Author:
- Elena Vitalievna Naumova, otolaryngologist, leading doctor of the clinic
5.00 (Votes: 2)
It is difficult to cure a sore throat without antibiotics, so otolaryngologists often supplement the usual treatment regimen with antibacterial drugs. Antibacterial drugs differ in chemical composition and mechanism of action, so only a specialist can choose the best drug. It is important to note that uncontrolled self-administration of antibiotics only harms the body - dysbiosis develops, and the causative agent of sore throat remains and develops resistance to the medication.
To prevent this, you should consult with an ENT doctor, get tested, and only then begin treating tonsillitis with antibiotics.
Indications for use
Tonsillitis, accompanied by the following clinical picture, requires antibiotics:
- A clear white coating on the tonsils, visible to the naked eye.
- Consistently high temperature (above 38°C).
- Enlarged lymph nodes near the neck.
Antibiotics are effective only for tonsillitis caused by bacteria - fusobacterium Fusobacterium necrophorum, group A streptococcus, beta-hemolytic streptococcus Streptococcus pyogenes, staphylococcus, aerobic and anaerobic bacteria. To verify the bacterial etiology of the disease, the ENT doctor gives a referral for a bacterial culture from the back of the throat.
Important to remember! If a bacterial pathogen is not confirmed, then antibacterial therapy is not needed - antibiotics have no effect against viruses.
Causes, main risk factors
Up to 30 different colonies of pathogenic microbes can be sown on the surface of the tonsils of patients suffering from chronic tonsillitis. But in crypts and lacunae staphylo- or streptococcus is usually determined. A key role in the pathogenesis of chronic tonsillitis is played by beta-hemolytic strains of streptococcus (type A). Other flora - gram-negative coccal, fungal, viral - have an impact on local immunity, they support inflammation.
There are a number of factors contributing to the occurrence of the disease:
- hypothermia;
- decreased immunity;
- microtrauma of the tonsils;
- foci of inflammation in the mouth and in the head area (caries, sinusitis, adenoids, etc.);
- smoking;
- poor nutrition;
- allergy.
Viruses and bacteria that cause tonsillitis can come from the external environment.
Features of antibiotic therapy in children
When treating tonsillitis in children, the ENT doctor prescribes predominantly local antibiotics, because Systemic medications have a detrimental effect on beneficial bacteria.
Basically, penicillin drugs or macrolides are used, since streptococcus or staphylococcus most often causes sore throat in children. The course of antibiotics is 7-10 days, and treatment cannot be stopped if the condition improves.
Important to remember! It is necessary to get tested before taking an antibiotic, because... symptoms of the initial stage of bacterial tonsillitis are similar to those of infectious mononucleosis.
Many parents are wary of taking antibiotics at a young age, but there is no need to worry. A properly selected drug prevents complications of tonsillitis such as rheumatic fever, purulent-inflammatory process, and peritonsillar abscess. The child tolerates the disease more easily and will not infect others.
It is important to know! If a child gets tonsillitis again, you should not take the same antibiotic again.
Severe stages of tonsillitis are treated with suspensions, an antibiotic in the form of a dry powder for oral administration.
Exacerbation of chronic tonsillitis: symptoms
Often, for a long time, chronic tonsillitis occurs without symptoms or has scanty symptoms (in a simple form). There may be discomfort when swallowing food and liquids, a sensation of a foreign body in the throat, dry mouth, halitosis (bad odor) and tingling. Externally, the tonsils increase in size and there are signs of inflammation. The disease is characterized by exacerbations of sore throats up to three times a year, long periods of recovery, with general symptoms of asthenia and prolonged low-grade fever.
For the toxic-allergic form, more frequent exacerbations are typical, often with complications in the area of neighboring tissues (pharyngitis, peritonsillar abscesses), and the almost constant presence of asthenia and prolonged fever are typical.
The clinical picture of chronic tonsillitis during an exacerbation is as follows:
- sore throat that gets worse when swallowing;
- redness of the throat and tonsils;
- characteristic plaque;
- purulent discharge from the tonsils;
- bad breath;
- swelling of the nasopharynx;
- temperature increase;
- weakness;
- headache;
- fast fatiguability;
- arrhythmia;
- enlarged lymph nodes;
- dyspnea.
Features of antibiotic therapy in adults
Most often, an otorhinolaryngologist prescribes tetracycline or penicillin antibiotics. Acute pain goes away within 12 hours after the first dose of the drug. If the effect is not noticeable after 2-3 days, then the doctor prescribes a second-generation antibiotic from the group of cephalosporins or lincosamides. For tonsillitis caused by Staphylococcus aureus, third generation aminoglycosides are effective. Depending on the severity of the disease, the ENT doctor prescribes the drug in tablet form or by injection.
The course of treatment is 7-10 days. The doctor individually indicates the frequency of administration, dosage and name of the medication in accordance with the symptoms, age, and weight of the patient.
Antibiotics prevent the accumulation of purulent exudate in the lacunae of the tonsils and its further spread through the respiratory tract. For the treatment of adults, local antibiotics complement general therapy.
Therapeutic tactics for tonsillitis
If we consider that chronic tonsillitis is only a long-term inflammatory process in the tonsils, then it is unlikely that this disease should have received so much attention from other medical specialties. Therefore, the very definition of tonsil disease as chronic tonsillitis requires clarification. This will make the motivation for different types of conservative or surgical treatment clearer. So, chronic tonsillitis is a process of constant interaction between lymphoid tissue and the contents of the lacunae of the palatine tonsils (purulent detritus with elements of foreign protein, toxins as a result of the vital activity of pathogenic flora, microorganisms themselves, dead epithelial cells from the walls of the lacunae of the palatine tonsils, nutritional particles). The discharge in the lacunae can be purulent, caseous, accumulate in narrow lacunae convoluted with spurs, and form so-called fetid plugs. This process, which takes place in the lacunae of the palatine tonsils, is under the control of the body until a certain time, i.e. There is constant active and passive drainage of tonsil lacunae along with the activity of macrophages, which, preventing inflammation of the palatine tonsil, contributes to the development of immunity to many microorganisms that enter the oral cavity and pharynx along with air and food.
This kind of balance between the vital activity of pathogenic active flora and the protective capabilities of the body can be disturbed for many reasons, as a result of which inflammation of varying intensity develops (it captures only the covering epithelium of the oral surface of the tonsils without its destruction), which passes to the epithelial cover of the lacunae of the tonsils with its destruction and formation necrotic plaques; suppuration of the tonsil follicles. Catarrhal, lacunar or follicular tonsillitis develops
.
In foreign literature, they tend to combine two diseases of the oropharynx and designate inflammation of the tonsils and pharyngeal mucosa as “tonsillopharyngitis.” However, experts in Russia quite reasonably believe that such a combination of two nosological units is possible only in cases of a combination of acute catarrhal pharyngitis and catarrhal tonsillitis. Lacunar and follicular tonsillitis have their own clearly defined clinical, morphological and microbiological aspects
, and they cannot be confused with manifestations of pharyngitis, especially from the point of view of the approach to treatment.
According to modern concepts, angina is an acute infectious-allergic disease, and it is necessary to approach the treatment of a patient with angina from this point of view.
As was said, the presence and persistent preservation of purulent detritus in the lacunae of the palatine tonsils is a determining factor both in making the diagnosis of “chronic tonsillitis” and in choosing the appropriate method of treatment - conservative or surgical.
A sore throat with destruction of the integumentary epithelium of the lacunae promotes the formation of scars in their lumen, which subsequently complicates the drainage of the lacunae of the tonsils. A kind of vicious circle arises - sore throat develops under the influence of pathogenic flora against the background of sensitization by a foreign protein due to a violation of the epithelial cover of the lacunae. Moreover, a sore throat can occur both under the influence of a pathogenic infection and as a result of nonspecific irritation (general hypothermia, drinking cold water).
Each previous angina, especially lacunar, follicular, can contribute to the development of conditions for relapse of inflammation, accompanied by otitis, sinusitis, and bronchitis.
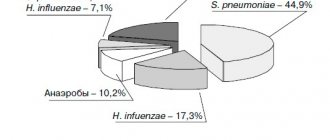
The main reason for this is the viruses that cause most respiratory tract infections, which can weaken the body's defenses. Viruses reduce the ability of macrophages and granulocytes to absorb infectious agents. In this way, the epithelium of the mucous membrane is damaged, which impedes the activity of the epithelial villi and leads to stagnation of mucus. Weakening of local protective mechanisms in many cases leads to infection of the upper and lower respiratory tract with bacteria Haemophilus influenzae, Streptococcus pneumoniae and Staphilococcus aureus, which are usually found in the oral cavity and trachea.
The chronic nature of infections is an indicator that the body's immune system is unable to cope with its functions. Constant but insufficient activation of nonspecific defense mechanisms often causes an inflammatory response, but this is not enough to suppress infectious agents.
Undoubtedly, the nature of the pathogenic flora plays a big role in the occurrence of a particular sore throat,
but the background against which it occurs also influences the clinical picture of the disease. Therefore, therapy should be prescribed and carried out taking into account all identified features in each case (time from the onset of angina, age of the patient, frequency of exacerbations, concomitant diseases: general and from the ENT organs, clinical manifestations, including in the oropharynx, nature of the flora , previous treatment, its effectiveness).
Currently, much attention is paid to the role of group A streptococcus in the occurrence of acute tonsillitis and pharyngitis, although b-hemolytic streptococcus still occupies a leading position among bacterial pathogens. Thus, it is believed that in late autumn and spring it is group A streptococci that cause disease in 40% of children and 10% of adults. Along with this, there is an opinion that in the vast majority of cases, the incidence of the lymphadenoid ring of the pharynx in children is determined by a viral infection, the features of which are a protracted and recurrent course, insufficient effectiveness of conservative anti-inflammatory measures, and a tendency to hyperplasia of the palatine and pharyngeal tonsils. Usually, the doctor diagnoses a sore throat “by eye,” only on the basis of clinical experience, and prescribes antibacterial treatment without taking into account the advisability of antiviral therapy. This not only slows down the healing process, but can also contribute to a decrease in the protective properties of the pharyngeal mucosa, since under the influence of antibiotics a-hemolytic streptococcus, which produces bactericin, a natural antibiotic, disappears. It is penicillins
to a greater extent than cephalosporins, they suppress this beneficial flora of the oropharynx and allow pathogenic streptococci to take its place on the epithelium of both the tonsils and the entire pharynx. Therefore, irrational (too early and without taking into account the flora) prescription of antibiotics leads to a decrease in antibacterial immunity and contributes to relapses of sore throat.
Based on the foregoing, the treatment tactics for patients with acute and chronic tonsillitis should consist of an accurate determination of the nature of the inflammatory process (acute, exacerbation of chronic or its sluggish course), justification of the type of inflammation (catarrhal, purulent, phlegmonous), determination of the type of pathogen (streptococcus, spirochete, bacillus , virus, mushrooms). To this it is necessary to add that all sore throats can be divided into two groups
- primary tonsillitis, as a self-developing acute inflammatory process in the tonsils, and secondary tonsillitis, as a symptom of the underlying disease, for example, in blood diseases. Only the correct diagnosis, taking into account the general condition of the patient, determines the choice of treatment tactics.
Acute sore throat
Catarrhal tonsillitis is the mildest form of tonsillitis, which affects the mucous membrane of the tonsils, sometimes in combination with inflammation of the mucous membrane of the oropharynx (mainly the area of its posterior wall), which gives a mixed picture of tonsillitis and pharyngitis. The main complaint is pain when swallowing food and saliva (with pharyngitis, swallowing saliva is more painful - “empty swallow”). The general condition is satisfactory, the disease lasts 6-7 days, body temperature is within the subfebrile range. Treatment involves the widespread use of physiotherapeutic procedures, frequent rinsing with warm disinfectant solutions, a gentle diet, plenty of warm drinks, and the use of salicylates. Prescribing antibiotics for identified catarrhal tonsillitis is considered inappropriate, especially without a clear idea of the causative agent
.
Due to the fact that even without the use of antibiotics all the symptoms of the disease disappear quite quickly (on the 2-3rd day), early prescription of antibiotics in cases of catarrhal tonsillitis leads to the fact that patients stop taking them without observing the course dose. In addition, complete suppression, for example, by phenoxymethylpenicillin, amoxicillin (the most commonly used antibiotics), group A streptococci (and with them a-hemolytic streptococcus, which resists pathogenic flora) leads to the fact that the person returning to the normal environment (home, school and etc.) the recovered patient again encounters this flora, but already capable of transmission, i.e. the possibility of relapse of inflammation of the tonsils increases - natural immunity is suppressed. When prescribing antibiotics in the first days of a sore throat, it is also necessary to remember about the possible resistance of a number of strains of streptococci to the prescribed antibiotics, for example, to macrolides such as erythromycin, clarithromycin. Therefore, the most rational prescription of antibiotics in the treatment of mild forms of sore throat is after laboratory confirmation of the sensitivity of the flora to them
. These provisions are classics, but in practice, for many reasons, they are not always observed, which will ultimately lead humanity to complete disarmament in the face of transforming strains of pathogens, including those that cause sore throat.
Severe forms of angina - lacunar, follicular
- require the prescription of antibiotics, but also in compliance with the rules for combating infection and taking into account all factors: diagnosis, flora, somatic status, the need to prevent complications, the full course of taking an antibiotic.
Chronic tonsillitis
What are the treatment tactics for recurrent tonsillitis, recurring 2 times a year or more often?
In these cases, the disease is defined as “chronic tonsillitis,” however, for it, the frequency of relapses of tonsillitis may not always be the determining factor, since the concept of “chronic tonsillitis” also includes other parameters that support the diagnosis. These are, first of all, complications clearly associated with it from other organs and systems of the body.
For a practicing physician, both a general practitioner and an otorhinolaryngologist, after making a diagnosis of “chronic tonsillitis,” it is important to choose the tactics of treating the patient and decide the question: in which cases is surgery indicated, and in which - conservative therapy.
We divide chronic tonsillitis into only two forms: chronic tonsillitis I and chronic tonsillitis II
. In the first case, conservative treatment is required, in the second - surgical treatment. The determining factor is the combination of local signs of tonsillitis with complications and features of the course.
Conservative treatment
Conservative treatment involves, first of all, systematic sanitation of the lacunae of the palatine tonsils while preserving the lymphoid tissue of the tonsils.
as an immune, to a certain extent, organ. Conservative treatment is indicated for uncomplicated chronic tonsillitis in cases where surgery can be delayed due to the general condition of the patient; if the patient has not previously received any therapy or is mainly concerned about local manifestations of tonsillitis - purulent plugs in the tonsils, bad breath, etc.
Among the methods of conservative treatment for chronic tonsillitis, the most effective are the following: washing the lacunae of the tonsils and removing purulent plugs and detritus (carrying out repeated courses using the “Tonsilor” apparatus, when simultaneously washing the lacunae of the tonsils with a disinfectant solution, suctioning out the pathological contents from them and ultrasonic exposure with low-frequency ultrasound on the tonsil tissue), as well as the introduction of various medications into the tonsil using phonophoresis. Physiotherapeutic treatment – KUF, “Yakhont-F”.
Both for sore throat and for accompanying pharyngitis, gargling, inhalation, and irrigation of the mucous membrane with disinfectant solutions are indicated.
Increasing the effectiveness of treatment can be achieved by prescribing immunostimulating plant extracts. Tonsilgon N
is a combination preparation of plant origin. The chamomile, marshmallow and horsetail components included in its composition stimulate the body's defense mechanisms by increasing the phagocytic activity of macrophages and granulocytes. The drug has anti-inflammatory, immunostimulating, anti-edematous and antiviral effects, accelerates the healing process and shortens the duration of the disease; can be used in the future to prevent relapse of the disease. There were no side effects when using the drug.
Tonsilgon N is available in two forms: in the form of drops for oral administration and in the form of tablets. For adults, the drug is prescribed 25 drops or 2 tablets 5-6 times a day, for children under 5 years old - 5-10 drops, for children 5-10 years old - 15 drops, for teenagers 10-16 years old - 20 drops 5-6 times a day. day. After the disappearance of acute manifestations of the disease, the frequency of taking Tonsilgon N is reduced to 3 times a day. The duration of basic therapy is 4-6 weeks.
The prescription of systemic antibiotic therapy for uncomplicated forms of tonsillitis of non-streptococcal etiology is not always justified. In this case, local prescription of antimicrobial drugs is more rational (from the first day of the disease until the results of a microbiological study are obtained). The main requirements for local antibacterial agents are a wide spectrum of antimicrobial action, including the most typical pathogens, lack of absorption from the mucous membrane, and low allergenicity.
Fusafyungin (Bioparox) has the most optimal combination of the above requirements.
- inhaled antibiotic with anti-inflammatory properties. The wide spectrum of antibacterial action of fusafyungin, the absence of resistant strains of microorganisms, and the drug’s own anti-inflammatory properties make it especially effective in the treatment of tonsillitis of non-streptococcal etiology. The most optimal is to use 4 doses of the drug every 4 hours for 10 days.
Other drugs used in the treatment of sore throats and exacerbations of chronic tonsillitis are:
Clarithromycin
- 1 tablet 2 times a day.
Coldrex
- 2 tablets 2 times a day. Children 6-12 years old - 1 tablet 4 times a day.
Tonsillotren
(lozenges) - 1 tablet every hour.
Treatment of tonsillitis such as agranulocytic and monocytic requires the participation of a hematologist.
Surgery
Indications for surgical intervention:
1. Frequent (2-4 times a year) sore throats, accompanied by high body temperature; pathological purulent detritus is noted in the lacunae; there is one or another complication associated with an exacerbation of the process (polyarthritis, pyelonephritis, etc.).
2. Frequent sore throats (2-4 times a year or more often), accompanied by high body temperature, local signs of chronic tonsillitis are observed, without identified complications. Frequently recurring sore throats indicate a weakened immune system.
3. As a result of one of the rare cases of tonsillitis (once every 5-7 years), some complication of the heart, joints, etc. developed. Local signs of chronic tonsillitis, adenitis of the lymph nodes in the area of the angle of the lower jaw.
4. There were no cases of tonsillitis, however, against the background of emerging diseases of the heart, joints, etc., local signs of chronic tonsillitis are revealed, mainly the accumulation of purulent contents in the lacunae of the tonsils.
Fuzafyungin –
Bioparox (trade name)
(Servier)
Combined preparation of herbal origin –
Tonsilgon N (trade name)
(BIONORICA Arzneimittel GmbH)
| Applications to the article |
| Chronic tonsillitis is a process of constant interaction between lymphoid tissue and the contents of the lacunae of the palatine tonsils. |
| After making a diagnosis of chronic tonsillitis, it is important to choose a treatment strategy for the patient and decide the question: in which cases is surgery indicated, and in which - conservative therapy. |
Complications of chronic tonsillitis
Against the background of a chronic inflammatory process in the tonsil area, various complications are possible. Therefore, it is important to know why chronic tonsillitis is dangerous. Thus, the tonsils themselves, losing their function as a barrier to infection, become its breeding ground. Inside them are pathogens with the products of their metabolism. The infection can spread throughout organs and tissues, affecting the renal parenchyma, joint and heart tissue, and liver. In addition, tonsillitis adversely affects the functioning of the immune system and can be a provocateur of collagen diseases - lupus, scleroderma, dermatomyositis, periarteritis. The skin and peripheral nerve fibers may also be affected. With prolonged intoxication against the background of the disease, damage to blood vessels (vasculitis) and platelets (purpura) is possible.
Diagnosis of acute tonsillopharyngitis
If there are signs of streptococcal infection, the diagnosis is confirmed by a positive microbiological test (rapid test for the detection of GABHS antigen or a throat swab for GABHS). A test or smear should be performed before starting antibiotic therapy, as even a single dose of antibiotics can lead to a negative result.
Rapid tests for GABHS have a specificity of more than 95% and a sensitivity that varies between 70 and 90%. Given the high specificity and limited sensitivity of the available tests, a positive test for GABHS is sufficient to establish the diagnosis of streptococcal pharyngitis, but a negative test, in turn, does not exclude GABHS infection. Therefore, in a child or adolescent, in case of a negative result of the rapid test, it is necessary to perform a throat smear for GABHS. If the rapid test is positive, then subsequent bacteriological examination is not required.
In adults, with a negative rapid test in a standard situation, subsequent microbiological testing is not required.
A test for GABHS is indicated in the following cases:
- there are signs of acute tonsillopharyngitis (erythema, swelling and/or exudate in the tonsils) or a scarlet rash, but there are no symptoms of a viral infection;
- there was contact with a sick person whose diagnosis of streptococcal infection was confirmed (at home, at school);
- suspicion of acute rheumatic fever or post-streptococcal glomerulonephritis.
GABHS testing is not indicated for children and adolescents with manifestations of a viral infection. From 5 to 21% of children aged 3-15 years are carriers of GABHS, which can be mistakenly perceived as streptococcal rather than viral pharyngitis.
Timely treatment of GABHS in children and adolescents is primarily necessary for:
- prevention of purulent complications and acute rheumatic fever;
- preventing transmission of the disease to others, especially if the patient is in contact with a person who has had a history of an episode of acute rheumatic fever;
- reducing the duration and severity of symptoms of the disease.
General recommendations
Rest, adequate fluid intake, gentle nutrition, it is advisable to avoid irritation of the respiratory tract. Most patients can return to work or school after completing one full day of treatment, provided their general health allows it.
The recommendation is based on a small cohort study in children that showed that about 80% of patients with culture-proven streptococcal pharyngitis were no longer infectious within 24 hours of starting therapy.
A follow-up rapid test for streptococcus after treatment is usually not required and is indicated only in the following cases:
- patients with a history of acute rheumatic fever;
- patients who became ill during an outbreak of acute rheumatic fever or post-streptococcal glomerulonephritis;
- patients who became infected from close relatives (in the family).
If the control test is positive, it is recommended to repeat the 10-day course of antibiotic therapy. For the second course of treatment, an antibiotic is selected that is more stable against beta-lactamase degradation.