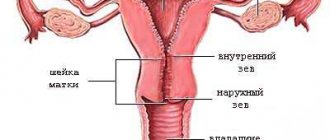
Uterine rupture (UR) during childbirth is a complication that can lead to massive bleeding, being the most dramatic cause of maternal and perinatal mortality. Violation of the integrity of the wall of the unoperated uterus is considered one of the indicators of improper management of labor and poor quality obstetric care in general.
In Russia R.M. According to pathogenesis, they are divided into mechanical, histopathic, mechano-histopathic and violent [1]. In foreign literature, the dominant cause of RM was considered to be the presence of a scar on the uterus after previous interventions. As a conditional analogue of mechanical RM, one can consider the rupture of an unoperated (unscarred or unattached uterus), and histopathic - a previously operated uterus (scarred uterus). There is no complete identity between the concepts of “histopathic uterine rupture” and “rupture of a previously operated uterus,” since damage to the myometrium may be associated with other causes, i.e., the absence of a scar on the uterus does not guarantee the impossibility of its rupture.
According to WHO, the overall incidence of RM is 5.3 per 10,000 births, rupture of the operated uterus is 100 per 10,000, and rupture of the unoperated uterus is 0.6 per 10,000 births (Table 1).
Table 1. Frequency of uterine rupture and accompanying maternal and perinatal mortality, according to various authors
According to Rosstat in the Russian Federation, the incidence of RM in 2014 was 1.4 per 10,000 births. In Moscow, according to the organizational and methodological department of the Department of Health (DZ) of Moscow, the frequency of RM for the past 2014 was 2.7 per 10,000 births. According to the Center for Family Planning and Reproduction D.Z. Moscow, the overall incidence of uterine rupture was 3 per 10,000 births, and rupture of an unoperated uterus was 0.9 per 10,000 births.
Maternal mortality from uterine rupture in Russia, according to Rosstat, in 2013 was 0.42 per 100,000 live births.
Presented in table. 1 data show wide variability in the incidence of rupture of the operated uterus from 5 per 10,000 in Saudi Arabia to 740 per 10,000 births in India. Unoperated uterine rupture represents a relatively low rate of 0.3–0.7 per 10,000 births or 11.5–13% of all RMs.
According to some authors [10], decreased interest in managing vaginal delivery in patients with a uterine scar after cesarean section may lead to a change in the ratio and a relative increase in the number of ruptures of the unoperated uterus.
Currently, rupture of the unoperated uterus occurs more often in countries with less developed economies, which are characterized by high birth rates and a lack of emergency obstetric care. According to authors from Nigeria, 94% of patients with RM had no scar on the uterus; in India, such patients also made up the majority - 77.4% [11, 12]. Such ruptures lead to more severe complications in the mother and fetus (compared to uterine ruptures along the scar) and can be a direct cause of maternal mortality [2, 6, 9].
Rupture of the unoperated uterus often occurs due to overstretching of the myometrium of the lower uterine segment due to obstruction of the fetus being born (mechanical factor). Sometimes trauma to the uterus can be associated with obstetric manipulations: internal rotation and extraction of the fetus by the pelvic end, application of abdominal obstetric forceps with a high-standing head. In the literature, congenital or acquired inferiority of the myometrium, disorders of the collagen matrix and abnormal architecture of the uterine cavity (bicornuate and complete duplication of the uterus, uterus with a blind uterine horn) are considered as putative causes of RM [13, 14].
In the 35th chapter of Williams Obstetrics, devoted to obstetric hemorrhage, uterine curettage is mentioned first among the provoking moments [15].
Risk factors for rupture of the unoperated uterus during childbirth include a large number of births and overstretching of the myometrium during multiple pregnancies. Drug induction and stimulation of labor with mifepristone, misoprostol, and oxytocin are described as an iatrogenic cause of uterine rupture [16].
The purpose of the study was to use an in-depth retrospective analysis of observations of patients with an unoperated uterus who experienced RM during childbirth, to identify the causes of RM and offer recommendations to reduce their frequency; confirm the feasibility of performing organ-preserving operations for uterine ruptures during childbirth.
Risk factors and main causes
There are several theories that try to explain the origin of the injury. The creator of one of them is Bandle, who explained the pathology by mechanical reasons. He described this process as excessive distension of the lower part of the uterus due to the large size of the fetus and the narrow pelvis of the mother. But this theory cannot explain why trauma occurs when the child is small.
This theory was supplemented by the research of Ya. F. Verbov, who believed that pathologically altered tissues are necessary for the formation of a wall defect. This disease occurs against the background of chronic endometritis, after multiple abortions and curettage, endometriosis or scar changes.
Currently, the causes of uterine rupture have expanded significantly. It is believed that histological changes in the wall predispose to cavity formation, and this process is triggered by mechanical or violent action.
Histological causes include the following:
- Scars after operations (caesarean section, plastic surgery of congenital defects, removal of myomatous node, perforation);
- chronic inflammatory process;
- tight fit of the placenta;
- dystrophic changes after frequent curettage;
- Infantilism and birth defects;
- biochemical changes during prolonged labor.
The defect can occur not only at the site of a scar or altered wall, but the injury occurs around the prostate horn. In this case, the rupture occurs at 16-20 weeks of pregnancy, provided that the fetus is attached to the area of the prostate horn. Clinical manifestations of the pathology resemble tubular abortion.
Mechanical causes combine cases that cause discrepancies in the size of the fetus and the female pelvis:
- Clinically or anatomically narrow pelvis;
- hydrocephalus;
- Large fruit;
- Frontal or posterior presentation;
- incorrect head position;
- transverse or oblique position of the fetus;
- myometrial tumors;
- birth canal with cicatricial changes;
- unevenness or deformation of the bones in the pelvis.
The occurrence of this complication can be caused by sudden actions resulting from improper use of surgical or obstetric manipulations:
- obstetric forceps;
- vacuum extraction of the fetus;
- Kristeller Extraction;
- extraction of the fetus through the end of the pelvis;
- internal rotation;
- Removal of the head according to Morisseau-Levre;
- release the retracted lever when presenting the lock;
- fetal demolition operations.
Causes of violence include accidental injuries that may occur outside of childbirth.
Sources
- Turan OM., Driscoll C., Cetinkaya-Demir B., Gabbay-Benziv R., Turan S., Kopelman JN., Harman C. Prolonged early antenatal indomethacin exposure is safe for fetus and neonate. // J Matern Fetal Neonatal Med - 2021 - Vol34 - N2 - p.167-176; PMID:30905227
- Wallstrom T., Bjorklund J., Frykman J., Jarnbert-Pettersson H., Akerud H., Darj E., Gemzell-Danielsson K., Wiberg-Itzel E. Induction of labor after one previous Cesarean section in women with an unfavorable cervix: A retrospective cohort study. // PLoS One - 2021 - Vol13 - N7 - p.e0200024; PMID:29965989
- Vogel JP., Osoti AO., Kelly AJ., Livio S., Norman JE., Alfirevic Z. Pharmacological and mechanical interventions for labor induction in outpatient settings. // Cochrane Database Syst Rev - 2021 - Vol9 - NNULL - p.CD007701; PMID:28901007
- Sarreau M., Leufflen L., Monceau E., Tariel D., Villemonteix P., Morel O., Pierre F. . // J Gynecol Obstet Biol Reprod (Paris) - 2014 - Vol43 - N1 - p.46-55; PMID:23972769
- Epee-Bekima M., Overton C. Diagnosis and treatment of ectopic pregnancy. // Practitioner - 2013 - Vol257 - N1759 - p.15-7, 2; PMID:23634634
- Charach R., Sheiner E. Risk factors for peripartum hysterectomy following uterine rupture. // J Matern Fetal Neonatal Med - 2013 - Vol26 - N12 - p.1196-200; PMID:23356737
Features of the mechanism
One of the common causes of this complication is an inconsistent method of delivery. This condition develops as a result of stimulation of labor, for which there is no indication, or due to the individual characteristics of the body (more about the indications and contraindications for stimulation of labor). These include imbalances in the autonomic nervous system with a predominant influence of the parasympathetic department. Such disorders occur during childbirth against the background of increased myometrial tone. Stimulation contractions become more frequent and do not decrease.
The pressure in the uterus changes rapidly, and instead of the muscle fibers gradually spreading, they quickly stretch. In the presence of pathological changes, a crack forms.
A fracture that occurs primarily due to mechanical obstruction occurs by a different mechanism. The fetus cannot move along the birth canal, so the myometrium moves to the bottom, and the lower segment is stretched. The baby's head presses the cervix against the pelvic bones, causing hyperemia and swelling. The minimum thickness of the uterine wall with the probability of rupture in this condition is several millimeters. When the fabric no longer stretches, the following process begins:
- Rupture of the vessel wall;
- formation of hematomas;
- formation of cracks;
- Eventually the uterus becomes incomplete or completely ruptured.
The mechanism of violent rupture during childbirth is associated with an additional impact on the uterus, which is already in a critical condition. Excessive stretching of the lower segment in a clinically narrow pelvis and pressure on the fundus of the uterus cause increased tissue tension and a defect.
It is generally accepted that healthy myometrium is not prone to cracking. If a healthy woman experiences a discrepancy between the size of the fetal head and the birth canal, labor is usually stopped. Pathologically changed tissues after abortion, curettage and inflammation are characterized by the presence of connective tissue and impaired blood supply. Histological changes occur at the cellular level, so sometimes they cannot be noticed during examination.
This modified wall is capable of stretching during pregnancy and can withstand contractions during normal childbirth, but cannot withstand additional load.
After each operation on the internal genital organs, which was accompanied by cutting the wall, some of the muscle cells at the edge of the wound are lost. During healing, the wound surface is filled with new myocytes and connective tissue, but the structure is not restored. If not enough time has passed from the formation of the scar to the onset of pregnancy, imperfection of its tissue can lead to rupture of the uterus along the length of the scar.
Options for birth trauma
There are several different variants of uterine rupture, which have become the basis for different approaches to the classification of this pathological condition. Based on the characteristics of the formation mechanism, they distinguish:
- Spontaneous - occurs without the influence of external factors as a result of pathological changes in the wall and disturbances in professional activity;
- Violent - when performing manipulations and obstetric operations.
The stage of advancement is determined by the clinical course:
- threatening;
- in the early stages;
- accomplished.
The nature of the damage may vary:
- A rupture is a small break in a piece of the uterine wall.
- An incomplete fracture consists of the appearance of a defect only in the mucous membrane and muscles. The outer layer of the serous membrane remains intact. This type of injury is more common on the lateral surfaces of the lower segment or along the rib of the uterus. The injury is accompanied by internal bleeding with the formation of a huge hematoma between the ligaments of the uterus.
- Complete loss is the most common. It is characterized by damage to all layers of masonry.
Uterine rupture: Fig. 1 - through the scar after cesarean section; Dig. 2 - incomplete, in the lower segment with the formation of a hematoma
Most often, the crack occurs in the lower segment. This area is most rarely seen during childbirth. But another arrangement is possible:
- at the bottom of the uterus;
- along the side walls;
- in organism;
- detachment of the uterus from the vaginal vault.
Uterine rupture is a condition associated with the period of labor of the fetus. Therefore, it is impossible to consider the causes of rupture outside pregnancy from this point of view. Violation of the integrity of the wall in non-pregnant women is more often called perforation.
results
In group 1 (n=35) with mechanical and/or mechano-histopathic uterine rupture, the average age of those examined was 31.4±5.4 years (from 22 to 44 years), 7 (20) were primiparous, and multiparous - 28 (80%): 17 had a second birth, 7 had a third, 2 had a fourth, 1 had a fifth, 1 had a sixth. 24 (68.6%) women had a history of abortion or curettage of the walls of the uterine cavity due to endometrial pathology. Complicated course of previous births was observed in 11 (31.4%) patients: large fetus - in 5, large fetus in combination with postpartum endometritis - in 1, twin births - in 1, perinatal death for unknown reasons - in 3, cervical ruptures - at 1.
All births accompanied by uterine rupture occurred at term. 19 (54.3%) women in group 1 gave birth spontaneously, 16 (45.7%) were delivered by cesarean section.
Among 19 women who gave birth through the vagina, induction of labor by intracervical or intravenous administration of prostaglandins was carried out in 2, labor activation with oxytocin - in 4.
Large babies were born to 17 of 19 patients. The weight of the newborn was 4000-4200 g in 13 patients, 4350 g in 1, 4500 g in 1, 4650 g in 1, 5028 g in 1.
The most common clinical sign of uterine rupture during childbirth [1, 17]—impaired fetal cardiac activity—was detected in 4 (11.4%) patients. The birth histories did not show any symptoms of hyperextension of the lower uterine segment. It can be assumed that the doctors leading the birth did not pay attention to them.
All 19 patients underwent manual examination of the walls of the uterine cavity for the following indications: hypotonic bleeding in the early postpartum period - in 10, control (a large number of births in history) - in 4, suspected uterine rupture - in 2, cervical rupture of the third degree - in in 1 patient, partial tight placenta in 1 patient, giant fetus in 1 patient.
All 19 parturient women subsequently underwent transection, the indications for which were: RM detected during manual examination in 12 patients, hypotonic bleeding that was not amenable to conservative therapy in 3, intra-abdominal bleeding in 3, hematoma in the parametrium identified by ultrasound, - in 1. In 5 out of 19 postpartum women, cervical ruptures of II-III degree, passing to the lower segment, were diagnosed; all 5 patients were multiparous.
Intraoperatively, in 8 patients, a rupture was found in the area of the lateral edge (margo uteri sinister, dexter) of the “rib” of the lower uterine segment of the uterus (more often left than right), in 5 the rupture extended from the cervix to the lower segment, in 4 it was localized in the lower segment under the vesical - uterine fold and in 2 - along the posterior wall of the uterine body.
In all 5 patients in whom the cervical rupture continued into a uterine rupture, and in 6 out of 8 women with a uterine rupture in the area of the “rib” of the lower segment of the uterus, the weight of the newborns ranged from 4000 to 4500 g. The children were born in satisfactory condition or with mild asphyxia , which suggests PM at the height of the last attempt.
Rupture of the lower uterine segment was typical for multiparas with newborns weighing from 4050 to 4650 g. Two children were born with moderate asphyxia (perhaps there were histopathic changes in the myometrium associated with the birth of a child weighing 4700 g in previous births in one patient and the fourth present second childbirth).
RM along the posterior wall in the lower third was in a primiparous woman with a baby weighing 4200 g after induction of labor with prostaglandins and in the middle third in a multiparous woman with a newborn weighing 5028 g. It is difficult to explain the cause of rupture of the posterior wall of the uterus in the second patient; perhaps the history of the rupture was significant abortion. The children were born in satisfactory condition.
In one primiparous patient with a large fetus, intraoperatively, in addition to a rupture in the “rib” area of the lower segment of the uterus, a rupture of the spleen was diagnosed, probably of a violent nature (iatrogenic rupture). In 2 patients, the body weight of the children was 2960 and 3560 g, both women had a uniformly narrowed pelvis of the first degree, the duration of labor was 12 hours 50 minutes and 8 hours 50 minutes, respectively. In one patient, labor activation with oxytocin was used, in the second, labor induction with prostaglandins was additionally performed. A child weighing 2960 g died intrapartum, weighing 3560 g was born with moderate asphyxia, which may have been determined by exceeding the permissible doses of oxytocin and the duration of its administration.
Emergency caesarean section was performed on 16 patients, 7 of them were operated on for a clinically narrow pelvis. The weight of newborns in 3 patients was 4400, 5050 and 5420 g. In 4 patients, the weight of children was 2880-3850 g, 3 of them had a uniformly narrowed pelvis of I-II degree. One woman in labor developed a clinically narrow pelvis as a result of frontal insertion of a fetus weighing 3000 g. Not a single patient in the history of childbirth had symptoms of hyperextension of the lower segment of the uterus.
RM was localized along the lateral edge in the lower segment in 5 women. In one patient with the fifth birth, RM occurred along the posterior wall of the lower segment and intrapartum death of the fetus weighing 5420 g. One primigravida with premature rupture of amniotic fluid was induced with intravenous prostaglandins. This patient was of average height and had normal pelvimetry findings and was delivered by cesarean section due to symptoms of a clinically narrow pelvis. An examination of the birth canal revealed a third degree cervical rupture, which continued into a rupture of the lower segment of the uterus. The child's body weight is 3520 g.
The remaining 9 patients were delivered due to the onset of uterine rupture, which was incorrectly interpreted as acute fetal hypoxia and premature abruption of a normally located placenta. In 7 of 9 patients, RM was localized in the lower segment, all children were large, 2 children died intrapartum, 3 were born with severe asphyxia and one with moderate asphyxia.
In 2 multiparous women, uterine rupture occurred along the posterior wall of the uterine body; children weighing 3300 and 4000 g were born with mild asphyxia. Both patients had a history of pregnancy loss, which could have caused injury to the uterus of an atypical location.
The scope of the operation for mechanical RM consisted of suturing the uterine wall defect, which was performed in 32 (91.4%) patients. Hysterectomy after unsuccessful ligation of the internal iliac arteries was performed in 3 (8.6%). Ligation of the internal iliac arteries as additional hemostasis during organ-preserving operations was used in 20 (57.1%) patients, ligation of the uterine arteries on both sides - in 2 (5.6%), embolization of the uterine arteries - in 1 (2.8%) . Total blood loss was 700–2000 ml in 14 (40%), 2001–3000 ml in 13 (37.3%), 3001–4000 ml in 6 (17.1%), 4500 ml in 2 (5, 6%).
Reinfusion of autoerythrocytes with the Cell-Saver device was used in 20 (57.1%) patients. The volume of reinfusion varied from 200 to 2098 ml. Transfusion of donor red blood cells with a volume of 233-1565 ml was performed in 25 (71.4%) women.
The length of hospital stay varied from 7 to 24 days. In 5 (14.3%) patients the postoperative period proceeded with complications. Endometritis was diagnosed in 1 patient, hematoma of a postoperative wound on the uterus - in 1, acute pyelonephritis - in 1, thrombophlebitis of the radial vein - in 1. Conservative therapy was carried out with a positive effect. No maternal mortality was recorded.
Group 2 – histopathic RM (n=51). The average age of the patients was 31.2±5 years (from 21 to 45 years). Primiparous and multiparous patients were distributed with the same frequency - 23 (45.1%) and 28 (54.9%), respectively. There were 16 expected second births, 8 thirds, 2 fourths, 1 fifth, and 1 sixth. Every fifth patient had a premature birth (28-36 weeks).
30 (58.8%) patients had a history of abortion or diagnostic uterine curettage, 8 (15.7%) had laparoscopic or laparotomic surgical interventions (cystectomy, adhesiolysis, coagulation of endometrioid heterotopias), with which it is difficult to associate probable RM with the onset of pregnancy. One patient was diagnosed with complete duplication of the uterus.
Among 28 multiparous women, a complicated course of previous births was noted in 8: large fetus - in 2, postpartum endometritis - in 1, twin births - in 1, perinatal death - in 2, obstetric forceps, birth trauma of the child - in 1, hypotonic bleeding - in 1.
32 (62.7%) women gave birth through the vaginal canal, 19 (37.3%) were delivered by cesarean section.
Among 32 women who gave birth through the vagina, induction of labor by intracervical administration of prostaglandins was attempted in 3, by amniotomy in 2, and labor activation with oxytocin in 7.
The weight of children at birth was less than 3000 g in 6 (18.8%) patients, 3001-3500 g in 20 (62.5%), 3501-3750 g in 4 (12.5%). In 2 (6.2%) multiparous patients (second and third upcoming births), the weight of the children was 3920-3930 g.
In histopathic uterine rupture, the leading clinical sign was impaired fetal cardiac activity in 9 (28.1%) women.
In 29 of 32 patients, a manual examination of the walls of the uterine cavity was performed for hypotonic bleeding in the early postpartum period - in 11, cervical rupture of the third degree - in 8, partial or complete tight attachment of the placenta - in 6, placental defect - in 4 patients. During manual examination of the uterus, a defect of the uterine wall was found in 21, and not found in 8.
All 32 patients subsequently underwent laparotomy, the indication for which was RM identified during manual examination in 21 patients, intra-abdominal bleeding in 6, hypotonic bleeding not amenable to conservative therapy in 4, hematoma in the parametrium diagnosed by ultrasound, - at 1.
In all patients, RM was confirmed intraoperatively. The II-III degree cervical rupture continued into a rupture of the lower uterine segment in 17, was localized isolated in the lower segment in 10, along the posterior wall in 4, in the fundus of the uterus in 1.
Complete RM was detected in 15 women, incomplete – in 17.
Among 17 patients with grade II-III cervical rupture that lasted in the Republic of Moldova, 11 were multiparous. A large number of births (3rd-6th births) were observed in 6. Of the 6 primiparas, all underwent labor activation with oxytocin. 11 children were born in a state of mild asphyxia; uterine rupture probably occurred at the end of the second stage of labor.
When the rupture was localized in the lower segment of the uterus, 7 out of 10 patients were multiparous, 2 with a large number of births. In 2 out of 3 primiparas, no risk factors for RM were identified. All children, except one, were born in a satisfactory condition or a state of mild asphyxia.
RM along the posterior wall was typical for patients with a history of 2–4 abortions. In 3 out of 4 children, the Apgar score at birth was 7 or 8 points.
In one primigravida with an uncomplicated history, RM was localized in the fundus.
Caesarean section was performed in 19 patients, among whom in 8 the indication for surgery was a diagnosis of premature abruption of a normally located placenta, bleeding, in 7 - acute fetal hypoxia, in 3 - uterine rupture and in 1 - weakness of labor. All of these clinical manifestations could, with a certain degree of probability, indicate the presence of symptoms of threatening or incipient RM of the histopathic type, although there was no scar on the uterus in these patients.
The weight of children at birth was less than 3000 g in 9 patients, 3001-3500 g in 7, 3501-3850 g in 3.
When opening the abdominal cavity, a rupture in the lower uterine segment was found in 12, in the fundus in 3, along the posterior wall in 2, a cervical rupture of the third degree, extending into a rupture of the rib of the lower segment, in 2.
Complete RM was detected in 12, incomplete - in 7.
When the rupture was localized in the lower segment of the uterus, primiparas and multiparas were distributed with the same frequency. There were 3 women with high parity; in 2 of them, previous births ended in the birth of large children weighing 4100-5000 g. The rest of the multiparous women had from 3 to 6 abortions. Of the 6 primigravidas, 3 were primigravidas; no risk factors could be identified in them; the rest had 1-2 abortions.
All patients with RM in the fundus had a history of abortions without indication of perforation. A third degree cervical rupture, which extended into a rupture of the lateral edge of the uterus, occurred in one patient with a large number of births and in one primigravida who underwent prolonged labor activation with oxytocin due to primary weakness of labor. The reason for the rupture of the posterior wall of the uterine body, which occurred in 2 primigravida patients, is difficult to explain.
Organ-conserving surgery was successfully performed in the majority of patients with histopathic uterine rupture. Stitching up R.M. performed in 45 (88.2%), hysterectomy after ineffective ligation of the internal iliac arteries - in 6 (11.8%). To reduce blood loss during suturing of the RM, ligation of the internal iliac arteries was used in 23 (45.1%), ligation of the uterine arteries on both sides - in 12 (23.5%). Total blood loss in a volume of less than 1000 ml was in 10 (19.6%), 1001-2000 ml - in 18 (35.4%), 2001-3000 ml - in 8 (15.7%), 3001-4000 ml - in 7 (13.7%), 4001-5000 ml - in 7 (13.7%), 5600 ml - in 1 (1.9%).
Reinfusion of autoerythrocytes with the Cell-Saver device was used in 24 (47.1%) patients. Its volume varied from 200 to 1900 ml. Transfusion of donor red blood cells with a volume of 233-2250 ml was performed in 26 (51%) women.
The length of hospital stay varied from 6 to 27 days. In 9 (17.6%) patients the postoperative period proceeded with complications. Endometritis was diagnosed in 1, ureteral fistula and hydronephrosis (after hysterectomy) - in 1, postoperative wound seroma - in 1, impaired urine outflow - in 1, pleurisy - in 2, peritonitis - in 2, acute gastric ulcer - in 1.
Group 3 (n=6) – forced uterine rupture. The age of the subjects ranged from 23 to 38 years, with an average of 28.4±5.9 years. There were 2 primiparous patients, 4 were about to give birth for the second time. 3 patients had a history of abortion, 1 patient had a large fetus, complicated by postpartum endometritis.
All births were timely. By vacuum extraction of the fetus with a high-standing head, 3 patients were delivered; abdominal forceps were used in 2; caesarean section after an unsuccessful attempt to apply abdominal forceps was performed in 1. The weight of the children was from 3200 to 3590 g in 3 patients, 3700-3950 g - in 3. 4 children were born with severe asphyxia, 2 with mild asphyxia.
Laparotomy revealed that all RMs were incomplete and localized in the lower segment, of which in 2 women the tear to the lower segment extended from the cervix.
All patients had the rupture sutured. Ligation of the internal iliac arteries was performed in 4 patients. Blood loss from 400 to 1600 ml was in 4 women, 4500 and 5500 ml in 2. Hardware reinfusion of autoerythroid suspension was performed in one postpartum woman. Donor red blood cells were used in 3 cases. The postoperative period ranged from 7 to 28 days.
Of the 92 women with RM, 2 died. One patient with a third upcoming birth (with a history of 2 spontaneous births and 2 abortions) underwent an emergency cesarean section due to suspected premature abruption of a normally located placenta, bleeding, and intrapartum fetal death. Intraoperatively, a hematoma was discovered in the right parametrium, reaching the lower pole of the right kidney. After emptying the hematoma, a 12 cm long RM was diagnosed along the right “rib”. Hysterectomy was accompanied by blood loss of 5000 ml (81% of circulating blood volume). Cardiac arrest occurred due to inadequate replacement of blood loss (donor red blood cells were not transfused, 2245 ml of fresh frozen plasma was transfused).
Another patient with a second upcoming birth underwent abdominal forceps surgery due to acute fetal hypoxia. The extraction failed and the birth was completed by caesarean section. Intraoperatively, RM was diagnosed along the left “rib” to the internal pharynx with injury to the vascular bundle and the formation of a hematoma in the parametrium. The RM was sutured with a blood loss of 5500 ml (72% of the circulating blood volume). Death occurred on the 25th day from multiple organ failure due to untimely and insufficient replacement of blood loss. A child weighing 3700 g was born with severe asphyxia (Apgar score 1) and died on the 39th day.
The condition of newborns with rupture of the unoperated uterus is presented in Table. 2.
Table 2. Condition of children born after rupture of the unoperated uterus
Clinical manifestations of different stages of the process
Symptoms of uterine rupture are varied and depend on the stage of the process. The mechanism and timing of injury have important implications for clinical symptoms. Sometimes, with obvious changes in the wall, symptoms at the initial stage are minimal, and gradual tissue growth is observed, which is difficult to diagnose.
Threatening
If there is persistent scarring or tissue inflammation, this may occur after 30 weeks of pregnancy. Myometrial stretch reaches its maximum during this period. The woman has the following symptoms:
- A nagging pain in the lower abdomen and lower back that cannot be clearly defined;
- low blood pressure;
- scanty bleeding from the genital tract;
- increased uterine tone;
- decrease in vital parameters of the fetus.
During childbirth, rapid rupture is manifested by various symptoms:
- quick birth;
- overload of the lower segment and change in the shape of the abdomen;
- sharp pain when touching the uterus;
- severe swelling of the vagina and swelling of the genitals;
- persistent leakage of amniotic fluid.
Symptoms of birth trauma may be more subtle due to frequent use of pain medications.
Started
The next stage is characterized by all of the above symptoms, but they can appear in various combinations and be more serious.
Contractions become sharp, painful, sometimes accompanied by convulsions. Sharp pain in the lower abdomen in the uterine area persists even after contractions. The woman's state is excited, her pupils are dilated, and a feeling of fear appears. Vaginal bleeding is light, and there may be urinary retention or small amounts of blood in the urine. The fetal head stops moving along the birth canal, and pronounced swelling appears above the uterus.
The fetal condition is deteriorating. It can become overactive. CTG examination shows increased or rapid heart rate and muffled sounds. If this stage is not treated, fetal death occurs in 80% of cases.
Accomplished
The symptoms of what is happening correspond to the clinical signs of massive bleeding. But first there is a sharp pain in the lower abdomen. A woman may feel like something has broken inside her. In this case, the contractions stop abruptly, the fetus rolls down and dies. The shape of the abdomen changes and parts of the fetus can be felt under the skin. The woman’s condition is serious, bleeding symptoms predominate:
- low blood pressure;
- pale skin;
- dry mouth;
- weakness, loss of consciousness;
- tachycardia;
- The pulse is practically not felt.
Bleeding from the genital tract increases. The uterus becomes irregular as it moves upward. The fracture along the length of the scar produces a convexity; there is a convexity along the anterior wall. In case of incomplete rupture and hematoma formation, it is felt as a bulky mass adhering to the lateral surface.
If the rupture occurred during the expulsion period, the child may remain alive and not show signs of hypoxia. But immediately after childbirth, the mother’s condition deteriorates sharply, massive bleeding begins, and symptoms of hemorrhagic shock appear.
Recovery process and suture care
How long a woman in labor will take to recover depends on the severity of the injuries. The shortest period of recovery and healing of perineal ruptures after childbirth occurs from 4 months.
In the first days, the seams are treated with brilliant green or hydrogen peroxide. Next, the patient must follow simple rules so as not to harm or disturb the seam.
- After each visit to the toilet, wash with warm water, moving from the vagina to the anus (from front to back.)
- Keep the seam areas dry by blotting them with a towel or paper napkin.
- Wear sanitary pads and change them every 2 hours if possible.
- The perineal area should have access to air.
- Walk more often, provided there is no discomfort or pain.
- Monitor digestion, avoiding constipation or eliminating it with rectal glycerin suppositories.
- If you notice a strange smell, an increase in body temperature, discharge of a strange color, and the pain begins to intensify, consult a doctor immediately.
- Try not to sit down for a week. If you really want to sit down, it’s best to do it on an inflatable rubber ring to prevent the seams from coming apart.
Diagnostic techniques
Already during pregnancy, pregnant women undergo examination and are classified as at risk of developing congenital anomalies. A history of miscarriage, chronic inflammation of the uterus, previous cesarean section or surgery increases the likelihood of injury.
Assessing the integrity of the scar is mandatory. Vaginal birth after the first cesarean section is not contraindicated, but a second cesarean section is often preferred in the post-Soviet space.
Diagnosing a rupture during labor can be difficult. The doctor must urgently assess the deterioration of the condition of the mother and fetus, determine the diagnosis and tactics of the procedure.
When examining the birth canal, the following symptoms are noted:
- increased obstetric swelling on the fetal head;
- no head advancement;
- The anterior part of the mucous membrane of the cervical spine is pinched and swollen;
- The swelling spreads to the vagina and external genitalia.
Upon external examination, the contractile ring is high and may be inclined.
Diagnosis includes measuring blood pressure and pulse. To determine the condition of the fetus, CTG is performed.
When a first-degree uterine rupture occurs during childbirth, diagnosis is not difficult. There are all signs of massive bleeding; the woman’s condition requires emergency assistance.
Sometimes the diagnosis can be made after birth. The woman has abdominal bloating. Manual examination of the uterine cavity allows you to identify the defect and take the necessary measures to eliminate bleeding and its consequences. If the disease is not diagnosed in the delivery room, symptoms of peritonitis appear the next day.
Caring for a woman during pregnancy and childbirth
Women with an imminent breakup should not be transported. This means that she should not be transferred to another hospital if she develops worrying symptoms, even if adequate care cannot be provided under the circumstances. Fetal and maternal death may occur during transmission when treatment is not possible.
Clinical guidelines for this complication prohibit active labor and require delivery by cesarean section. The woman is given deep anesthesia. If the fetus is still alive, the operation is performed regardless of the obstetric situation.
Even if the fetal head is in the pelvic cavity, you should not try to remove it without surgery. Then the state of emergency would become a fait accompli.
If the fetus is dead, a caesarean section is not performed but is replaced by surgery to remove the fetus.
The treatment protocol for a uterine rupture that has already occurred includes performing an emergency laparotomy. In this case, childbirth is not carried out, since fetal death occurs almost immediately. It is necessary to stop the bleeding and prevent the development of severe hemorrhagic shock and disseminated intravascular coagulation. Therefore, already in preparation for surgery, blood, plasma or other anti-shock solutions should be transfused.
We are trying to complete the operation as soon as possible. This requires ligation of the feeding vessels and elimination of bleeding. Indications for hysterectomy in case of rupture have been determined:
- hemorrhagic shock;
- damage to the main vascular bundle;
- extensive gap.
In the case of a linear crack, the wall defect is sutured. The abdominal cavity is inspected and blood clots are removed. In case of incomplete rupture, it is necessary to remove the resulting hematoma, determine the source of bleeding and stop it.
After surgery, infusions of solutions are prescribed to compensate for blood loss and antibiotics to prevent infectious complications. Accurate anesthesia is required.
Women who have lost a child during childbirth may need the help of an experienced psychologist.
Why is this happening?
Now let's look at the reasons for perineal rupture during childbirth.
Birth ruptures can happen if:
- labor is too fast;
- the woman in labor suffered from infections in the reproductive and reproductive systems;
- before pregnancy, the woman did not cure diseases that loosen the pelvic tissue (vulvovaginitis, vaginitis, thrush);
- failure to follow the obstetrician’s instructions (push and relax at the wrong time);
- swelling of the perineum is observed;
- breech presentation of the fetus (in this case, a caesarean section is prescribed);
- occipital presentation, i.e. the head moves as expected, but the back is turned upward if the woman in labor is lying down;
- the fetus is past term (41-42 weeks);
- the fruit is too large;
- the woman in labor has a so-called narrow pelvis, i.e. the child is larger than the size of the pelvis;
- there is no control of labor;
- the midwife’s actions to protect the perineum are incorrect;
- during childbirth, obstetric forceps or a vacuum extractor are used to extract the fetus;
- the woman in labor had previously had ruptures or incisions that left scars;
- there are scars from laser treatment of erosion before pregnancy;
- the distance between the anus and vagina is large (7-9 cm - “high perineum”;
- late birth (the mother in labor is no longer young);
- a woman in labor is professionally involved in sports, which is why the muscles involved in childbirth are pumped up.
Photo source: shutterstock.com
Consequences and possibilities of prevention
The consequences of myometrial rupture can be dire. This condition, even with the current level of maternal health care, is accompanied by a high percentage of fetal death. A woman suffering from heavy bleeding requires a long recovery period.
Blood transfusion is always accompanied by a risk of contracting HIV and hepatitis C. However, the danger is massive bleeding, which leads to hypoxia of the pituitary gland and the development of Sheehan syndrome. This hormonal imbalance makes it difficult to become pregnant again.
Prevention takes place even at the stage of pregnancy planning. Women after surgery require a comprehensive assessment of the density of the uterine scar, which should include not only ultrasound data, but also hysteroscopy.
Your doctor's instructions should be followed throughout your pregnancy. If several risk factors are present, birth may only take place in first- or second-degree institutions, including regional maternity hospitals and large perinatal centers. Hospitalization should be carried out in advance.