Moxifloxacine
Absorption and bioavailability
When taken orally, moxifloxacin is absorbed quickly and almost completely. Absolute bioavailability is about 91%.
The pharmacokinetics of moxifloxacin when taken at a dose of 50 to 1200 mg once, as well as 600 mg/day for 10 days, is linear. The equilibrium state is achieved within 3 days.
After a single dose of 400 mg of moxifloxacin, the maximum concentration (Cmax) in the blood plasma is reached within 0.5-4 hours and is 3.1 mg/l. After oral administration of 400 mg of moxifloxacin once daily, Cssmax (maximum equilibrium concentration) and Cssmin (minimum equilibrium concentration) are 3.2 mg/L and 0.6 mg/L, respectively.
When taking moxifloxacin with food, there is a slight increase in the time to reach Cmax (by 2 hours) and a slight decrease in Cmax (by approximately 16%), while the duration of absorption does not change. However, these data do not have clinical significance, and the drug can be used regardless of food intake.
Distribution
Moxifloxacin is rapidly distributed in tissues and organs and binds to blood proteins (mainly albumin) by approximately 45%. The volume of distribution is approximately 2 l/kg.
High concentrations of moxifloxacin, exceeding those in blood plasma, are created in the lung tissue (including in epithelial fluid, alveolar macrophages), in the nasal sinuses (maxillary and ethmoid sinuses), in nasal polyps, in exudate from the site of skin inflammation. In interstitial fluid and saliva, moxifloxacin is determined in a free form, not bound to proteins, in a concentration higher than in plasma. In addition, high concentrations of moxifloxacin are determined in the abdominal organs and peritoneal fluid, as well as in the tissues of the female genital organs.
Metabolism
After passing through the 2nd phase of biotransformation, moxifloxacin is excreted from the body by the kidneys and intestines, both unchanged and in the form of inactive sulfo compounds (M1) and glucuronides (M2). Moxifloxacin is not biotransformed by the microsomal cytochrome P450 system.
Metabolites M1 and M2 are present in blood plasma in concentrations lower than the parent compound and do not have a negative effect on the body in terms of safety and tolerability.
Removal
The half-life of moxifloxacin is approximately 12 hours.
The average total clearance after administration of a dose of 400 mg ranges from 179 to 246 ml/min.
Renal clearance is 24-53 ml/min, indicating partial tubular reabsorption of the drug. The mass balance of parent compound and phase 2 metabolites is approximately 96-98%, indicating the absence of oxidative metabolism. About 22% of a single dose (400 mg) is excreted unchanged by the kidneys, about 26% by the intestines.
Pharmacokinetics in different patient groups
Age, gender and ethnicity
A study of the pharmacokinetics of moxifloxacin in men and women revealed differences of 33% in terms of area under the concentration-time pharmacokinetic curve (AUC) and Cmax.
The absorption of moxifloxacin did not depend on gender.
Differences in AUC and Cmax were due to differences in weight rather than gender and are not clinically significant.
There were no clinically significant differences in the pharmacokinetics of moxifloxacin in patients of different ethnic groups and different ages.
Children
The pharmacokinetics of moxifloxacin in children has not been studied.
Renal dysfunction
There were no significant changes in the pharmacokinetics of moxifloxacin in patients with impaired renal function (including patients with creatinine clearance <30 ml/min/1.73 m2) and in patients on continuous hemodialysis and long-term ambulatory peritoneal dialysis.
Liver dysfunction
There were no significant differences in moxifloxacin concentrations in patients with impaired liver function (Child-Pugh classes A, B) compared with healthy volunteers and patients with normal liver function.
Moxifloxacin tablet p/o 400 mg N5 (Vertex)
In some cases, after the first use of the drug, hypersensitivity and allergic reactions may develop, which should be reported to your doctor immediately. Very rarely, even after the first use of the drug, anaphylactic reactions can progress to life-threatening anaphylactic shock. In these cases, treatment with moxifloxacin should be discontinued and the necessary therapeutic measures (including anti-shock) should be taken. QT interval prolongation may occur in some patients when using moxifloxacin. Moxifloxacin should be used with caution in women and elderly patients. Because women have a longer QT interval than men, they may be more sensitive to drugs that prolong the QT interval. Elderly patients are also more susceptible to drugs that affect the QT interval. The degree of QT interval prolongation may increase with increasing drug concentrations, so the recommended dose should not be exceeded. However, in patients with pneumonia, no correlation was observed between moxifloxacin plasma concentrations and QT interval prolongation. Prolongation of the QT interval is associated with an increased risk of ventricular arrhythmias, including polymorphic ventricular tachycardia. None of the 9,000 patients treated with moxifloxacin experienced cardiovascular events or deaths associated with QT prolongation. However, in patients with conditions predisposing to arrhythmias, the risk of developing ventricular arrhythmias may be increased when using moxifloxacin. In this regard, moxifloxacin is contraindicated in patients with established prolongation of the QT interval, patients with uncorrected hypokalemia, and patients taking drugs that prolong the QT interval (see section “Interaction with other drugs”). Due to the risk of additive effects on the QT interval, moxifloxacin is contraindicated in patients with conditions predisposing to arrhythmias, such as clinically significant bradycardia, clinically significant heart failure, rhythm disturbances accompanied by clinical symptoms, acute myocardial ischemia; patients with liver cirrhosis (since in this category of patients the risk of developing QT prolongation cannot be excluded). Cases of fulminant hepatitis, potentially leading to liver failure (including fatal cases), have been reported while taking moxifloxacin (see section "Side effects"). The patient should be informed that if symptoms of liver failure occur, it is necessary to consult a doctor before continuing treatment with moxifloxacin. Cases of bullous skin lesions (Stevens-Johnson syndrome, toxic epidermal necrolysis) have been reported when taking moxifloxacin. The patient should be informed that if symptoms of skin or mucous membrane lesions occur, they should consult a doctor before continuing treatment with moxifloxacin. The use of quinolone drugs is associated with a possible risk of developing seizures. Moxifloxacin should be used with caution in patients with diseases of the central nervous system and with conditions suspected of involving the central nervous system, predisposing to seizures or lowering the threshold for seizure activity. The use of broad-spectrum antibacterial drugs, including moxifloxacin, is associated with the risk of developing antibiotic-associated pseudomembranous colitis. This diagnosis should be kept in mind in patients who develop severe diarrhea during treatment with moxifloxacin. In this case, the drug should be discontinued and appropriate therapy should be immediately prescribed. Drugs that inhibit intestinal motility are contraindicated in the development of severe diarrhea. Moxifloxacin should be used with caution in patients with myasthenia gravis due to possible exacerbation of the disease. During therapy with quinolones, including moxifloxacin, tendonitis and tendon rupture may develop, especially in elderly people and patients receiving glucocorticosteroids. Cases have been described that occurred within several months after completion of treatment. At the first symptoms of pain or inflammation at the site of injury, you should stop taking the drug and unload the affected limb. When using quinolones, photosensitivity reactions are observed. However, during preclinical and clinical studies, as well as when using moxifloxacin in practice, no photosensitivity reactions were observed. However, patients receiving moxifloxacin should avoid direct sunlight and ultraviolet light. The use of the drug in patients with complicated inflammatory diseases of the pelvic organs (for example, associated with tubo-ovarian or pelvic abscesses) is not recommended. The use of moxifloxacin is not recommended to treat infections caused by methicillin-resistant Staphylococcus aureus (MRSA). In cases of suspected or confirmed infections caused by MRSA, treatment with appropriate antibacterial drugs should be prescribed (see section "Pharmacodynamics"). The ability of Moxifloxacin to inhibit the growth of mycobacteria may cause in vitro interaction of moxifloxacin with the test for Mycobacterium spp., leading to false negative results when analyzing samples from patients who are being treated with moxifloxacin during this period. In patients treated with quinolones, including moxifloxacin, cases of sensory or sensorimotor polyneuropathy leading to paresthesia, hypoesthesia, dysesthesia or weakness have been described. Patients treated with moxifloxacin should be warned to seek immediate medical attention before continuing treatment if symptoms of neuropathy, including pain, burning, tingling, numbness or weakness, occur (see section "Side Effects"). Psychiatric reactions can occur even after the first prescription of fluoroquinolones, including moxifloxacin. In very rare cases, depression or psychotic reactions progress to the occurrence of suicidal thoughts and behavior with a tendency to self-harm, including suicide attempts (see section "Side effects"). If patients develop such reactions, the drug should be discontinued and the necessary measures taken. Caution must be exercised when prescribing moxifloxacin to patients with psychosis and patients with a history of mental illness. Due to the widespread and increasing incidence of infections caused by fluoroquinolone-resistant Neisseria gonorrhoeae, moxifloxacin monotherapy should not be used in the treatment of patients with pelvic inflammatory diseases. Unless the presence of fluoroquinolone-resistant N. gonorrhoeae is excluded. If the presence of fluoroquinolone-resistant N. gonorrhoeae cannot be excluded, consideration should be given to supplementing empiric moxifloxacin therapy with an appropriate antibiotic that is active against N. gonorrhoeae (eg, a cephalosporin). Effect of the drug on the ability to drive vehicles and other mechanisms: Fluoroquinolones, including moxifloxacin, may impair the ability of patients to drive a car and engage in other potentially hazardous activities that require increased attention and speed of psychomotor reactions due to their effect on the central nervous system.
Avelox
Use during pregnancy and breastfeeding
The safety of moxifloxacin during pregnancy has not been established and its use is contraindicated.
Cases of reversible joint damage have been described in children receiving some quinolones, but this effect has not been reported in the fetus (when used by the mother during pregnancy). Reproductive toxicity has been shown in animal studies. The potential risk to humans is unknown.
Like other quinolones, moxifloxacin causes cartilage damage in large joints in premature animals. Preclinical studies have shown that small amounts of moxifloxacin are excreted in breast milk. There are no data on its use in women during lactation. Therefore, the use of moxifloxacin during breastfeeding is contraindicated.
Use for liver dysfunction
Patients with impaired liver function do not require a change in dosage regimen.
The drug should be used with caution in patients with liver cirrhosis.
Use for renal impairment
Patients with impaired renal function (including those with CC <30 ml/min/1.73 m2), as well as patients on continuous hemodialysis and long-term ambulatory peritoneal dialysis, do not require changes in the dosage regimen.
Use in children
Contraindicated: children and adolescents under 18 years of age.
Use in elderly patients
Elderly patients do not require changes in the dosage regimen.
special instructions
In some cases, after the first use of the drug, hypersensitivity and allergic reactions may develop, which should be reported to your doctor immediately. Very rarely, even after the first use of the drug, anaphylactic reactions can progress to life-threatening anaphylactic shock. In these cases, treatment with Avelox® should be stopped and the necessary therapeutic measures (including anti-shock) should be started immediately.
When using Avelox®, some patients may experience prolongation of the QT interval.
Avelox® should be used with caution in women and elderly patients. Because women have a longer QT interval than men, they may be more sensitive to drugs that prolong the QT interval. Elderly patients are also more susceptible to drugs that affect the QT interval.
The degree of QT interval prolongation may increase with increasing drug concentrations, so the recommended dose should not be exceeded. Prolongation of the QT interval is associated with an increased risk of ventricular arrhythmias, including polymorphic ventricular tachycardia. However, in patients with pneumonia, a correlation between moxifloxacin plasma concentrations and QT interval prolongation was noted. None of the 9,000 patients receiving Avelox® experienced cardiovascular complications or deaths associated with QT prolongation.
When using Avelox®, the risk of developing ventricular arrhythmias may increase in patients with conditions predisposing to arrhythmias. In this regard, Avelox® is contraindicated in:
- changes in electrophysiological parameters of the heart, expressed in prolongation of the QT interval (congenital or acquired documented prolongation of the QT interval, electrolyte disturbances, especially uncorrected hypokalemia, clinically significant bradycardia, clinically significant heart failure with reduced left ventricular ejection fraction, a history of indications of rhythm disturbances, accompanied by clinical symptoms);
- use with other drugs that prolong the QT interval.
Avelox® should be used with caution:
- in patients with potentially proarrhythmic conditions, such as acute myocardial ischemia;
- in patients with liver cirrhosis (since in this category of patients the risk of developing a prolongation of the QT interval cannot be excluded).
Cases of fulminant hepatitis, potentially leading to liver failure (including fatal cases), have been reported while taking Avelox®. The patient should be informed that if symptoms of liver failure occur, it is necessary to consult a doctor before continuing treatment with Avelox®.
Cases of bullous skin lesions (such as Stevens-Johnson syndrome or toxic epidermal necrolysis) have been reported while taking Avelox®. The patient should be informed that if symptoms of skin or mucous membrane lesions appear, it is necessary to consult a doctor before continuing treatment with Avelox®.
The use of quinolone drugs is associated with a possible risk of developing seizures. Avelox® should be used with caution in patients with diseases of the central nervous system and disorders of the central nervous system that predispose to seizures or reduce the threshold for seizure activity.
The use of broad-spectrum antibacterial drugs, including Avelox®, is associated with a risk of developing pseudomembranous colitis. This diagnosis should be kept in mind in patients who develop severe diarrhea during treatment with Avelox®. In this case, appropriate therapy should be prescribed immediately. Drugs that inhibit intestinal motility are contraindicated in the development of severe diarrhea.
Avelox® should be used with caution in patients with myasthenia gravis due to a possible exacerbation of the disease.
During therapy with quinolones, incl. moxifloxacin, tendonitis and tendon rupture may develop, especially in the elderly and patients receiving corticosteroids. Cases have been described that occurred within several months after completion of treatment. At the first symptoms of pain or inflammation at the site of injury, the drug should be stopped and the affected limb should be unloaded.
When using quinolones, photosensitivity reactions are observed. However, during preclinical and clinical studies, as well as when using the drug Avelox® in practice, no photosensitivity reactions were observed. However, patients receiving Avelox® should avoid exposure to direct sunlight and ultraviolet radiation.
The use of the drug in the form of tablets for oral administration is not recommended in patients with complicated inflammatory diseases of the pelvic organs (for example, associated with tubo-ovarian or pelvic abscesses).
Moxifloxacin is not recommended for the treatment of infections caused by methicillin-resistant Staphylococcus aureus (MRSA). Suspected or confirmed MRSA infections should be treated with appropriate antibacterial drugs.
The ability of Avelox® to inhibit the growth of mycobacteria may cause in vitro interaction of moxifloxacin with the test for Mycobacterium spp., leading to false negative results when analyzing samples from patients who are being treated with Avelox® during this period.
In patients treated with quinolones, including Avelox®, cases of sensory or sensorimotor polyneuropathy leading to paresthesia, hypoesthesia, dysesthesia or weakness have been described. Patients being treated with Avelox should be advised to seek immediate medical attention before continuing treatment if symptoms of neuropathy, including pain, burning, tingling, numbness or weakness, occur.
Psychiatric reactions can occur even after the first prescription of fluoroquinolones, including moxifloxacin. In very rare cases, depression or psychotic reactions progress to suicidal thoughts and behavior with a tendency to self-harm, including suicide attempts. If patients develop such reactions, the drug Avelox® should be discontinued and the necessary measures taken. Caution should be exercised when prescribing Avelox® to patients with a history of psychosis and/or psychiatric illness.
Due to the widespread and increasing incidence of infections caused by fluoroquinolone-resistant Neisseria gonorrhoeae, moxifloxacin monotherapy should not be used in the treatment of patients with pelvic inflammatory disease, unless the presence of fluoroquinolone-resistant N. gonorrhoeae is excluded. If the presence of fluoroquinolone-resistant N. gonorrhoeae cannot be excluded, consideration should be given to supplementing empiric moxifloxacin therapy with an appropriate antibiotic that is active against N. gonorrhoeae (eg, a cephalosporin).
As with other fluoroquinolones, changes in blood glucose concentrations, including hypo- and hyperglycemia, were observed when using Avelox®. During therapy with Avelox®, dysglycemia occurred predominantly in elderly patients with diabetes mellitus receiving concomitant therapy with oral hypoglycemic drugs (for example, sulfonylureas) or insulin. When treating patients with diabetes mellitus, careful monitoring of blood glucose concentrations is recommended.
Impact on the ability to drive vehicles and operate machinery
Fluoroquinolones, including moxifloxacin, may impair the ability of patients to drive a car and engage in other potentially hazardous activities that require increased attention and speed of psychomotor reactions due to their effects on the central nervous system and visual impairment.
Moxifloxacin
An antimicrobial agent from the group of fluoroquinolones, it has a bactericidal effect. Shows activity against a wide range of gram-positive and gram-negative microorganisms, anaerobic, acid-fast and atypical bacteria: Mycoplasma spp., Chlamydia spp., Legionella spp. Effective against bacterial strains resistant to beta-lactams and macrolides. Active against most strains of microorganisms: gram-positive - Staphylococcus aureus (including strains insensitive to methicillin), Streptococcus pneumoniae (including strains resistant to penicillin and macrolides), Streptococcus pyogenes (group A); gram-negative - Haemophilus influenzae (including both beta-lactamase-producing and non-beta-lactamase-producing strains), Haemophilus parainfluenzae, Klebsiella pneumoniae, Moraxella catarrhalis (including both beta-lactamase-producing and non-beta-lactamase-producing strains), Escherichia coli, Enterobacter cloacae; atypical - Chlamydia pneumoniae, Mycoplasma pneumoniae. According to in vitro studies, although the microorganisms listed below are sensitive to the drug, its safety and effectiveness in the treatment of infections have not been established. Gram-positive microorganisms: Streptococcus milleri, Streptococcus mitior, Streptococcus agalactiae, Streptococcus dysgalactiae, Staphylococcus cohnii, Staphylococcus epidermidis (including strains sensitive to methicillin), Staphylococcus haemolyticus, Staphylococcus hominis, Staphylococcus saprophyticus, Staphylococcus simulans , Corynebacterium diphtheriae. Gram-negative microorganisms: Bordetella pertussis, Klebsiella oxytoca, Enterobacter aerogenes, Enterobacter agglomerans, Enterobacter Intermedius, Enterobacter sakazaki, Proteus mirabilis, Proteus vulgaris, Morganella morganii, Providencia rettgeri, Providencia stuartii. Anaerobic microorganisms: Bacteroides distasonis, Bacteroides eggerthii, Bacteroides fragilis, Bacteroides ovatus, Bacteroides thetaiotaornicron, Bacteroides uniformis, Fusobacterium spp., Porphyromonas spp., Porphyromonas anaerobius, Porphyromonas asaccharolyticus, Porphyromonas magnus, Prevot ella spp., Propionibacterium spp., Clostridium perfringens, Clostridium ramosum. Atypical microorganisms: Legionella pneumophila, Caxiella burnettii.
Moxifloxacin, 400 mg, film-coated tablets, 5 pcs.
In some cases, after the first use of the drug, hypersensitivity and allergic reactions may develop, which should be reported to your doctor immediately. Very rarely, even after the first use of the drug, anaphylactic reactions can progress to life-threatening anaphylactic shock. In these cases, treatment with Moxifloxacin should be stopped and the necessary therapeutic measures (including anti-shock) should be started immediately.
When using moxifloxacin, some patients may experience prolongation of the QT interval. Moxifloxacin should be used with caution in women and elderly patients. Because women have a longer QT interval than men, they may be more sensitive to drugs that prolong the QT interval. Elderly patients are also more susceptible to drugs that affect the QT interval.
Prolongation of the QT interval is associated with an increased risk of ventricular arrhythmias, including polymorphic ventricular tachycardia.
The degree of QT prolongation may increase with increasing concentrations of moxifloxacin, so the recommended dose should not be exceeded. However, in patients with pneumonia, no correlation was observed between moxifloxacin plasma concentrations and QT interval prolongation. None of the 9,000 patients treated with moxifloxacin experienced cardiovascular complications or deaths associated with QT prolongation. When using moxifloxacin, the risk of developing ventricular arrhythmias may increase in patients with conditions predisposing to arrhythmias.
In this regard, moxifloxacin is contraindicated in:
- changes in electrophysiological parameters of the heart, expressed in prolongation of the QT interval: congenital or acquired documented prolongation of the QT interval, electrolyte disturbances, especially uncorrected hypokalemia; clinically significant bradycardia; clinically significant heart failure with reduced left ventricular ejection fraction; a history of rhythm disturbances accompanied by clinical symptoms;
- use with other drugs that prolong the QT interval (see section “Interaction with other drugs”).
Moxifloxacin should be used with caution:
- in patients with potentially proarrhythmic conditions such as acute myocardial ischemia and cardiac arrest;
- in patients with liver cirrhosis (since in this category of patients the risk of developing a prolongation of the QT interval cannot be excluded).
Cases of fulminant hepatitis, potentially leading to liver failure (including fatal cases), have been reported while taking Moxifloxacin (see section "Side effects"). The patient should be informed that if symptoms of liver failure occur, it is necessary to consult a doctor before continuing treatment with moxifloxacin.
Cases of bullous skin lesions such as Stevens-Johnson syndrome or toxic epidermal necrolysis have been reported while taking moxifloxacin (see section "Side effects"). The patient should be informed that if symptoms of skin or mucous membrane lesions occur, they should consult a doctor before continuing treatment with moxifloxacin.
The use of quinolone drugs is associated with a possible risk of developing seizures. Moxifloxacin should be used with caution in patients with diseases of the central nervous system and with disorders of the central nervous system that predispose to seizures or lower the threshold for seizure activity.
The use of broad-spectrum antibacterial drugs, including moxifloxacin, is associated with a risk of developing pseudomembranous colitis. This diagnosis should be considered in patients who experience severe diarrhea during treatment with moxifloxacin. In this case, appropriate therapy should be prescribed immediately. Drugs that inhibit intestinal motility are contraindicated in the development of severe diarrhea.
Moxifloxacin should be used with caution in patients with myasthenia gravis due to possible exacerbation of the disease.
During therapy with quinolones, including moxifloxacin, tendonitis and tendon rupture may develop, especially in the elderly and patients receiving glucocorticosteroids. Cases have been described that occurred within several months after completion of treatment. At the first symptoms of pain or inflammation at the site of injury, the drug should be stopped and the affected limb should be unloaded. When using quinolones, photosensitivity reactions are observed. However, during preclinical and clinical studies, as well as with the use of moxifloxacin in practice, no photosensitivity reactions were observed. However, patients receiving moxifloxacin should avoid exposure to direct sunlight and ultraviolet light.
The use of the drug in the form of tablets for oral administration is not recommended in patients with complicated inflammatory diseases of the pelvic organs (for example, associated with tubo-ovarian or pelvic abscesses).
The use of moxifloxacin is not recommended to treat infections caused by methicillin-resistant Staphylococcus aureus (MRSA). In cases of suspected or confirmed infections caused by MRSA, treatment with appropriate antibacterial drugs should be prescribed (see section "Pharmacodynamics").
The ability of moxifloxacin to inhibit the growth of mycobacteria may cause invitromoxifloxacin to interact with the test for Mycobacterium spp., leading to false negative results when analyzing samples from patients who are being treated with moxifloxacin during this period.
In patients treated with quinolones, including moxifloxacin, cases of sensory or sensorimotor polyneuropathy leading to paresthesia, hypoesthesia, dysesthesia or weakness have been described. Patients treated with moxifloxacin should be warned to seek immediate medical attention before continuing treatment if symptoms of neuropathy, including pain, burning, tingling, numbness or weakness, occur (see section "Side Effects").
Psychiatric reactions may occur even after the first use of fluoroquinolones, including moxifloxacin. In very rare cases, depression or psychotic reactions progress to the occurrence of suicidal thoughts and behavior with a tendency to self-harm, including suicide attempts (see section "Side effects"). If patients develop such reactions, moxifloxacin should be discontinued and the necessary measures taken. Caution should be exercised when using moxifloxacin in patients with a history of psychosis and/or psychiatric illness.
Due to the widespread and increasing incidence of infections caused by fluoroquinolone-resistant Neisseriagonorrhoeae, patients with pelvic inflammatory disease should not be treated with moxifloxacin monotherapy unless fluoroquinolone-resistant N is present. gonorrhoeae excluded. If it is not possible to exclude the presence of fluoroquinolone-resistant N. gonorrhoeae, consideration must be given to supplementing empiric moxifloxacin therapy with an appropriate antibiotic that is active against N. gonorrhoeae (eg, a cephalosporin).
Dysglycemia
As with other fluoroquinolones, changes in blood glucose concentrations, including hypo- and hyperglycemia, were observed with the use of moxifloxacin. During therapy with moxifloxacin, dysglycemia occurred predominantly in elderly patients with diabetes mellitus receiving concomitant therapy with oral hypoglycemic drugs (for example, sulfonylureas) or insulin. When conducting treatment in patients with diabetes mellitus, careful monitoring of blood glucose concentrations is recommended (see section “Side Effects”).
Moxifloxacin in the treatment of pelvic inflammatory diseases
Yu.E. Dobrokhotova, E.Yu. Dubner RGMU, City Clinical Hospital No. 1 named after. N.I. Pirogov, Moscow
ABSTRACT
Moxifloxacin in the treatment of pelvic inflammatory diseases
Pelvic inflammatory diseases (PID) are among the common gynecological diseases, and their treatment represents a serious medical problem. An important place in the treatment of PID belongs to fluoroquinolones, the only representative of the fourth generation in Russia is moxifloxacin (Avelox). Moxifloxacin is characterized by a wide antimicrobial spectrum (gram-positive and gram-negative aerobic bacteria and anaerobes, atypical microorganisms), favorable pharmacokinetic properties, allowing dosing of the drug once a day, good tolerability and the absence of serious adverse events noted with the use of other fluoroquinolones. The results of a study are presented, the purpose of which was to compare two regimens of antibacterial therapy in 35 patients with PID: two-component (ciprofloxacin and metronidazole) and monotherapy (moxifloxacin). The results of the study confirm the literature data and indicate that the effectiveness of moxifloxacin monotherapy for PID is not inferior to that of combination therapy with 2-3 antibacterial drugs, which makes it possible to use moxifloxacin for initial empirical antibacterial therapy of this group of diseases.
The problem of pelvic inflammatory diseases (PID) is still relevant. Inflammatory diseases of the uterine appendages significantly affect the health of women of reproductive age. PID is characterized by a long course with recurrence of the pathological process. As a consequence of the inflammatory disease, adhesions often form and the anatomical relationships and functions of the pelvic organs are disrupted.
According to WHO, complete occlusion of the fallopian tubes was found in 14.2%, and partial occlusion in 9.2% of patients who had inflammation of the appendages. According to Russian authors, obstructive lesions of the fallopian tubes occur in 29.9–32% of such women. In Moscow, PID accounts for 28–30% of the structure of gynecological diseases, and this figure, unfortunately, does not tend to decrease.
In recent years, gonorrheal infection as a cause of PID is gradually giving way to staphylococcus and E. coli; associations of microorganisms (staphylococci, enterobacteria, streptococci, chlamydia, gonococci) are becoming increasingly important. According to Zuev V.M. (1998), in 96.7% of patients with PID, polymicrobial associations are found, in which the dominant role belongs to opportunistic microorganisms (Escherichia coli, enterococcus, epidermal staphylococcus) and bacteroids. Among other microorganisms, chlamydia (12.1%), mycoplasma (9.2%), ureaplasma (11.6%), and gardnerella (19.3%) were identified. Most researchers believe that non-spore-forming anaerobes (bacteroides, fusobacteria, peptostreptococci) play a predominant role in the development of purulent-destructive processes in the uterine appendages. Along with aerobic-anaerobic associations of microorganisms, frequent components in the structure of pathogens of the purulent inflammatory process are vector-borne infections, primarily gonococci, chlamydia and viruses. Identification of pathogens is extremely important for the selection of antibacterial therapy.
A serious problem in the treatment of inflammatory processes is the selection as a result of antibacterial therapy of antibiotic-resistant microorganisms with the formation of strains that produce β-lactamase. These include varieties of bacteroides, gonococcus, Staphylococcus aureus, and enterobacteria. While the need for antibacterial therapy is beyond doubt, there is no consensus regarding the choice of optimal antibacterial therapy regimens for various forms of gynecological infection, especially before obtaining the results of a microbiological study.
From the standpoint of treatment tactics, it is advisable to distinguish between empirical and targeted antibacterial therapy for PID. Empirical antibacterial therapy is based on data on the polymicrobial etiology of abdominal infection involving Escherichia coli, enterobacteria and anaerobic microorganisms. Effective control of these pathogens can be achieved using combination antibacterial therapy or by prescribing monotherapy. Empirical antibacterial therapy is especially relevant in emergency gynecology and involves the earliest possible prescription of effective antibiotics even before obtaining microbiological confirmation of the etiological factor. New prospects in the treatment of PID have opened up with the introduction into practice of broad-spectrum antibiotics that are active against the most significant causative agents of infection of the pelvic organs. Fluoroquinolones can be fully included among them. These drugs have a wide spectrum of antimicrobial action, are well tolerated, are capable of creating high concentrations in the tissues of the pelvic organs, and are characterized by a low frequency of adverse reactions.
The molecule of each compound from the quinolone class contains a six-membered ring with a COOH group at position 3 and a keto group at position 4 - a pyridone fragment that determines the main mechanism of action - inhibition of DNA gyrase and, accordingly, antimicrobial activity. Based on this chemical feature, these compounds are sometimes called “4-quinolones.” The severity of DNA gyrase inhibition, the breadth of the antimicrobial spectrum, and the pharmacokinetic properties of individual drugs depend on the overall structure of the molecule and the nature of the radicals at various positions in the cycle. Despite the similarity in the chemical structure of non-fluorinated and fluorinated quinolones, they differ significantly in their properties. This gives grounds to consider fluoroquinolones as an independent group within the quinolone class.
The so-called old fluoroquinolones (ciprofloxacin, ofloxacin, etc.) have preferential activity against gram-negative bacteria. The high activity of these drugs against the Enterobacteriaceae family, including multi-resistant strains, has been established. Neisseria gonorrhoeae and Neisseria meningitidis are very sensitive to fluoroquinolones. Fluoroquinolones also have a pronounced effect on other gram-negative bacteria (Campylobacter jejuni, Moraxella catarrhalis), including those producing β-lactamase [1, 2].
In recent years, the attention of researchers working in the field of chemotherapy of bacterial infections has been attracted by the increased frequency of isolation of gram-positive microorganisms, often with resistance to various antibacterial drugs. In this regard, new fluoroquinolones are of great interest, which, while maintaining the high activity against gram-negative microorganisms characteristic of all drugs in this group, also effectively act on gram-positive bacteria. The “gold standard” of second-generation quinolones has become ciprofloxacin, which is used with great success to treat many infections. The disadvantages of drugs of this generation include low activity against pneumococcus and some other cocci, chlamydia, mycoplasmas and anaerobes. These shortcomings were overcome during the development of third generation fluoroquinolones. One of the first drugs in this group was levofloxacin, which was superior in activity against pneumococcus and atypical pathogens to previous fluoroquinolones. Further modifications of the chemical structure led to the emergence of fourth generation fluoroquinolones, which are also active against anaerobes. However, some of the newly developed drugs, due to serious adverse reactions associated with their use, were either excluded from clinical practice (trovafloxacin, grepafloxacin, etc.) or limited in use (sparfloxacin) [3, 4]. The only representative of the fourth generation fluoroquinolones registered in Russia is moxifloxacin (Avelox).
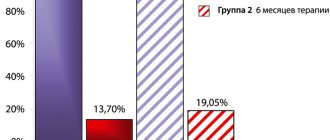
Moxifloxacin is characterized by a wide antimicrobial spectrum (gram-positive and gram-negative aerobic bacteria and anaerobes, atypical microorganisms), favorable pharmacokinetic properties (high bioavailability, good tissue penetration, long half-life), allowing dosing of the drug once a day, good tolerability and the absence of serious adverse events observed with the use of other fluoroquinolones. The mechanism of action of moxifloxacin is associated with the inhibition of DNA gyrase, the main enzyme of the bacterial cell responsible for the process of normal DNA biosynthesis. At the same time, moxifloxacin inhibits 2 enzymes at once - topoisomerase-2 and topoisomerase-4, which guarantees a very low probability of mutations in both enzymes simultaneously and, accordingly, a low probability of developing resistance to the drug. Moxifloxacin is characterized by high bactericidal activity and a clinically significant post-antibiotic period [5–7]. To date, the high clinical and bacteriological effectiveness of moxifloxacin has been proven not only for respiratory infections, but also for bacterial infections of other localizations, in particular for inflammatory diseases of the pelvic organs. Thus, in one of the large controlled international studies (43 centers from 14 countries), the effectiveness of 14-day use of moxifloxacin (orally 400 mg once daily) was compared with ciprofloxacin (500 mg once daily) in combination with doxycycline (according to 100 mg 2 times a day) and metronidazole (400 mg 3 times a day) in the treatment of 434 women with clinical signs of uncomplicated PID. The clinical effect at the end of treatment with moxifloxacin monotherapy was observed in 224 of 232 patients (96.6%), and when ciprofloxacin was used in combination with other drugs - in 198 of 202 (98%). The bacteriological effect of moxifloxacin at the end of treatment was 92.6%, the comparison drugs – 88.2%. For infection caused by Chlamydia trachomatis, the use of moxifloxacin ensured the elimination of 95.5% of strains, and the comparison drugs - 85%. For infection caused by N. gonorrhoeae, these figures were 91.7 and 90%, respectively [8].
We conducted our own study to compare two antibacterial therapy regimens in patients with PID: two-component (ciprofloxacin and metronidazole) and monotherapy (moxifloxacin).
The study involved 35 patients who were randomly divided into two groups. The first group included 17 patients who received monotherapy with moxifloxacin (400 mg once a day); 18 patients of the second group received ciprofloxacin and metronidazole according to the standard regimen. The age of patients in both groups was identical and was 22.3 ± 2.3 and 24 ± 2.7 years, respectively. All patients complained of pain in the lower abdomen, a rise in body temperature to 37.9–39.1 °C, and increased discharge from the genital tract. Seven patients from the first group and 6 from the second indicated menstrual dysfunction. These patients were tested for β-chorionic hormone to exclude pregnancy.
A gynecological examination revealed pain on palpation of the uterus and appendages, as well as painful traction on the cervix. The blood test revealed leukocytosis of 12.1 ± 1.7? 109/l – in the first group and 13.2 ± 2.4? 109/l – in the second. In the vaginal discharge, an increase in the number of leukocytes was detected from 40–50 in the field of view to “covering the entire field of view”; coccal flora was determined in 12 and 11 patients of the first and second groups, respectively. Diplococci were found in 7 and 9 patients, respectively. Cultures of vaginal contents revealed Escherichia coli in 7 and 8 patients, respectively, group B Streptococcus in 7 and 8 patients, and Staphylococcus epidermidis in 6 patients in each group.
In patients of the first group, a noticeable improvement in well-being occurred already by the end of the 2nd – 3rd day of treatment. Pain on a 10-point scale decreased in the first group from 9.1 ± 1.3 to 7.0 ± 0.9 on day 2 and to 4.3 ± 1.3 on day 3 of treatment, in the second group - from 9.2 ± 1.2 to 6.9 ± 1.0 and 4.5 ± 1.1, respectively. Almost complete disappearance of pain was observed by the 5th day of treatment in both groups.
The temperature response in the groups during treatment was similar. In the first group, the average body temperature before treatment was 38.2 ± 0.5 °C, on the 3rd day of therapy it decreased to 36.9 ± 0.3 °C; in the second group these indicators were 38.2 ± 0.4 °C and 37.0 ± 0.3 °C, respectively.
The leukocyte level on the 3rd day of treatment dropped to 9.0 ± 0.3? 109/l in the first group and 9.1 ± 0.3? 109/l – in the second; On the 7th day of treatment, leukocytosis was not observed in both groups.
In smears for the degree of purity and flora by the end of treatment (day 14), the number of leukocytes corresponded to 1–2 degrees of purity in all 17 patients of the first group, and in 15 patients in the second (efficacy in the second group - 95.5%).
Diplococci and Escherichia coli were not detected in any patient at the end of treatment. Group B streptococci were cultured in 2 patients of the second group, and staphylococcus epidermidis was also cultured in 2 patients of this group.
Thus, the studies have demonstrated the high effectiveness of moxifloxacin monotherapy, which is not inferior to that of combination therapy with 2-3 antibacterial drugs, and allow, taking into account the wide spectrum of antimicrobial activity, good tolerability and high compliance, to consider moxifloxacin as a drug for initial empirical antibacterial therapy of PID.
Literature
- Padeiskaya E.N., Yakovlev V.P. Antimicrobial drugs of the fluoroquinolone group in clinical practice. M., Dogata, 1998.
- Paton J, Reeves D. Fluoroquinolone antibiotics.Microbiology, parmacokinetics and clinical use. Drugs 1988;36:193–228.
- Dalhoff A. In vitro activities of quinolones. Exp Opin Invest Drugs 1999;8:123–37.
- Appelbaum P, Hunter P. The fluoroquinolone antibacterials: past, present and future perspectives. Int J Antimicrob Agents 2000; 16:5–15.
- MacGowan AP. Moxifloxacin (Bay 12-8039): a new methoxyquinolone antibacterial. Ezp Opin Invest Drugs 1999;8:181–99.
- Siefert HM, Domdey-Bette A, Henniger K, et al. Pharmacokinetics of the 8-meth-oxyquinolone, moxifloxacin: a comparison in humans and other mammalian species. J Antimicrob Chemother 1999;43(suppl. B):69–76.
- Balfour JA, Wiseman LR. Moxifloxacin. Drugs 1999;57:363–73.
- Heystek MJ, Tellarini M, Schmitz H. Efficacy and safety of moxifloxacin vs ciprofloxacin plus doxycycline plus metronidazole for the treatment of uncomplicated pelvic inflammatory disease. . 21st Intern Congress Chemotherapy. Birmingham, 4-7 July, 1999. J Antimicrob Chemother 1999;44 (suppl. A):143.
Until relatively recently, the latest generation of fluoroquinolones—moxifloxacin and levofloxacin—were not seriously considered as treatments for severe infections (with the exception of severe pneumonia). Arguments against their use were the lack of a pronounced effect against some current pathogens (Pseudomonas aeruginosa, anaerobes - levofloxacin), the presence of effective antibiotics among drugs of other classes, and most importantly, the need to accumulate reliable material on the effectiveness of these drugs for “non-respiratory” diseases. However, it is now becoming clear that with increased attention to antimicrobial rotation as a factor in preventing pathogen resistance, these fluoroquinolones may be potentially useful in empirical antibiotic regimens and severe infections.
Fluoroquinolones in general and ciprofloxacin, which has the greatest activity against Pseudomonas aeruginosa in particular, have been successfully used for a long time to treat serious hospital infections [1, 2]. In terms of its antimicrobial spectrum, ciprofloxacin is generally comparable to aminoglycosides, but does not have the inherent nephro- and ototoxicity of the latter. At the same time, it is characterized by low activity against streptococci and no effect against actual anaerobes. Moxifloxacin belongs to the group of extended-spectrum fluoroquinolones. It exhibits increased activity against pneumococci, streptococci and staphylococci, is comparable to ciprofloxacin in its effect on Enterobacteriaceae (although it is inferior to it in its effect on Pseudomonas aeruginosa), but unlike ciprofloxacin it has a high bactericidal index against anaerobes, comparable to the “standard” antianaerobic agent - metronidazole [3]. Its activity against anaerobes does not differ from amoxicillin/clavulanate [4] and even carbapenems. This spectrum of action allows us to consider moxifloxacin as a promising antimicrobial agent for the treatment of mixed (including nosocomial) infections.
The effectiveness of moxifloxacin against P. aeruginosa is less than that of ceftazidime and other antibiotics with targeted “antipseudomonas” activity [5]. In principle, it is also less than that of ciprofloxacin. However, recently, evidence has been accumulating that the minimum inhibitory concentration (MIC) of ciprofloxacin for this pathogen is increasing, which indicates the formation of resistance and predetermines attempts to replace this drug with other antimicrobial agents.
Moxifloxacin inhibits enzymes of the topoisomerase class – DNA gyrase (topoisomerase II) and topoisomerase IV, which are the targets of fluoroquinolones in the bacterial cell and are responsible for changes in the spatial configuration of bacterial DNA IV [6]. DNA gyrase supercoils bacterial DNA, and topoisomerase IV separates daughter chromosomes during replication. The key point in the action of moxifloxacin is the formation of a three-component complex, bacterial DNA - enzyme - quinolone, which prevents the replication of bacterial DNA.
The level of bacterial activity of fluoroquinolones is determined by the degree of their affinity for topoisomerases. To suppress the vital activity of a microbial cell, it is sufficient to inhibit the activity of only one enzyme. This feature explains the fact that for all fluoroquinolone drugs it is possible to distinguish a primary and secondary target of action. The primary target is the enzyme for which a given fluoroquinolone exhibits the greatest affinity. In gram-negative bacteria, fluoroquinolones exhibit the greatest affinity for DNA gyrase, making this enzyme the primary target. In Gram-positive bacteria, the primary target of most drugs in this class is topoisomerase IV [7].
Only moxifloxacin has the same affinity for the two enzymes, which most contributes to the bactericidal effect and prevents the selection of resistant strains [8]. The main mechanism of resistance to fluoroquinolones is a change in the structure of topoisomerase as a result of mutations in the corresponding genes and amino acid substitutions in enzyme molecules. In the vast majority of cases, stability is formed in stages. After the occurrence and selection of mutations in the genes that control the enzyme that is the primary target, the MIC of fluoroquinolones increases 4–8 times. If you continue to administer the drugs, the second enzyme (secondary target) is suppressed, and the MIC increases another 4–8 times.
It is believed that it is the affinity for both topoisomerases that allows moxifloxacin to avoid the formation of stepwise mutations in bacteria and provide an almost constant effect on sensitive strains. This advantage of the drug is relevant for intensive care units, since it is the rapid selection of resistant strains of bacteria that poses the main threat to effective treatment of infection. The reliable effect of the drug is also confirmed by in vitro data. Its activity decreases only slightly with shifts in the pH of the environment in the range of 5.6–8.4 and remains virtually unchanged at inoculum values of 104–106 CFU/ml [9]. This circumstance is extremely important, since during infectious inflammation the pH values of the environment undergo fluctuations over a wide range, and the inoculum tends to rapidly increase.
It is believed that the maximum therapeutic effect of fluoroquinolones and a reduction in the risk of developing microbial resistance to them are achieved when the ratio of peak concentration to MIC is > 8–10, and the ratio of the area under the concentration-time curve (AUC) to MIC should be £ 125 for gram-negative microorganisms and Ћ 30 for gram-positive pathogens [10].
Even more accurate is to take into account the ratio of the AUC of the free fraction of the drug to the MIC. As is known, it is the free fraction of fluoroquinolones, not bound to proteins, that has pharmacological activity. With this approach, the optimal ratio for eliminating microorganisms and preventing microbial resistance is considered to be Ћ 25. For moxifloxacin, this figure is more than 50 (for ciprofloxacin, only 7); when it is reached, the elimination of sensitive microorganisms occurs within 12 hours [11].
Moxifloxacin is registered in Russia under the commercial name Avelox in dosage forms for enteral and intravenous administration. The bioavailability of moxifloxacin when taken orally is close to 100%, i.e. its concentrations after oral and intravenous administration are identical, which determines the same severity of the bactericidal effect in tissues [12]. In addition, it has a clinically significant post-antibiotic effect, which prolongs the effect of the drug up to 24 hours. The convenient mode of administration – once a day and the availability of enteral and parenteral dosage forms makes moxifloxacin one of the drugs of choice for “stepped” treatment tactics – first parenterally, then orally [13].
The results of the clinical use of moxifloxacin indicate its high effectiveness and good tolerability in pneumonia, exacerbation of chronic bronchitis, urogenital infections, and infections of the pelvic organs in women [14]. There are individual reports of the successful use of this drug in surgery, in particular for complicated infectious processes in ENT practice [15]. Particular attention is paid to the issues of “stepwise” use of moxifloxacin, which reduces the cost of treatment. It has been shown that the effectiveness of this method of use in severe pneumonia is comparable to the results of a parenteral course of beta-lactam antibiotics or their combination with antianaerobic agents.
The following features of the pharmacodynamics and pharmacokinetics of moxifloxacin allow us to count on its effectiveness for the prevention and treatment of surgical infections:
- wide spectrum of antibacterial action against gram-positive and gram-negative aerobic and anaerobic bacteria;
- simple and convenient dosing regimen – 400 mg once a day;
- the ability to choose between intravenous or oral administration at the same dose and (if necessary and/or possible) conducting “stepped” therapy;
- favorable safety and tolerability profile.
Let us note that if in outpatient practice the use of all fluoroquinolones in children is still contraindicated, then in the treatment of severe infections in a hospital, this restriction, in our opinion, should not be approached so strictly.
Moxifloxacin was officially included in the recommendations for the management of septic patients with community-acquired surgical infections of the abdominal cavity, as well as with a primary bacterial focus in the kidneys [16]. At the same time, we should not forget about the leading role of this drug in the treatment of severe respiratory tract infections. It is significant that in case of aspiration pneumonia with the formation of a cavity in the lung, moxifloxacin has advantages over many antibiotics and their combinations. Its effect extends to the anaerobic flora that occurs during this process; the drug penetrates well into this cavity [17]. The effectiveness of “stepped” therapy with moxifloxacin (intravenously for 3–4 days, then orally for 4–10 days) and those carried out using a combination therapy method that included amoxicillin/clavulanate and clarithromycin was almost equal (88 and 83%, respectively) [18]. Of course, monotherapy treatment should be considered preferable from a compliance point of view. In addition, it is better tolerated by patients.
Moxifloxacin demonstrates good activity against hospital strains of methicillin-sensitive staphylococci (in some cases against methicillin-resistant strains) and satisfactory activity against enterococci and even Pseudomonas aeruginosa with low MIC90 values [19]. It is the increased activity against gram-positive microorganisms that is considered one of the important advantages of moxifloxacin over previous generations of fluoroquinolones.
In cases of polymicrobial etiology of lung diseases (after artificial ventilation) with higher MIC90 values for moxifloxacin, it is recommended to combine this fluoroquinolone with amikacin [20]. Treatment with moxifloxacin after mechanical ventilation is also justified because after intravenous administration of the drug at a dose of 400 mg during the day, high bactericidal concentrations are established in the lung tissue, which cannot be achieved by administering some beta-lactam antibiotics and vancomycin [21].
Recently, Stenotrophomonus maltophilia has become one of the current causative agents of nosocomial infections. It is found in critically ill patients who have undergone massive antibiotic therapy with broad-spectrum drugs. The resistance of this pathogen is largely determined by the formation of antibiotic efflux. Moxifloxacin has good MIC90 values against S. maltophilia - 0.0625–0.5 μg/ml, surpassing ciprofloxacin in this regard (0.5–2 μg/ml). Suppression of the growth of this bacterium by moxifloxacin after a single dose is 1.5–2 times longer than by ciprofloxacin, and the number of mutated strains formed is several times less [22]. In addition, this problematic pathogen is able to protect itself from beta-lactam antibiotics using the biofilm it forms, which makes it impossible for these drugs to penetrate the microbial cell, which makes it impossible to ensure effective eradication. As recently shown, moxifloxacin, even at low concentrations (equal to half the MIC90), inhibits biofilm growth and provides a reliable bactericidal effect [23].
Moxifloxacin is considered as one of the effective agents for severe infections of the skin and soft tissues [24]. It is of particular relevance in patients with concomitant diabetes mellitus, with lesions of the skin and underlying structures, when there are polymicrobial associations of gram-positive aerobic and anaerobic flora.
It should be noted that there are no generic drugs of moxifloxacin on the domestic pharmaceutical market (contrast with “ciprofloxacins”), which guarantees all the above-described characteristics of action when using the original drug Avelox.
In conclusion, I would like to emphasize the authors’ understanding of the importance of the position according to which practical recommendations, in particular for the use of moxifloxacin for sepsis and other severe infections, should be based on the results of large international studies assessing the effectiveness and tolerability of the drug. However, given the great importance of the problem of treating these infections, the article makes an attempt, even before obtaining data from this type of research, to draw the attention of clinicians to the potential opportunities inherent in moxifloxacin, a modern antibacterial drug with a wide spectrum of action. Discovering these possibilities seems to be an urgent task for the specialists themselves, who in their daily work are faced with the problem of treating severe infections.






![Table 1. Comparison of the results of treatment with Tribestan for men with oligoasthenozoospermia [7] with mod.](https://ms-pi.ru/wp-content/uploads/tablica-1-sravnenie-rezultatov-lecheniya-tribestanom-muzhchin-s-oligoastenozoospermiej-7-330x140.jpg)