Probably each of us has heard about the placenta, but usually even pregnant women have a very general idea of its purpose and function. Let's talk about this amazing organ in more detail.
The placenta connects mother and child, it is needed to nourish the baby, after birth it will no longer be there - as a rule, this is the only knowledge about the placenta at the beginning of pregnancy. As the pregnancy progresses and after undergoing an ultrasound, the expectant mother learns the following about the placenta: “the placenta is located high (or low)”, “its degree of maturity is now such and such.” Then the placenta, like the baby, is born. True, this event is no longer so significant for many mothers against the backdrop of the arrival of the long-awaited baby.
The placenta does not appear immediately. It is formed from the chorion - the embryonic membranes of the fetus. The chorion looks like many elongated outgrowths of the membrane surrounding the unborn child, which penetrate deep into the wall of the uterus. As pregnancy progresses, the outgrowths of the chorion increase in size and turn into the placenta; it is finally formed by the end of the first trimester of pregnancy.
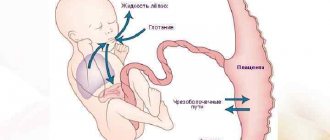
The new organ has the appearance of a disk, or cake (that’s exactly what “cake” is translated from Latin as the word placenta). One side of the placenta is attached to the uterus, and the other “looks” towards the baby. It is connected to the fetus by the umbilical cord. There are two arteries and one vein running inside the umbilical cord. Arteries carry blood from the fetus to the placenta, and veins carry nutrients and oxygen from the placenta to the baby. The umbilical cord grows with the child and by the end of pregnancy its length is on average 50–55 cm.
What is placenta
During the development of the embryo, a chorion is formed on its outer shell - specific outgrowths. It gradually grows into the woman’s uterus and increases in size. As a result, the so-called "children's place"
The process comes to an end at 12-16 weeks after conception. At this point, the organ becomes flat, resembling a disk in shape (placenta in Latin). The connection between the mother and child is provided by the umbilical cord. It has a length of 5-55 cm, and functions as follows:
- the artery delivers nutrients and oxygen;
- the vein is necessary to remove processed substances.
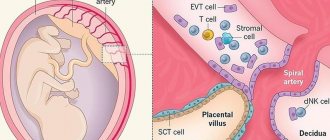
The formed placenta consists of decidual tissues, embryoblast and trophoblast, and the main element is called the villous tree. This organ is designed to prevent Rh conflict. Its thickness is approximately 3.5 cm, and its diameter is 20 cm; weight – about 600 g.
The development of the placenta until the 4th month occurs faster than the growth rate of the embryo. At this point, the villi and blood vessels are completely formed. If a child dies at any stage, degenerative phenomena increase.
The placenta consists of two sides:
- rough maternal surface, formed from the basal component of the decidural layer, facing the uterus;
- the fruit side, covered with the amniotic layer, turned towards the embryo.
If a woman is pregnant with twins, there are three options:
- Dizygotic twins implanted separately. The placenta is divided into two parts, each of which has its own membranes and blood vessels.
- Dichorionic twins separated from each other by a septum. The main part of nutrition comes from amniotic fluid, and there are practically no blood vessels in the placenta membrane. In this case, pregnancy management under the supervision of a specialist in our center is mandatory, since the risk of transfusion syndrome is high.
- Monoamniotic monochorionic twins not separated by a septum.
The placenta begins to form from conception. Starting from the 2nd week of pregnancy, its growth is activated, by the 13th the structure is fully developed, and maximum activity is observed by the 18th week. Complete cessation of growth and changes occurs only after delivery.
What are the dangers of low placental location?
This pathology is considered dangerous to the life and health of both the child and his mother. The greatest risks include:
- Miscarriage or premature birth. The likelihood of this outcome is due to the fact that with placental insufficiency the uterus experiences higher loads than during a normal pregnancy. Any physical stress and even mental stress can cause intense uterine contractions, expelling the fetus. Moreover, the likelihood of this remains throughout the entire pregnancy.
- Fetal presentation. If the placenta has formed low in early pregnancy, the risk of fetal malposition increases by 50%. Developing in the mother's belly, the unborn child strives to take a position so that its head is in contact with anything as little as possible - including the “baby place”. Transverse or breech presentation of the fetus makes natural childbirth impossible and is a pathological condition that threatens both itself and its mother.
- Fetal hypoxia. With inferior placenta previa, the blood supply to the embryo with nutrients and oxygen deteriorates. Chronic and acute hypoxia causes irreversible changes in the child’s brain, delays his intrauterine development, and during childbirth can lead to his death.
- Uterine bleeding. This complication threatens a woman with placental insufficiency throughout pregnancy. This risk is especially great in the later stages, when the fetus becomes quite large and puts more pressure on the walls of the uterus, increasing the likelihood of placental abruption from the endometrium. Mild but regular bleeding provokes the development of anemia in the mother, which, in turn, is one of the causes of chronic embryonic hypoxia. With severe placental abruption, extensive hemorrhage may develop with hemorrhagic shock, fatal for both the woman and her child.
All of these complications make placenta previa a dangerous pathology. Therefore, when it is detected, a woman is at risk. Depending on the type of pathology, doctors develop a special treatment strategy that will save the life of both the mother and her child.
Take the first step
make an appointment with a doctor!
Monitoring the development of the placenta
Changes occurring in the placenta are monitored using ultrasound. To do this, use the classification of organ maturity:
- Stage 0 – up to the 30th week;
- Stage 1 – from 30th to 34th;
- Stage 2 – from 34th to 37th;
- Stage 3 – from 37th to 39th;
- Stage 4 – before delivery.
By monitoring the rate of organ maturation, our doctors can promptly determine the pathology:
- too early development indicates disturbances in the placental blood supply (if the woman does not have a genetic predisposition to this phenomenon);
- delayed maturation does not affect the child’s condition and does not pose a threat to him.
Research is carried out not only using ultrasound, but also by determining the level of lactogen, a hormone that indicates normal maturation. Normally, it should be at least 4 mcg/ml.
Pregnancy management in Nizhny Novgorod also includes daily monitoring of estrogen concentrations. A low level may indicate renal failure of the expectant mother, severe liver pathologies, or be a consequence of taking antibiotics.
Sources
- Tiwari D., Das CR., Sultana R., Kashyap N., Islam M., Bose PD., Saikia AK., Bose S. Increased homocysteine mediated oxidative stress as a key determinant of hepatitis E virus (HEV) infected pregnancy complication and outcome: A study from Northeast India. // Infect Genet Evol - 2021 - Vol - NNULL - p.104882; PMID:33905889
- Salmanian B., Belfort MA., Shamshirsaz A.A. The risk of placenta accreta spectrum in women with in vitro fertilization in different populations. // Am J Obstet Gynecol - 2021 - Vol - NNULL - p.; PMID:33905744
- Olmos-Ortiz A., Olivares-Huerta A., García-Quiroz J., Zariñán T., Chavira R., Zaga-Clavellina V., Avila E., Halhali A., Durand M., Larrea F., Díaz L. Placentas associated with female neonates from pregnancies complicated by urinary-tract infections have higher cAMP content and cytokines expression than males. // Am J Reprod Immunol - 2021 - Vol - NNULL - p.e13434; PMID:33905581
- Tandl V., Hoch D., Bandres-Meriz J., Nikodijevic S., Desoye G., Majali-Martinez A. Different regulation of IRE1α and eIF2α pathways by oxygen and insulin in ACH-3P trophoblast model. // Reproduction - 2021 - Vol - NNULL - p.; PMID:33904834
- Ji S., Gumina D., McPeak K., Moldovan R., Post MD., Su EJ. Human placental villous stromal extracellular matrix regulates fetoplacental angiogenesis in severe fetal growth restriction. // Clin Sci (Lond) - 2021 - Vol - NNULL - p.; PMID:33904582
- Shmeleva EV., Colucci F. Maternal natural killer cells at the intersection between reproduction and mucosal immunity. // Mucosal Immunol - 2021 - Vol - NNULL - p.; PMID:33903735
- Moreno-Sepulveda J., Espinós JJ., Checa MA. Lower risk of adverse perinatal outcomes in natural versus artificial frozen-thawed embryo transfer cycles: a systematic review and meta-analysis. // Reprod Biomed Online - 2021 - Vol - NNULL - p.; PMID:33903031
- Owen MD., Cassidy AL., Weeks AD. Why are women still dying from obstetric hemorrhage? A narrative review of perspectives from high and low resource settings. // Int J Obstet Anesth - 2021 - Vol - NNULL - p.102982; PMID:33903002
- Liu CN., Yu FB., Xu YZ., Li JS., Guan ZH., Sun MN., Liu CA., He F., Chen DJ. Prevalence and risk factors of severe postpartum hemorrhage: a retrospective cohort study. // BMC Pregnancy Childbirth - 2021 - Vol21 - N1 - p.332; PMID:33902475
- Munoz JL., Kimura AM., Xenakis E., Jenkins DH., Braverman MA., Ramsey PS., Ireland KE. Whole blood transfusion reduces overall component transfusion in cases of placenta accreta spectrum: a pilot program. // J Matern Fetal Neonatal Med - 2021 - Vol - NNULL - p.1-6; PMID:33902384
Possible pathologies
The most common violations:
- discrepancy between the pace of development of the placenta and the baby;
- the appearance of blood clots that obstruct blood flow;
- incorrect location of the organ;
- excessive thickening;
- heart attack - cessation of blood flow through the arteries;
- various inflammations, tumors.
The reasons for these phenomena may be:
- toxicosis;
- diabetes;
- atherosclerosis;
- infectious phenomena in the mother's body;
- Rhesus conflict;
- excessive or insufficient weight of a woman;
- emotional stress;
- bad habits;
- woman's age over 35 years.
It is important that the expectant mother monitors her own well-being throughout the entire period of carrying the child. The appearance of any unusual symptoms - vaginal discharge, pain, cramps, increased swelling should be a signal for urgent contact to our center.
Pathogenesis
The second planned ultrasound during pregnancy (20-24th week) in most cases is not indicative of diagnosing the corresponding problem. For the first time, it is possible to detect early maturation of an organ mainly at 27-28 weeks, when the degree of development of the child’s place changes from 0 to 1.
Normally, the structure of the placenta is homogeneous, without undulations. At the first stage of maturity, the body of the organ becomes thicker. Ultrasound shows zones of hyperechogenicity. The first irregularities appear on the chorionic plate.
When exposed to negative factors, a premature transition of the placenta to the second degree of maturity occurs. The number of zones of hyperechogenicity increases, small inclusions appear, and irregularities on the chorionic plate deepen.
The third degree is characterized by the lobar structure of the placenta, blood flow through the vessels to the fetus is reduced, and calcifications can form in the parenchyma of the organ. The described changes can be diagnosed when the third ultrasound is performed during pregnancy (32-34 weeks).
Pregnant woman
The body of a pregnant woman continues to actively prepare for the birth of a baby, the content of estrogen rapidly increases, and the level of progesterone decreases significantly. Changes in hormonal levels help soften the tissues of the birth canal and cervix. Throughout pregnancy, the lumen of the cervical canal is closed by a plug of thick mucus, which protects the baby from infection, and the uterine cavity protects against the penetration of microorganisms hazardous to health. In the last weeks of pregnancy, the consistency of the mucus changes, it becomes more liquid and begins to gradually flow out. In some women, the mucus disappears gradually, while in other women in labor it comes off simultaneously. The discharge resembles colorless egg white in its consistency and appearance. Sometimes the mucus is pinkish, brown or yellow. The removal of the plug is painless; the woman may experience a slight feeling of discomfort in the lower abdomen. The removal of the plug may be signaled by more abundant vaginal discharge than during the entire pregnancy.
A woman should carefully monitor the color and volume of discharge, since too much colorless discharge may indicate not only the passage of the plug, but also be one of the symptoms of leakage of amniotic fluid. Indicator pads and amniotests or test strips will help determine the cause of the discharge. The pads are sold in many pharmacies and can be easily used at home. If leakage of amniotic fluid is confirmed, you should immediately consult a doctor.
After the mucus plug comes off, you should avoid visiting the pool and swimming in open water, as the risk of infection for the child increases significantly. It is also necessary to exclude sexual contact.
Causes of detachment
The exact reasons are not known today. Basically, there are several factors that provoke complications:
- mechanical factor
- bleeding disorder
- vasculopathy
Causes:
- many births with little time between them, which causes endometrial degeneration)
- post-term pregnancy
- compression of the inferior vena cava, which changes blood pressure
- sudden surges in blood pressure due to stress and other reasons
- high blood pressure as a consequence of vascular diseases
- endocrine disorders, mainly diabetes mellitus
- age (from 30 years of age the risk is higher)
- hereditary bleeding disorders
- autoimmune diseases, such as SLE
- tearing off an additional piece of placenta during pushing
- gestosis
- premature “aging” of a child’s seat
- congenital malformations of the uterus
- operations or cesarean section, as a result of which scar tissue has formed that does not “hold” the placenta well
- infectious-allergic vasculitis
- blunt abdominal trauma
- taking drugs, drinking alcohol, smoking and other habits harmful to the organisms of mother and child
- incorrect location of the placenta (too low attachment or presentation)
- blood transfusion or infusion of colloidal solutions, which leads to vascular-allergic reactions that cause placental abruption
Causes of detachment during childbirth:
- rapid or rapid labor
- the birth of the first fetus when carrying several children (the baby “pulls” the placenta behind him
- rapid decrease in pressure inside the uterus as water flows out
- anomalies of ancestral forces
- delayed opening of the amniotic sac
- short umbilical cord length
- oxytocin for labor stimulation
- obstetric manipulations to help the baby be born