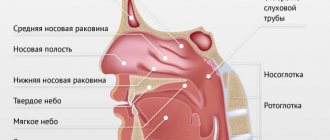
Rhinolalia is a speech disorder manifested by severe distortion of speech and incorrect pronunciation of individual sounds. As a rule, the development of this speech pathology is caused by an abnormal structure of the speech apparatus. The speech of a child with rhinolalia has a specific sound: since this pathology involves a violation of the resonator function of the nose, air flows incorrectly, which provokes deformation of sounds.
In addition to sound distortions, rhinolalia can cause difficulties in the lexical and grammatical development of a child’s speech. To exclude the development of psychological problems, specialized work with a child with rhinolalia is necessary.
Symptoms of rhinolalia
With organic rhinolalia, the diagnosis is made in infancy. From the first days such children have problems with nutrition and breathing and are susceptible to respiratory diseases.
The formation of speech in children with rhinolalia is difficult and occurs after 2 years. A sick child pronounces sounds, syllables and words late. They are unclear and difficult to understand.
In the open form, the sounds have a nasal timbre and are indistinguishable from each other. Closed rhinolalia manifests itself in a violation of the pronunciation of nasal sounds and their replacement with others. The timbre of the voice also suffers.
The disease also causes other disorders - dysgraphia and dyslexia, as well as persistent psychological discomfort. That’s why diagnosing rhinolalia and treating it is so important.
Diagnosis of rhinolalia
The examination of children and adults with rhinolalia is multifaceted and is carried out by various specialists:
- otolaryngologist;
- speech pathologist;
- speech therapist;
- neurologist;
- orthodontist;
- phoniatrist;
- pediatrician
An examination by specialized specialists allows us to identify the etiology of the disease, characterize as accurately as possible the nature of pathological changes and the severity of all symptoms. The following instrumental diagnostic methods are important:
- X-ray of the nasopharynx;
- rhinoscopy;
- electromyography;
- pharyngoscopy, etc.
These techniques make it possible to visualize the nature of pathological changes and their severity in each individual patient.
Of course, the most significant is an examination by a speech therapist, who, using a number of progressive techniques, will be able to assess the following parameters:
- structure of the articulatory apparatus;
- his mobility;
- voice disorders;
- parameters of physiological and phonation breathing, etc.
To diagnose open rhinolalia, the Gutzmann technique is used, which is based on the fact that the patient pronounces the sounds “a” and “i” alternately, while the doctor opens and closes the nasal passages. In the presence of pathological changes, the vibration of the wings of the nose is very clearly felt, and when the nasal passages are pinched, the sounds are significantly muffled. Thus, it is possible to diagnose the open form of rhinolalia.
Correction of rhinolalia at a speech therapy center in Moscow
Corrective work with children with rhinolalia should begin when a problem is detected in order to achieve positive results by adolescence. Depending on the form, speech therapy work can be the main or complementary work of other specialists.
The role of a speech therapist for rhinolalia is to consolidate sound pronunciation skills. Massage is used, the development of velopharyngeal closure, the development of exhalation and sound pronunciation, the elimination of nasality, the development of vocabulary and work on lexical literacy.
- Correction for functional rhinolalia. A positive effect can be achieved through sessions with a speech therapist. They include massage, breathing exercises, work on developing the correct pronunciation of sounds and auditory attention.
- Correction for organic form. The effectiveness depends on the surgical intervention, the timeliness of the operation and the completeness of the speech therapist’s work with the child.
Cause of rhinolalia
Rhinolalia usually occurs in an open form. It occurs when there is a split in the hard and soft palate, the alveolus of the lip, or the upper part of the entire speech apparatus. The causes of the pathology are caused by various highly pathogenic effects on the embryo in the period between the 5th and 8th weeks of development.
Typically, the reasons for such effects are associated with problems of the mother’s body during pregnancy such as:
- Flu;
- Mumps;
- Toxoplasmosis;
- Rubella;
- All kinds of endocrine disruptions;
- Abuse of bad habits (alcohol, smoking, etc.);
- ENT disorders in the fetus.
- The causes of the appearance of a closed form of rhinolalia are usually:
- Deviation of the nasal septum;
- Fibroids;
- Polyps;
- Tumors;
- Critical proliferation of adenoids.
Working to overcome the consequences of rhinolalia
Due to the organic origin of the disorder, surgical intervention is often required. A speech therapist is involved in correctional work. Speech therapy correction includes preoperative and postoperative periods. Work in each period is aimed at solving existing problems:
- development and differentiation of oral and nasal breathing,
- development of mobility and accuracy of movements of the organs of articulation,
- education of correct sound pronunciation,
- development of phonemic awareness.
- development of fine motor skills of the fingers,
- An adequate form of speech therapy is massage of the organs of articulation and hands.
Classification
- Open. It is observed when there is incomplete separation or absence of a barrier between the nasal and oral cavities, when sound penetrates through the oral nasal cavity.
- Closed. It is observed when there are obstructions in the nasal cavity or nasopharynx. Depending on the location of the anatomical obstacle, anterior and posterior closed rhinolalia are distinguished. A characteristic feature is decreased physiological nasal resonance.
- Mixed. It is observed when there is insufficient separation of the nasal and oral cavities and the presence of anatomical obstacles. Characterized by nasality and absence of nasal sounds.
The listed types of rhinolalia can be functional or organic in nature.
Types of rhinolalia (diagram)
Open rhinolalia
The timbre of consonants and vowels “A”, “I”, “U” is disrupted. When drawing a conclusion, samples are used:
- Gutzman's test (the child is asked to sing the vowels “A”, “I”, while the speech therapist’s fingers then clamp and then unclench the nasal passages - as a result, the sound “I” becomes duller, vibration is felt under the fingers);
- test using a phonendoscope (the child is asked to pronounce the vowels “I”, “U” - an incomprehensible hum is heard in the “olive”).
Functional open rhinolalia occurs after operations for adenoiditis or after post-diphtheria paresis and is characterized by a weak rise of the soft palate.
Organic open rhinolalia:
- acquired (pathology of the glossopharyngeal and vagus nerves, trauma, pressure from tumor formations);
- congenital (etiology: clefting of the soft or hard palate, shortening of the soft palate).
Types of congenital cleft palates
Mechanism of violations:
- absence of a velopharyngeal seal;
- the child’s lack of understanding of the difference between the nasal and oral sounds of the voice;
- modification of the localization and method of articulation of sounds due to an anomaly, reduced muscle tone.
- hypertonicity of facial muscles.
Logocorrection for open rhinolalia
The effectiveness of the measures taken depends on the anatomical and physiological state of the oral-nasal region and the complexity of medical, psychological and pedagogical measures.
The purpose of preoperative language intervention is to prevent possible secondary deviations in the psychophysical development of the child, such as oral agrammatisms, poor vocabulary in preschool age and specific errors in reading and writing in school. During the correction, exercises to activate the cerebral cortex, games to develop phonemic hearing, logorhythmics, art therapy techniques, and family psychotherapy are widely used.
Closed rhinolalia
It is divided into functional (the soft palate rises when pronouncing nasal sonorous sounds, blocking the access of air into the nasopharynx) and organic (anatomical obstruction in the new cavity).
Stages of speech therapy work for closed rhinolalia
- Elementary. Differentiation of nasal and oral exhalation, development of short and long nasal exhalation.
- Staged. Setting and automation of phonemes “M”, “M”, “N”, “N”.
- Final. Work on voice formation and sonority of vowel sounds. Differentiation of consonants by nasality and non-nasality in isolation, in syllables, words, sentences and texts.
Mixed rhinolalia
Combines the causes and combines the symptoms of the previous 2 types of rhinolalia.
In general, the prognosis is favorable. However, positive dynamics can be accelerated by including parents in the correction process with subsequent integration and socialization of the child with rhinolitis.
Types of cleft palate
Rhinolalia is often a consequence of clefts in the oral cavity, which can be congenital or acquired. Among congenital clefts there are clefts of the face, lip, nose, hard and soft palate. The degree of paresis varies from facial asymmetry to complex combined distortions of parts of the face and complete asymmetry in the eye. Clefts can be unilateral or bilateral. Unilateral are more often observed on the left (70%), more often in men than in women. 69% of men have a cleft lip in combination with a cleft palate, but of the remaining 31%, women are twice as likely to have an isolated cleft palate.
The following types of clefts have been recorded in medicine:
isolated cleft lip (“cleft lip”);
- combination of cleft lip and alveolar process;
- lips, alveolar process and hard palate;
- lips, alveolar process of the hard and soft palate (“cleft palate”);
- damage to the alveolar process and hard palate;
- paresis of the hard and soft palate;
- defect of the soft palate;
- cleft of the small tongue.
Cleft palates are often combined with clefts in the nasal septum, resulting in deformation in the patient - a double nose, a proboscis instead of a nose. The nasal passages may even become clogged.
Acquired clefts occur as a result of tumors, injuries, wounds, and frequent operations. More often they occur in people working in mines, logging sites, and participating in military operations involving explosions.
Correction methods
Treatment of rhinolalia includes a whole range of measures aimed at maximizing the elimination of speech defects.
If a child is diagnosed with congenital rhinolalia, then correction of the disorder begins with the elimination of defects of anatomical origin. From birth, such children begin to be fed using a tube, which is selected taking into account the characteristics of the cleft.
A special prosthesis, an obturator, is also made to close the nonunion. This prosthesis facilitates the processes of eating, breathing and speaking.
Late use of an obturator is less effective, since the child begins to develop incorrect tongue position with age. The obturator changes as the child grows and is used until the moment of surgical intervention, which, unfortunately, cannot be done without.
Maxillofacial disorders are subject to surgical intervention. Nasality with open rhinolalia is treated both before and after surgery.
As a rule, cleft lip surgery is performed at 2–3 months of a child’s life. Operations on the palate are carried out after two years, if the child has lost all his teeth. In weakened children, surgery is postponed to a later date or carried out in several stages.
Surgeries allow you to restore the integrity of the speech apparatus and the proper functioning of the palate.
Treatment and diagnosis
Doctors such as speech therapist, speech therapist and neuropsychiatrist are involved in the examination and development of treatment strategy for the treatment of childhood speech dysfunction caused by rhinolalia. Since the symptoms of the pathology are quite extensive and are caused by various reasons, in the treatment of rhinolalia there may be a need for the services of an orthodontist, dentist, otolaryngologist, and in some particularly severe cases, a plastic maxillofacial surgeon.
A defectologist and speech therapist are responsible for diagnosing the state of development of the speech and cognitive sphere of a child with rhinolalia, as well as developing developmental teaching methods. A child with rhinolalia is usually prescribed articulation exercises and exercises to develop phonemic hearing, speech therapy massage and breathing exercises.
Where to treat rhinolalia to be sure of the result
The NeuroSpectrum Center for Pediatric Speech Neurology and Rehabilitation is a modern medical center that treats patients with impaired or absent speech, mental development disorders, developmental delays, and so on. Patients diagnosed with Rhinolalia
This is also not uncommon here, and the center knows exactly how to make a correct diagnosis and what treatment will be most effective.
The specialists of our Center have extensive experience working with patients with rhinolalia; they have modern diagnostic and medical equipment at their disposal, so we are ready to solve problems of any level of complexity. However, it must be remembered that at an earlier stage of rhinolalia, treatment will be less expensive and more effective, so you should not delay contacting specialists.