Symptoms of the disease
In the first 10 days after infection, the disease occurs without symptoms. After this, the patient begins to be bothered by the following symptoms:
- moderate headache;
- muscle pain;
- feeling of tiredness, fatigue;
- temperature increase;
- nausea;
- vomit;
- diarrhea.
Some patients also experience decreased appetite, often leading to anorexia. Voluminous red spots appear on the skin.
Symptoms of erysipelas of the lower extremities
- quite noticeable headache
- high temperature, which is very difficult to bring down
- chills
- vomiting like food poisoning
- burning sensation on the skin
- severe redness on the skin
- The area of skin affected by erysipelas differs from healthy skin - it is either convex or separated by a small ridge.
If you notice such symptoms, you should immediately consult a doctor so as not to start the disease, because erysipelas can become more complicated.
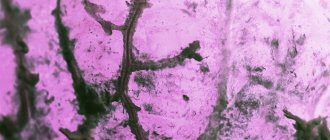
This is what erysipelas looks like
If erysipelas is a consequence of varicose veins, then such a complication may be thrombophlebitis, in which inflammation spreads to the wall of the veins, and then a blood clot forms in the lumen of the vein. Another complication of erysipelas with varicose veins is tissue necrosis, leading to the appearance of trophic ulcers that are difficult to treat.
Medicines for treatment
The basis of therapy is antibiotics. The best therapeutic effect for erysipelas is provided by Biseptol, Erythromycin, Oleanodomycin.
Antibiotics are taken in combination with vitamins A, B, C, anti-inflammatory drugs, diuretics and medications to reduce vascular permeability.
The treatment regimen, dosage of drugs and duration of therapy are determined by the doctor individually for each patient.
Effective ointments
Erythromycin ointment effectively treats erysipelas. Belongs to the group of antibiotics, allows you to fight the direct causative agent of infection - streptococcus. A very high-quality product for external use, which also has an affordable price.
Optimal treatment regimen: apply the product to the affected area three times a day. It is permissible to make compresses - fold the bandage in several layers, apply a thick layer of ointment on it and apply it to the infected area, fixing it on the leg.
Tetracycline ointment has a similar effect. Refers to potent antibiotics, the method of use is identical to Erythromycin ointment.
Streptocide
For erysipelas, streptocide will help, which has a bactericidal and antimicrobial effect. Moreover, it can be used both internally and externally. For oral administration, 0.5 g is prescribed, which must be taken every 5-6 hours.
For external use, use sterile powder (no more than 15 g per procedure). The infected area is treated with powder.
Important! The recommendations presented should not be taken as instructions for action. Any drugs for internal and external use must be prescribed by a doctor!
At-risk groups
Most often, women over 50 years of age are affected by this disease, but it can also occur in infants. In their case, infection occurs after streptococcus enters the wound of the umbilical region. There is no explanation for this fact, but people with blood group III suffer from erysipelas more often. There is also a connection with the place of residence. In South Asia, as well as in Africa, this disease is very rare.
People with a low level of immunity, weakened by illness, stress, treatment and other factors are at risk.
Folk remedies for the treatment of erysipelas
The secrets of traditional medicine are no less effective in treating erysipelas on the skin.
Beaver jet treatment
Beaver stream is available in the form of extract and powder. The powerful healing composition of the product has a bactericidal effect, accelerates wound healing, and strengthens the immune system.
To treat erysipelas, the affected area is treated with sterile powder. You can also make compresses - a bandage folded in several layers is moistened in the extract and fixed on the leg in the affected area.
Potato
Raw potatoes will help treat erysipelas. It must be grated on a fine grater and squeezed thoroughly to form juice. Soak a gauze bandage in it, then apply it to the leg at the site of infection. Change the bandage at least 4 times a day.
Honey
Honey is a natural antibiotic and has an antiseptic, anti-inflammatory, and decongestant effect. To treat erysipelas, you need to generously smear red silk fabric with honey and fix it in the area where the disease appears.
If you perform this procedure daily, you will notice a positive result within a week.
Herbal decoctions, compresses and infusions
Using infusions, compresses and decoctions, you can make effective medicinal lotions:
- fresh plantain leaves in a mortar and then chop. Add thick honey and stir. Place the mixture in a water bath, wait until the honey becomes semi-liquid. Let the mixture brew for 2-3 hours. Treat your foot with the prepared infusion every day.
- the yarrow leaves thoroughly and pour boiling water over them. Leave for 2 hours. Take out the leaves and apply them to your leg. Apply a gauze bandage soaked in the infusion on top.
- calendula, dandelion (flowers), oak bark in equal proportions . Fill with water and place on low heat. Bring to a boil, remove from heat and cool. Rinse your foot regularly with the decoction.
- Mix dry chamomile and coltsfoot leaves , then add thick honey and stir until smooth. Apply the resulting mixture to the skin, after half an hour, clean the body with a damp cotton swab.
It is important to remember that infusions and decoctions should be at a comfortable temperature when used.
What is erysipelas or erysipelas?
This is one of the most unpleasant inflammatory diseases, which mainly affects the face and limbs. It not only brings with it fever and pain, but also causes a lot of inconvenience.
Erysipelas on our patient’s leg
The causative agent of erysipelas is staphylococcus, a bacteria that can destroy the vital activity of cells. Usually the human body is quite resistant to this disease. However, during periods of decreased general and local immunity, erysipelas may appear with varicose veins. Even the leading and best European specialists are familiar with this disease first-hand. Both surgeons and dermatologists in public clinics and phlebologists in private city medical centers encounter erysipelas in their patients. Every year, thousands and thousands of patients in Moscow and the Moscow region seek help with signs of erysipelas. Only a fraction of them receive really good treatment, even in Moscow. The best solution when symptoms of erysipelas appear is to find a good specialist who will conduct modern diagnostics and prescribe adequate treatment.
Other effective treatments
There are several more effective folk methods for treating erysipelas:
- Fresh cottage cheese will help cope with infectious diseases . It needs to be laid out in a thick layer on the leg, where the disease manifests itself. As soon as the cottage cheese begins to dry out, you need to remove it and add a fresh layer. Repeat at least 5 times in a row.
- One of the most popular folk methods for treating erysipelas is the use of chalk . It needs to be crushed into powder, sprinkled on the affected area, covered with a gauze bandage and wrapped in a towel.
- Chitosan gel with silver ions ArgoVasna Lilac has proven itself well in the treatment of erysipelas. Silver ions have a bactericidal effect on the skin, chitosan (crushed crab shell) promotes skin healing, lilac is famous for its anti-inflammatory, absorbable and anti-edema properties. The properties of lilac are used in folk medicine to heal minor wounds and for erysipelas.
- In treatment, you can use not only raw potato juice, but also potato starch . Pour a teaspoon of starch onto a cotton swab, apply it to your leg and fix it. This compress can be kept for up to 2 hours. Repeat the procedure three times a day.
- the burdock leaf very thoroughly, then generously grease it with sour cream. Apply to the leg in the area of redness and wrap with gauze or a towel. Apply the compress 4-5 times a day. The compress can be made with ready-made burdock root extract. It can be taken orally, in combination with lotions. This will speed up the healing process.
If during the procedure the patient feels discomfort, such as itching or redness, it is better to stop treatment with the chosen method.
Contraindications
Any medical procedures should be carried out only in consultation with a doctor. Contraindications include:
- pregnancy;
- lactation period;
- immunity of the body to the components of the composition.
An allergic reaction to the components included in the drug may also develop.
In order not to aggravate the patient’s condition, self-medication is prohibited! It is important to remember that both medications and traditional medicine can cause negative consequences.
Erysipelas: CLINIC, DIAGNOSTICS, TREATMENT
• According to the nature of local manifestations: a) erythematous; b) erythematous-bullous; c) erythematous-hemorrhagic; d) bullous-hemorrhagic. • According to the degree of intoxication (severity): I - mild; II - moderate; III - heavy. • By flow rate: a) primary; b) recurrent (occurring after 2 years, different localization of the process) c) recurrent. If there are at least three relapses of erysipelas per year, the definition of “frequently recurrent erysipelas” is appropriate. • According to the prevalence of local manifestations: a) localized erysipelas; b) common (migratory) erysipelas; c) metastatic erysipelas with the appearance of distant foci of inflammation. • Complications of erysipelas: a) local b) general. • Consequences of erysipelas: a) persistent lymphostasis (lymphatic edema, lymphedema); b) secondary elephantiasis (fibredema). Primary, repeated erysipelas and the so-called late relapses of the disease (after 6 - 12 months and later) are an acute cyclic infectious process that occurs as a result of exogenous infection with group A b-hemolytic streptococcus. The source of infection in this case is both patients with a variety of streptococcal infections and and healthy streptococcus bacteria carriers. The main transmission mechanism is contact (microtraumas, abrasions, skin rash, etc.). The airborne transmission mechanism of streptococcus with primary damage to the nasopharynx and subsequent introduction of the microbe to the skin by hand, as well as by lymphogenous and hematogenous routes, is also of particular importance. Recurrent erysipelas, in which early and frequent relapses of the disease occur, is formed after a primary or recurrent erysipelas due to inadequate treatment, the presence of unfavorable background and concomitant diseases (varicose veins, mycoses, diabetes mellitus, chronic tonsillitis, sinusitis, etc.), the development of secondary immune deficiency, defects in nonspecific defense of the body. Foci of chronic endogenous infection form in the skin and regional lymph nodes. Along with the bacterial forms of group A streptococcus, when the process is chronic, the L-forms of the pathogen are also of great importance, persisting for a long time in the macrophages of the skin and organs of the mononuclear-phagocytic system. Reversion of L-forms of streptococcus into the original bacterial forms leads to another relapse of the disease. Erysipelas usually occurs against the background of pronounced sensitization to b-hemolytic streptococcus and is accompanied by the formation of fixed immune complexes in the dermis, including perivascularly. When infected with streptococcus, the disease develops only in individuals who have a congenital or acquired predisposition to it. Infectious-allergic and immunocomplex mechanisms of inflammation in erysipelas determine its serous or serous-hemorrhagic nature. The addition of purulent inflammation indicates a complicated course of the disease. Patients with erysipelas are less contagious. Women get erysipelas more often than men, especially the recurrent form of the disease. In more than 60% of cases, erysipelas occurs in people aged 40 years and older. Unlike other streptococcal infections, erysipelas is characterized by a distinct summer-autumn seasonality. In recent years, there has been an increase in the number of cases of hemorrhagic erysipelas, which is characterized by slow tissue repair at the site of inflammation, a tendency towards a protracted (chronic) course of the infectious process, and a high frequency of complications. Clinical picture of erysipelas
The incubation period ranges from several hours to 3 - 5 days. In patients with recurrent erysipelas, the development of another attack of the disease is often preceded by hypothermia and stress. In the vast majority of cases, the disease begins acutely. Initial period
The disease is characterized by the rapid development of intoxication symptoms, which in more than half of patients (usually when erysipelas is localized on the lower extremities) precede the onset of local manifestations of the disease by several hours to 1–2 days.
Headache, general weakness, chills, and muscle pain are noted. Nausea and vomiting occur in 25–30% of patients. Already in the first hours of illness, the temperature rises to 38 - 40°C. In areas of the skin in the area of future local manifestations, a number of patients experience paresthesia, a feeling of fullness or burning, and mild pain. Often pain also occurs in the area of enlarged regional lymph nodes. The height of the disease
occurs within a period of several hours to 1 - 2 days after the first manifestations of the disease.
General toxic manifestations and fever reach their maximum. Characteristic local manifestations of erysipelas occur. Most often, the inflammatory process is localized on the lower extremities (60 - 70%), less often on the face (20 - 30%) and upper extremities (4 - 7%), very rarely only on the torso, in the area of the mammary gland, perineum, external genitalia . With timely treatment and uncomplicated course of erysipelas, the duration of fever usually does not exceed 5 days. In 10 - 15% of patients, fever persists for longer than 7 days, which is usually observed with a widespread process and insufficient adequate etiotropic therapy. The longest febrile period is observed with bullous hemorrhagic erysipelas. More than 70% of patients with erysipelas develop regional lymphadenitis, which develops in all forms of the disease. The period of convalescence.
Normalization of temperature and disappearance of symptoms of intoxication are observed with erysipelas earlier than the disappearance of local manifestations.
Acute local manifestations of the disease persist for up to 5 - 8 days, in hemorrhagic forms - up to 12 - 18 days or more. Residual effects of erysipelas that persist for several weeks and months include pasty and pigmented skin, congestive hyperemia at the site of faded erythema, dense dry crusts at the site of bullae, and edematous syndrome. Unfavorable prognostic significance (the likelihood of an early relapse) are persistent enlarged and painful lymph nodes, skin infiltrates in the area of the extinguished source of inflammation, and low-grade fever. Prognostically unfavorable is also the long-term persistence of lymphatic edema (lymphostasis), which should be considered as an early stage of secondary elephantiasis. Hyperpigmentation of skin areas on the lower extremities in patients who have suffered from bullous hemorrhagic erysipelas can persist for life. Erythematous erysipelas
can be either an independent clinical form of erysipelas or the initial stage of development of other forms of erysipelas.
A small red or pink spot appears on the skin, which within a few hours turns into the characteristic erythema erysipelas. Erythema is a clearly demarcated area of hyperemic skin with uneven boundaries in the form of teeth and tongues. The skin in the area of erythema is infiltrated, tense, hot to the touch, moderately painful on palpation (more along the periphery of the erythema). In some cases, a “peripheral ridge” can be detected in the form of infiltrated and raised edges of erythema. Along with hyperemia and infiltration of the skin, its edema develops, spreading beyond the erythema. Erythematous-bullous
erysipelas develops in a period of several hours to 2 - 5 days against the background of erythema erysipelas.
The development of blisters is associated with increased exudation at the site of inflammation and detachment of the epidermis from the dermis by accumulated fluid. When the surfaces of the blisters are damaged or they spontaneously rupture, exudate leaks out, and erosion often occurs in large quantities at the site of the blisters. While maintaining the integrity of the blisters, they gradually shrink to form yellow or brown crusts. Erythematous-hemorrhagic
erysipelas develops against the background of erythematous erysipelas within 1 to 3 days from the onset of the disease, sometimes later.
Hemorrhages of various sizes appear - from small petechiae to extensive confluent hemorrhages, sometimes throughout the entire erythema. Bullous-hemorrhagic
erysipelas transforms from the erythematous-bullous or erythematous-hemorrhagic form and occurs as a result of deep damage to the capillaries and blood vessels of the reticular and papillary layers of the dermis.
Bullous elements are filled with hemorrhagic and fibro-hemorrhagic exudate, and extensive hemorrhages occur in the skin in the area of erythema. The resulting blisters come in different sizes and are dark in color with translucent yellow inclusions of fibrin. The blisters may also contain predominantly fibrinous exudate. The appearance of extensive flattened blisters, dense on palpation due to significant deposition of fibrin in them, is possible. In patients with active repair in the lesion, brown crusts quickly form at the site of the blisters. In other cases, the covers of the blisters rupture and are rejected along with clots of fibrinous-hemorrhagic contents, exposing the eroded surface. In most patients, its gradual epithelization occurs. With significant hemorrhages in the bottom of the bladder and the thickness of the skin, necrosis may develop, sometimes with the addition of secondary suppuration and the formation of ulcers. According to the specialized erysipelas department of the 2nd Clinical Infectious Diseases Hospital (Moscow), in patients hospitalized in the department in 1997, the erythematous or erythematous-bullous form was diagnosed in 5.2% of cases, the erythematous-hemorrhagic form - in 48.8% , bullous-hemorrhagic - in 46%. The severity criteria
for erysipelas are the severity of intoxication and the prevalence of the local process.
The mild (I) form of erysipelas includes cases with minor intoxication, low-grade fever, and a localized (usually erythematous) local process. The moderate (II) form of the disease is characterized by severe intoxication. There is general weakness, headache, chills, muscle pain, sometimes nausea, vomiting, fever up to 38 - 40 ° C, tachycardia, and in almost half of the patients - hypotension. The local process can be either localized or widespread (involves two anatomical areas) in nature. Severe (III) form of erysipelas includes cases of illness with severe intoxication: intense headache, repeated vomiting, hyperthermia (above 40°C), sometimes blackout, symptoms of meningism, convulsions. Significant tachycardia and often hypotension are observed; in elderly and senile people, with late treatment, the development of acute cardiovascular failure is possible. Widespread bullous-hemorrhagic erysipelas with extensive blisters should be considered severe in the absence of pronounced toxicosis and hyperthermia. With different localization of erysipelas, the clinical course of the disease and its prognosis have their own characteristics. Erysipelas of the lower extremities is the most common localization of the disease (60 - 70%). Characteristic are hemorrhagic forms of the disease with the development of extensive hemorrhages, large blisters with subsequent formation of erosions and other skin defects. For this localization of the process, the most typical lesions of the lymphatic system are lymphangitis, periadenitis, and a chronically relapsing course of the disease. The latter is largely facilitated by background concomitant conditions - chronic venous insufficiency, primary disorders of lymph circulation, mycoses, etc. Erysipelas (20 - 30%) is usually observed in primary and recurrent forms of the disease. With it, it is relatively rare that the disease often recurs. With timely treatment, facial erysipelas is easier than erysipelas of other localizations. It is often preceded by tonsillitis, acute respiratory diseases, exacerbations of chronic sinusitis, otitis media, and caries. Erysipelas of the upper extremities (5 - 7%), as a rule, occurs against the background of postoperative lymphostasis (elephantiasis) in women operated on for a breast tumor. Erysipelas of this localization in women has a tendency to recur. One of the main aspects of the problem of erysipelas as a streptococcal infection is the tendency of the disease to have a chronically relapsing course (in 25 - 35% of all cases). Relapses of erysipelas can be late
(occur a year or more after the previous outbreak of erysipelas with the same localization of the local inflammatory process), seasonal (occur annually for many years, most often in the summer-autumn period).
Late and seasonal relapses of the disease, usually the result of reinfection, do not differ in clinical course from typical primary erysipelas, although they occur against the background of persistent lymphostasis and other consequences of previous outbreaks of the disease. Early
and
frequent
relapses (3 relapses per year or more) are exacerbations of a chronic disease.
In more than 70% of patients, often recurrent erysipelas occurs against the background of various concomitant conditions, accompanied by disturbances in skin trophism, a decrease in its barrier functions, and local immunodeficiency. These include primary lymphostasis and elephantiasis of various etiologies, chronic venous insufficiency (postthrombophlebitic syndrome, varicose veins), fungal skin lesions, diaper rash, etc. Chronic ENT infection, diabetes mellitus, and obesity are of particular importance for the formation of recurrent erysipelas. The combination of two or three of the listed background diseases significantly increases the possibility of frequent relapses of the disease, and those suffering from them constitute a risk group. Complications
of erysipelas, mainly of a local nature, are observed in 5 - 8% of patients.
Local complications of erysipelas include abscesses, phlegmons, skin necrosis, pustulization of bullae, phlebitis, thrombophlebitis, lymphangitis, and periadenitis. Complications most often occur in patients with bullous hemorrhagic erysipelas. With thrombophlebitis, the subcutaneous and less often the deep veins of the leg are affected. Treatment of these complications must be carried out in purulent surgical departments. Common complications that develop in patients with erysipelas quite rarely include sepsis, toxic-infectious shock, acute cardiovascular failure, pulmonary embolism, etc. The consequences
of erysipelas include persistent lymphostasis (lymphedema) and secondary elephantiasis itself (fibredema), which are two stages of one process. According to modern concepts, persistent lymphostasis and elephantiasis in most cases develop in patients with erysipelas against the background of already existing functional insufficiency of lymph circulation of the skin (congenital, post-traumatic, etc.). Recurrent erysipelas that occurs against this background significantly enhances existing (sometimes subclinical) lymph circulation disorders, leading to the formation of consequences of the disease. Successful anti-recurrence treatment of erysipelas (including repeated courses of physical therapy) can lead to a significant reduction in lymphedema. In case of already formed secondary elephantiasis, only surgical treatment is effective.
Laboratory diagnostics
Due to the rare isolation of b-hemolytic streptococcus from the blood of patients and from the source of inflammation, conducting routine bacteriological studies is impractical. Elevated titers of antistreptolysin-O and other antistreptococcal antibodies, identification of bacterial and L-forms of streptococcus in the blood of patients have a certain diagnostic significance, which is especially important when predicting relapses in convalescents. Recently, polymerase chain reaction has begun to be used to diagnose streptococcal infections. In most patients with erysipelas, at the height of the disease, moderate neutrophilic leukocytosis with a shift to the left, aneosinophilia, and moderately increased ESR are usually observed. In patients with frequent relapses of the disease, leukopenia may occur. In severe cases of erysipelas and its purulent complications, hyperleukocytosis may be detected, sometimes with the development of a leukemoid reaction and toxic granularity of neutrophils. Changed hemogram parameters usually normalize during the period of convalescence. Changes in the T- and B-immune systems are most typical for the recurrent form of the disease. They reflect signs of secondary immune deficiency, usually occurring in the hypersuppressor mode. For patients with hemorrhagic erysipelas, pronounced disturbances of hemostasis and fibrinolysis are typical, manifested by an increase in the blood level of fibrinogen, PDP, RKMP, an increase or decrease in the amount of plasminogen, plasmin, antithrombin III, an increase in the level of platelet factor 4, and a decrease in their number. Moreover, the activity of various components of hemostasis and fibrinolysis varies significantly in individual patients.
Diagnostic criteria and differential diagnosis
Diagnostic criteria for erysipelas in typical cases are: • acute onset of the disease with severe symptoms of intoxication, increased body temperature to 38-39°C and above; • predominant localization of the local inflammatory process on the lower extremities and face; • development of typical local manifestations with characteristic erythema, possible local hemorrhagic syndrome; • development of regional lymphadenitis; • absence of severe pain in the area of inflammation at rest. Differential diagnosis for erysipelas should be carried out with more than 50 diseases related to the clinic of surgical, skin, infectious and internal diseases. First of all, it is necessary to exclude abscess, phlegmon, suppurating hematoma, thrombophlebitis (phlebitis), dermatitis, eczema, herpes zoster, erysipeloid, erythema nodosum.
Treatment
Treatment of patients with erysipelas should be carried out taking into account the form of the disease, primarily its frequency (primary, repeated, recurrent, often recurrent erysipelas), as well as the degree of intoxication, the nature of local lesions, the presence of complications and consequences. Currently, most patients with mild erysipelas and many patients with moderate forms of the disease are treated in a clinic. Indications for compulsory hospitalization in infectious diseases hospitals (departments) are: • severe erysipelas with severe intoxication or widespread skin lesions (especially in the bullous-hemorrhagic form of erysipelas); • frequent relapses of erysipelas, regardless of the degree of intoxication, the nature of the local process; • presence of severe common concomitant diseases; • old age or childhood. Antibacterial therapy occupies the most important place in the complex treatment of patients with erysipelas (as well as other streptococcal infections). When treating patients in a clinic and at home, it is advisable to prescribe antibiotics orally: erythromycin 0.3 g 4 times a day, oletethrin 0.25 g 4 - 5 times a day, doxycycline 0.1 g 2 times a day, spiramycin 3 million IU 2 times a day (course of treatment 7 - 10 days); azithromycin - on the 1st day 0.5 g, then for 4 days 0.25 g 1 time per day (or 0.5 g for 5 days); ciprofloxacin - 0.5 g 2 - 3 times a day (5 - 7 days); biseptol (sulfatone) - 0.96 g 2 - 3 times a day for 7 - 10 days; rifampicin - 0.3 - 0.45 g 2 times a day (7 - 10 days). In case of intolerance to antibiotics, furazolidone is indicated - 0.1 g 4 times a day (10 days); delagil 0.25 g 2 times a day (10 days). It is advisable to treat erysipelas in a hospital setting with benzylpenicillin in a daily dose of 6 - 12 million units, a course of 7 - 10 days. In severe cases of the disease, the development of complications (abscess, phlegmon, etc.), a combination of benzylpenicillin and gentamicin (240 mg once a day) and the prescription of cephalosporins are possible. For severe skin infiltration at the site of inflammation, non-steroidal anti-inflammatory drugs are indicated: chlotazol 0.1 - 0.2 g 3 times or butadione 0.15 g 3 times a day for 10 - 15 days. Patients with erysipelas need to be prescribed a complex of B vitamins, vitamin A, rutin, ascorbic acid, a course of treatment of 2 - 4 weeks. In case of severe erysipelas, parenteral detoxification therapy is carried out (hemodez, rheopolyglucin, 5% glucose solution, saline solution) with the addition of 5 - 10 ml of 5% ascorbic acid solution, 60 - 90 mg of prednisolone. Cardiovascular, diuretic, and antipyretic drugs are prescribed. Pathogenetic therapy of local hemorrhagic syndrome is effective with earlier treatment (in the first 3-4 days), when it prevents the development of extensive hemorrhages and bullae. The choice of drug is carried out taking into account the initial state of hemostasis and fibrinolysis (according to coagulogram data). In case of clearly expressed hypercoagulation phenomena, treatment with a direct-acting anticoagulant heparin (subcutaneous administration or by electrophoresis) and the antiplatelet agent trental at a dose of 0.2 g 3 times a day for 7 - 10 days is indicated. In the presence of pronounced activation of fibrinolysis in the early stages of the disease, it is advisable to treat with the fibrinolysis inhibitor Ambien at a dose of 0.25 g 3 times a day for 5 - 6 days. In the absence of pronounced hypercoagulation, it is also recommended to administer protease inhibitors - Contrical and Gordox - directly into the inflammation site by electrophoresis, for a course of treatment of 5 - 6 days.
Treatment of patients with recurrent erysipelas
Treatment of this form of the disease should be carried out in a hospital setting. It is mandatory to prescribe reserve antibiotics that were not used in the treatment of previous relapses. Cephalosporins (I or II generation) are prescribed intramuscularly at 0.5 - 1.0 g 3 - 4 times a day or lincomycin intramuscularly 0.6 g 3 times a day, rifampicin intramuscularly 0.25 g 3 times a day. The course of antibacterial therapy is 8 - 10 days. For particularly persistent relapses of erysipelas, two-course treatment is advisable. Antibiotics are consistently prescribed that have an optimal effect on bacterial and L-forms of streptococcus. The first course of antibiotic therapy is carried out with cephalosporins (7 - 8 days). After a 5-7 day break, a second course of treatment with lincomycin is carried out (6-7 days). For recurrent erysipelas, immunocorrective therapy (methyluracil, sodium nucleinate, prodigiosan, T-activin) is indicated.
Local therapy
Treatment of local manifestations of the disease is carried out only in its bullous forms with localization of the process on the extremities. The erythematous form of erysipelas does not require the use of local treatments, and many of them (ichthyol ointment, Vishnevsky balm, antibiotic ointments) are generally contraindicated. In the acute period of erysipelas, if there are intact blisters, they are carefully incised at one of the edges and after the exudate is released, bandages with a 0.1% solution of rivanol or a 0.02% solution of furatsilin are applied to the site of inflammation, changing them several times during the day. Tight bandaging is unacceptable. In the presence of extensive weeping erosions at the site of the opened blisters, local treatment begins with manganese baths for the extremities, followed by the application of the bandages listed above. For the treatment of local hemorrhagic syndrome with erythematous-hemorrhagic erysipelas, 5-10% dibunol liniment is prescribed in the form of applications in the area of inflammation 2 times a day for 5-7 days. Timely treatment of hemorrhagic syndrome significantly reduces the duration of the acute period of the disease, prevents the transformation of erythematous-hemorrhagic erysipelas into bullous-hemorrhagic, accelerates reparative processes, and prevents complications characteristic of hemorrhagic erysipelas.
Physiotherapy
Traditionally, in the acute period of erysipelas, ultraviolet radiation is prescribed to the area of inflammation in the area of regional lymph nodes. If skin infiltration, edematous syndrome, regional lymphadenitis persist during the convalescence period, ozokerite applications or dressings with heated naphthalan ointment (on the lower extremities), paraffin applications (on the face), lidase electrophoresis (especially in the initial stages of elephantiasis formation), calcium chloride, radon baths. Recent studies have shown the high effectiveness of low-intensity laser therapy for local inflammation, especially in hemorrhagic forms of erysipelas. Laser radiation is used in both the red and infrared ranges. The applied dose of laser radiation varies depending on the condition of the local hemorrhagic lesion and the presence of concomitant diseases.
Bicillin prevention of recurrent erysipelas
Bicillin prophylaxis is an integral part of complex dispensary treatment of patients suffering from a recurrent form of the disease. Prophylactic intramuscular administration of bicillin (5 - 1.5 million units) or retarpen (2.4 million units) prevents relapses of the disease associated with reinfection with streptococcus. While foci of endogenous infection persist, these drugs prevent the reversion of L-forms of streptococcus into the original bacterial forms, which helps prevent relapses. In case of frequent relapses (at least 3 in the last year) of erysipelas, continuous (year-round) bicillin prophylaxis is advisable for 2 - 3 years with an interval of drug administration of 3 - 4 weeks (in the first months the interval can be reduced to 2 weeks). In case of seasonal relapses, the drug is started to be administered a month before the start of the morbidity season in a given patient with an interval of 4 weeks for 3 to 4 months annually. If there are significant residual effects after erysipelas, the drug is administered at intervals of 4 weeks for 4 to 6 months. Clinical examination of patients with erysipelas should be carried out by doctors in the infectious diseases departments of polyclinics, with the involvement, if necessary, of doctors of other specialties.
Prevention of erysipelas on the leg
As you know, it is easier to prevent a disease than to treat it later. To protect yourself from infection, you need to lead the healthiest lifestyle possible, consume healthy foods, and avoid stressful situations. In this way, it will be possible to strengthen the immune system and reduce the risk of infection.
It is also necessary to maintain personal hygiene, pay close attention to washing your feet, avoid various injuries and injuries, and do not overcool your feet.
Erysipelas is a dangerous pathology. At the first symptoms of the disease, you should immediately seek medical help. This will not only protect the patient from deterioration of health and complications, but also protect others from infection.
Symptoms
You can notice the first symptoms of erysipelas on different parts of the body: legs, arms, face, torso, perineum. Moreover, much will depend on how exactly the disease develops. For example, inflammation on the face can be localized around the eye socket, near the ear, on the scalp and neck. If the disease starts from the nose, a butterfly-type lesion may develop - extending to the cheeks. At the same time, swelling occurs, which distorts the size of the tissue. The same applies to all other organs - the localization of the disease is different and depends on the situation.
Symptoms of erysipelas are divided into general and local. General points include:
- Chills, fever. Patients often shake violently.
- High temperature, up to 40 degrees. It can last up to ten days.
- Convulsions, clouding of consciousness, delirium.
- Very strong weakness, dizziness.
- Nausea, often vomiting.
- Pain in muscles and joints.
In other words, symptoms of general poisoning of the body are observed.
Local symptoms of erysipelas look like this:
- Redness of the skin at the site of the lesion. Usually changes are noticeable ten to twenty hours after the pathological processes begin.
- Puffiness, swelling, pain in the place where the skin rises. Also, the area of skin becomes warmer to the touch, even hot. The patient may feel a burning sensation and a sensation as if something is bursting the skin from the inside.
- Rapid growth of inflammation, since streptococci multiply quite actively. The edges of the lesions are uneven, they constantly change as they grow.
- Enlargement of nearby lymph nodes as the pathogen spreads through the lymphatic system.
- Bubbles with clear liquid. They are small at first, but then they grow and unite with each other. This sign is not always present.
- Hemorrhages. If you do not help the patient at first, complications will occur, including damage to the blood vessels, the blood of which enters the intercellular space.
- Bubbles with blood and pus surrounded by areas of hemorrhage. The classification of erysipelas suggests different degrees of development of the disease - and these manifestations are already characteristic of complicated forms.
The more advanced the situation, the higher the risks that even after successful treatment a relapse will occur. Often the disease occurs in the same place as the first time.
Diagnostics
If the first signs of erysipelas occur, you should consult a dermatologist or therapist. Depending on the extent of the problem, assistance from specialists such as an immunologist, surgeon, or infectious disease specialist may be required.
Diagnosis of the disease includes interviewing the patient, as well as a thorough examination. Then tests are prescribed for the level of T-lymphocytes, ESR, and the number of neutrophils (all this is determined through a blood test).
An optional bacteriological examination is prescribed to determine the causative agent - doctors do not agree on the advisability of such an examination.