chills may indicate renal colic. This condition is caused by a violation of the outflow of urine from the kidney due to the migration of stones into the ureter.
Overstretching of the renal capsule occurs, which entails that very terrible pain. This condition is an indication for emergency hospitalization!
If you have a ureteral stone, several treatment options are available.
- If the stone is small - less than 1 cm, renal colic has been removed, there is no increase in body temperature - it is possible to prescribe special treatment without surgery with the hope of spontaneous passage of the stone. The patient should be warned about the possible complications of such tactics.
- Performing surgical treatment - endoscopic surgery - inserting an endoscope through the urethra, laser destruction of the stone with the removal of all fragments (contact lithotripsy) or performing remote lithotripsy - a procedure for crushing the stone using a large number of strokes focused on the stone. The specialist determines which method to use in each case, depending on the size, density of the stone and its location.
- If the stone has caused a complication - inflammation of the kidney - the first step is drainage of the kidney either with a special stent (inner tube connecting the kidney and bladder), or in severe cases of inflammation, a puncture of the kidney is performed through the lower back with installation of a tube in the kidney - nephrostomy - through which the flow temporarily flows urine. Next, antibacterial and anti-inflammatory therapy is carried out, and no earlier than 2 weeks later, endoscopic stone removal is performed.
Why does the disease appear?
There are a number of reasons why stones appear in the ureter:
- Presence of genetic predisposition. If a close relative of the patient had urolithiasis, then he is at risk.
- Geographical and climatic factor. The appearance of ureterolithiasis is more common in people who live in a country with a tropical climate.
- Failure to maintain proper nutrition. If a person regularly eats fatty foods, or those that contain oxalic and phosphoric acid, calcium enters the body in insufficient quantities, and the risk of stone formation increases.
- The urinary organs are abnormally developed, as a result of which the normal outflow of urine is disrupted. Such anomalies include stricture and ectopia of the ureter.
- Disturbed metabolic processes. If the metabolism of certain acids (uric, oxalic, phosphoric) is disrupted, salt crystals will appear in the urine.
- Infection and inflammatory process. The pH of urine changes, its colloidal state changes, and its dissolving ability is impaired.
- Long-term use of medications. This means taking glucocorticoids, tetracyclines, and antacids. Due to such medications, urine pH changes, calcium levels increase, etc.
- When dehydrated. The condition contributes to the fact that the concentration of urine increases; it will contain calcium salts, uric acid, etc.
- Impaired urine flow. This happens with strictures and vesicoureteral reflux. If the flow of urine is disrupted, crystals will form.
- Endogenous factor. This refers to the presence of hypercalciuria, hyperparathyroidism, prolonged immobilization, etc.
Kidney stones
In most cases, the presence of kidney stones is an indication for active action. Each case is considered individually. General principles
- Stones up to 1 cm that do not interfere with the flow of urine from the kidneys (kidney calyx stones), and also do not cause pain, can be observed by periodically performing an ultrasound, however, the patient should know that according to statistics, 50% of such stones will cause renal colic or other complications within 5 years
- Stones up to 15 mm, low density can be successfully treated by performing extracorporeal shock wave lithotripsy
- Stones larger than 15 mm, high-density stones (according to computed tomography) must be removed endoscopically - by performing a percutaneous removal technique (percutaneous nephrolithotomy or nephrolitholapaxy) or transurethral - through the ureter
- Stones associated with abnormalities, such as hydronephrosis, not only must be removed, but the kidney abnormality that is causing the stone formation must also be eliminated
Diagnosis of ureterolithiasis
Diagnosis of stones in the ureter is carried out on the basis of clinical symptoms, general examination, laboratory and instrumental examination (blood and urine tests, ultrasound and x-rays) and data collected during a patient interview.
The patient history interview includes:
- passport details;
- history of present illness;
- biographical data (information about the patient’s childhood, place of birth, place of residence);
- social and household data (professional biography of the patient, work schedule, conditions at the workplace, living conditions);
- information about family and relatives (presence of urinary tract pathologies, urolithiasis);
- data on previous diseases and surgical interventions;
- data on diet, bad habits, daily routine.
General inspection
During a general examination of the patient, in particular, the Tournai points are palpated, which correspond to the places of anatomical narrowing of the ureters.
Laboratory research
Since clinical blood tests for stones in the ureter are usually within normal limits, emphasis is placed on examining the patient’s urine:
- general urine analysis;
- bacteriological culture;
- pH determination.
Instrumental research
To localize stones, determine their size and shape, the following visual diagnostic methods are used:
- plain radiography of the abdominal cavity;
- survey and excretory urography;
- computed tomography of the kidneys;
- Ultrasound of the kidneys and ureters;
- ureteropyeloscopy (endoscopic examination of the ureter);
- chromocystoscopy (endoscopic examination of the kidneys and ureters using a contrast agent).
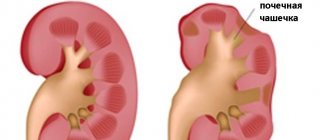
coral stone
A coral stone is a stone of the renal pelvis that has at least one spur into the calyx, or a stone that completely fills the renal pelvis. An incomplete staghorn stone fills only part of the kidney, a complete staghorn stone completely fills the renal calyces and renal pelvis.
Drawing. Coral stone of the right kidney.
The main method of treating coral stones is percutaneous endoscopic removal (percutaneous nephrolitholapaxy or percutaneous nephrolithotripsy).
Methods of surgical treatment of urolithiasis.
- External lithotripsy
- Percutaneous nephrolithotomy
- Retrograde ureterorenoscopy
Extracorporeal shock wave lithotripsy (ESWL) or extracorporeal shock wave lithotripsy (ESWL) is a non-invasive treatment for kidney and ureteral stones. The method was developed in the early 1980s in Germany, and became widely used with the introduction of the first lithotripter into clinical practice in 1983. Within a few years, ESWL became the standard treatment for small kidney and ureteral stones.
A lithotripter destroys stone using focused, high-intensity acoustic pulses. X-ray imaging or ultrasound imaging systems are used for guidance.
Typically, treatment begins at the lowest power level of the equipment, with long intervals between pulses, in order to adapt the patient's tissues and reduce the likelihood of bruising. The pulse frequency and power are then gradually increased so as to crush the stone more effectively. The final power level usually depends on the patient's pain threshold or the location of the stone (with kidney stones, maximum crushing modes often lead to renal hematomas and bleeding).
The criterion for effectiveness is the fragmentation of the stone into smaller pieces, which can then easily pass through the ureter and urethra. The crushing process takes about an hour. Placement of a ureteral stent may be used at the discretion of the urologist. The stent facilitates the passage of stone fragments, relieving swelling and expanding the ureter.
Extracorporeal lithotripsy works best for stones 4 mm to 1.5 cm in diameter that are still in the kidney. It can be used to crush stones that are also in the ureter, but with less success. ESWL is ineffective against some dense stones - oxalate monohydrate, brushite, the density of which exceeds 900 HU. ESWL is the least invasive treatment for stones, but provides a slower passage of stones than other more invasive treatments, such as ureteroscopy with contact laser lithotripsy or percutaneous nephrolithotomy. The passage of stone fragments may take several days or weeks and may cause moderate pain. There are often indications for kidney drainage by installing a stent or percutaneous nephrostomy. It is recommended to examine stone fragments collected by the patient. ESWL is not without risk. Shock waves can lead to capillary damage, renal parenchymal or subcapsular hemorrhages. This can lead to long-term consequences such as kidney failure, diabetes and hypertension. The overall complication rate of ESWL is in the range of 5-20%.
Percutaneous nephrolithotomy
Percutaneous nephrolithotomy or PCNL (also percutaneous puncture nephrolitholapaxy), a procedure for removing medium and large kidney stones by inserting a special instrument into the kidney - a nephroscope along a path created through the skin of the patient's lumbar region. PCNL was first performed in Sweden in 1973 as a less invasive alternative to open kidney surgery. The term "percutaneous" means that the procedure is done through a puncture of the skin (no incisions).
Classification of stones
Considering the anatomical location, stones can be located:
- Upper third of the ureter. The location of such stones is the area where the ureter anatomically narrows - the ureteropelvic segment.
- Middle third. The location is the second anatomical narrowing of the ureter - the border line.
- Lower third. The location is the third anatomical narrowing of the ureter - the vesicoureteral segment.
- On the one side. Stones are present in one ureter, right or left.
- On both sides. Stones are present in both the left and right ureter.
Considering the number of stones, they are:
- Single.
- Multiple.
Considering the frequency of occurrence, stones are:
- Primary. Can be found in rare cases. The initial site of stone formation is the ureter.
- Secondary. First, the stone forms in the kidney, then enters the ureter.
- Recurrent. This means that re-formation of stones has occurred.
Considering the chemical composition, stones are:
- Urate. These stones contain calcium and uric acid salts. Urate stones are formed due to improper nutrition, that is, if a person’s diet contains excessive amounts of salty and acidic foods. In addition, such stones are formed due to impaired metabolic processes, a sedentary lifestyle, inflammatory processes in the genitourinary organs, dehydration, and vitamin deficiency. Urate stones have a loose structure, so they can dissolve if the patient drinks a lot of liquid.
- Oxalate. They are a common type of stones. They can be found in almost 85% of cases. The formation of such stones occurs if oxalic acid enters the body in large quantities or its metabolism and excretion are impaired. After entering the urine, a reaction of oxalic acid and calcium occurs, and the formation of crystals begins. They are called oxalates. In addition, oxalate stones appear if magnesium and vitamin B6 are present in the body in insufficient quantities, as well as with chronic pyelonephritis and diabetes mellitus. This type of stone has a dark brown or black color, an uneven surface with sharp thorns.
- Phosphate. Such stones are detected in 80% of all cases. The stones contain calcium salts of phosphate acid. The color is light gray or white. Phosphate stones have a loose structure and a smooth surface. The main reason for the formation is a chronic inflammatory process in the urinary organs. The main danger is the rapid increase in the size of the stone.
- Xanthine and cystine. Occurs in rare cases. The reason for the formation of such stones is impaired amino acid metabolism, a chronic inflammatory process, and the presence of a genetic predisposition.
- Mixed. Almost half of all cases are a mixed type of stone. They are formed due to various factors. This can be due to poor nutrition, long-term use of certain medications, impaired metabolic processes, hormonal imbalance, inflammation, etc.
Considering the ability to absorb x-rays and display on an x-ray, stones can be radiopaque, low-contrast, or non-contrast.
What increases the likelihood of stones forming in the ureter
- Drinking poor quality water.
- The presence of a hereditary predisposition.
- Age indicator.
- For obesity.
- If metabolic processes are disrupted.
- Failure to maintain an active lifestyle.
- A person drinks little water.
- Doesn't eat right.
Preventive actions
- Drink about 2 liters of liquid every day. The consumption of carbonated drinks, tea, and coffee is prohibited.
- Eat properly.
- Adhere to a certain diet that is prescribed for ureteral stones.
- Ensure regular medical examinations.
- Take a vitamin complex.
- Promptly contact the clinic for the treatment of inflammatory processes in the urinary organs.
- Get rid of what caused the impaired outflow of urine.
Target
The goal of PCNL is to remove kidney stones to reduce pain, bleeding or urinary tract obstruction, and/or urinary tract infection. Kidney stones range in size from microscopic crystals to huge stones up to several centimeters (huge kidney stones occupy all the kidney cavities and begin to resemble corals - hence the term coral stone). Standard percutaneous nephrolithotomy is performed under general anesthesia and takes about 40 minutes - 4 hours. The surgeon makes a small incision, approximately 0.5 - 1.3 cm in length, in the patient's lumbar region. In percutaneous nephrolithotomy, the surgeon inserts a needle through the patient's skin directly into the kidneys using fluoroscopy and ultrasound guidance. The puncture tract is expanded and a nephroscope is installed in the kidney - an instrument that allows optical visualization of the renal cavity system. An ultrasound or laser probe is delivered through the nephroscope to crush large kidney stones. Pieces of stones are removed with instruments, and at the end a nephrostomy tube is installed to drain the kidney on the first day after surgery. In some cases, a ureteral stent is installed.
Drawing. Positioning the patient. Drawing. Creation of access to the renal cavity system.
Drawing. Nephroscopy.