Local therapist
Burnatskaya
Svetlana Nikolaevna
33 years of experience
Local therapist, occupational pathologist. Member of the Russian Scientific Medical Society of Therapists
Make an appointment
Breathing problems and the sensation of a foreign body in the throat can be signs of developing asphyxia. Asphyxia belongs to the category of life-threatening conditions that lead to circulatory and respiratory disorders. Regardless of the causes, asphyxia requires urgent measures, since death is possible as a result of the development of acute oxygen starvation within a few minutes.
The basis for the development of asphyxia can be:
- damage to the respiratory muscles;
- the presence of an obstruction that does not allow air to enter the lungs;
- dysfunction of the respiratory center.
In recent years, doctors have had to deal with such a pathology as autoerotic asphyxia, which occurs as a result of sexual experiments.
General information about the disease
Asphyxia is diagnosed in 4-6% of children. Moreover, the percentage varies depending on the degree of prematurity of the fetus. In babies born before 36 weeks, the incidence of pathology reaches 9%, and in children born after 37 weeks it decreases to 1-2%.
Scientific definitions of newborn asphyxia boil down to the fact that the child cannot breathe independently or makes superficial convulsive breathing movements that do not allow the body to receive sufficient oxygen. The authors consider infant asphyxia as suffocation, in which other signs that the fetus is alive remain: there is a heartbeat, the umbilical cord is pulsating, the muscles are weak but contracting.
The reasons for the development of newborn asphyxia include a complex of risk factors that disrupt the blood circulation and respiratory functions of the fetus in the womb and during birth. The most common reasons include:
- conflict of Rh blood between mother and child;
- abnormal fetal development;
- pathologies of the nervous system in a baby;
- circulatory disorders, heart disease in the baby;
- intracranial injury that the baby received during the birth process;
- infections affecting the fetus in the womb (chlamydia, herpes, rubella, etc.);
- extragenital pathologies of the mother (thyrotoxicosis, anemia, diabetes mellitus);
- infectious diseases in the second and third trimesters;
- complicated childbirth;
- premature or post-term pregnancy;
- bad habits of the mother (effects of alcohol, nicotine, drugs on the body);
- malnutrition during pregnancySource: Asphyxia of newborns. Zhetpisova L.B. West Kazakhstan Medical Journal, 2011.
The most common cause of asphyxia is intrauterine hypoxia, that is, the baby lacks oxygen in the womb.
Whatever the causes of the pathological condition, it causes the same processes in the child:
- disrupts metabolism and blood circulation;
- thickens and increases blood viscosity;
- damage is caused to the brain, liver, heart, adrenal glands;
- organs swell, bleeding occurs;
- disruptions in the functioning of the central nervous system occur.
The longer the body feels a lack of oxygen, the more serious the degree of damage to tissues, organs and systems becomes.
Main signs and symptoms
The most obvious diagnostic sign is respiratory distress. It is this that subsequently leads to disruption of the cardiovascular system, weakening of the child’s muscle tone and reflexes.
Clinical manifestations of moderate asphyxia:
- lethargy, weakness;
- decreased motor activity;
- weak reactions;
- depressed reflexes;
- low-emotional cry;
- tachycardia;
- arrhythmic breathing, sometimes with wheezing;
- the skin is bluish, but can quickly turn pink.
The child's condition is considered moderate. During the first 2-3 days of life, he is in a state of increased excitability, which can be replaced by a syndrome of depression, weakness, and lethargy. The condition manifests itself as small tremors of the arms and legs, disturbed sleep, and weak reflexes.
In severe asphyxia, the clinical picture includes:
- lack of cry at birth;
- reflexes are severely depressed or sharply reduced;
- the skin is bluish, pale, with a “marble pattern”;
- breathing is shallow, arrhythmic and periodically absent;
- wheezing is heard in the lungs;
- the heartbeat is weak, dull;
- convulsions.
If acute severe asphyxia is successfully overcome, breathing normalizes within 2-3 days and reflexes are restored. Source: Fetal hypoxia and asphyxia of the newborn. Kuznetsov P.A., Kozlov P.V. General Medicine, 2021. p. 9-15.
Types of newborn asphyxia
Classification is carried out according to several criteria. First of all, depending on the time of development of the pathological condition, the following are distinguished:
- primary, or intrauterine asphyxia - develops directly in the womb;
- secondary, or extrauterine asphyxia – occurs in the first hours of the baby’s life.
In turn, primary asphyxia is also divided into two subtypes:
- antenatal, or chronic - develops even before the onset of labor;
- intrapartum, or acute - occurs during the period of uterine dilation and fetal birth.
How to properly provide first aid for asphyxia?
Whether pre-medical first aid is provided for asphyxia determines whether a person will survive and how much his health will suffer.
What to do if you are choking?
While the ambulance is traveling, you should try to provide first aid yourself. There are few options for action. All of them are aimed at eliminating the cause of suffocation. Accordingly, depending on the reason, certain steps should be taken.
- Asphyxia: description of the condition, types of illness, main symptoms and consequences
If the victim is conscious?
If a person is conscious, it means there is still time to try to correct the situation:
- Explain to the victim that he should not inhale deeply and sharply, but that he should exhale and clear his throat intensively, trying to push out the object that is interfering with breathing with air pressure.
- Sit or position the person so that breathing is less uncomfortable.
- For obstructive syndrome, use mechanical methods (described below).
What if the victim lost consciousness?
In cases where the flow of air in the respiratory tract has stopped due to compression (i.e. physical suffocation), first aid for asphyxia involves freeing the neck from the compressive object.
As a rule, after violent strangulation, a person is unconscious and there is no breathing. The heart may continue to beat for 5-15 minutes even if breathing has stopped. Therefore, first of all, if the victim has lost consciousness, then he is placed on his right side, the pulse in the carotid artery is checked or the heartbeat is listened to by placing the ear in the chest.
If heartbeats are heard, then when providing first aid for asphyxia, they are guided by the following algorithm:
- The victim is turned over on his back;
- the head is thrown back a little;
- the lower jaw is pushed forward;
- open the mouth (use a spoon if necessary);
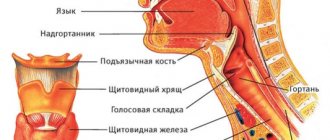
- check to see if the tongue is stuck and does not block the throat;
- if the tongue interferes with the passage of air, then take a piece of cloth or a napkin and forcefully pull the tongue out (this may not be easy, use a spoon to change the position of the root of the tongue).
After this, artificial respiration begins:
- The victim's mouth is covered with a handkerchief;
- the lips of the person being resuscitated are in close contact with the area around the mouth of the person being resuscitated, the nose is pinched;
- a strong, deep exhalation is made so that the victim’s chest rises slightly (raising the chest shows that artificial respiration is being done correctly);
- The victim exhales independently.
Forced inhalation lasts 3 s, exhalation – 1-2 s. The number of cycles per minute is 12-15.
Artificial respiration continues until the person being resuscitated shows signs of breathing on their own or until emergency assistance arrives.
After the victim has even the slightest signs of his own respiratory activity, artificial respiration is not stopped. External support is continued through 1 respiratory cycle until breathing returns to normal. In cases where the tongue does not allow mouth-to-mouth breathing, the mouth-to-nose scheme is used according to a similar algorithm.
For acute respiratory failure
With the development of respiratory failure caused by chronic diseases, the person is usually placed in a horizontal position on the right side. Another position is possible in which the patient can breathe most easily. Depending on the chronic pathology, medications are given to alleviate the condition.
- Asphyxia of newborns: causes, diagnosis, emergency care, consequences
In the presence of obstructive syndrome
Obstruction in the context of suffocation is the blocking of the air passage by an object that accidentally enters the respiratory tract. If mechanical suffocation is caused by a foreign object, then several methods of first aid for asphyxia are used.
- Standing
This is the main method of first aid for asphyxia, which is known to everyone, if not from personal experience, then at least from films. A person is grabbed “from behind” with hands held “in a lock” (i.e. one hand in a fist, the second hand clasps the fist so that the position of the arms is perpendicular to each other) in the area slightly above the navel and below the ribs.
In order for the procedure to be successful and effective, the shoulders of the person providing first aid for asphyxia must be lower than the shoulders of the person receiving assistance. That is, the victim should be lifted, as it were, in the arms of the person helping him. Or, conversely, the helper should sit down a little to become lower than the victim.
A series of fast, rhythmic pressures are applied with force, making sure that the main force comes from the pressure of a clenched fist at the point where the thumb comes into contact with the victim’s body. A series of pressures is repeated several times with 5-10 second breaks between them.
- Lying down
If the victim has a lot of weight, then it is often impossible to effectively perform the actions described above in a standing position. In order to provide first aid for asphyxia in this case, you can use the method in a lying position.
The person is placed on his back. The place where force is applied is the same as in a standing position: the upper abdomen in the center directly below the ribs. The fist is placed on this area, the second hand presses the fist. A series of rapid back-and-forth movements are made in an inward and upward direction, i.e. at an angle of approximately 45 0C to the horizontal plane.
- Face down and head tilted
An alternative option is to place the person face down so that the head is lower than the chest. Then, with rhythmic strong movements tangentially (i.e., not at a right angle), the area between the shoulder blades is struck several times.
- In a sitting position
The same method No. 3, but with less efficiency, can be used when a person is in a sitting position. We all know from childhood that if a person chokes at the table, then he should be tapped on the back in the area of the shoulder blades. This is exactly the maneuver that should be used, only do it more intensely so that it is not “tapping”, but a shaking of the chest.
The above-described methods of first aid for asphyxia can increase intrathoracic and intra-abdominal pressure, change the spatial location of a foreign body inside the respiratory tract and promote its release to the outside.
With increasing asphyxia and acute disturbances of external respiration
If the dynamics of suffocation are negative and resuscitation efforts are ineffective, prompt hospitalization is required. Attempts to restore breathing should not stop until doctors arrive.
- Fluid under the skin on the knee after a bruise or injury: symptoms, first aid and treatment
What NOT to do in case of suffocation (asphyxia)?
- If the cause of suffocation is a foreign object, then the victim should not be given anything to drink until the object is removed.
- The victim, who is in a lying position, should not place pillows or other objects under his head that change the angle of the head relative to the body.
- You should not perform artificial respiration if it is known that the cause of suffocation is obstruction of the respiratory passages by an object that was not removed.
The video shows techniques for assisting with obturation
Classification of asphyxia according to the Apgar scale
To assess the severity of asphyxia in a newborn, the Apgar scale is used. With its help, the doctor evaluates heart rate, breathing, muscle tone, skin color and reflexes, and then determines the severity of the pathological condition.
To give a rating, the doctor evaluates each of the five signs as 0, 1 or 2 points. Accordingly, the maximum and best score is 10 points. The assessment is determined taking into account the following criteria:
| Sign | 0 points | 1 point | 2 points |
| Pulse, beats per minute | No | Up to 100 | From 100 and above |
| Breath | No | Irregular, weak | Active, child screams and cries |
| Muscle tone | Arms and legs dangling | Weak flexion of arms and legs | Active movements |
| Reflexes | No | Weak | Present, well expressed |
| Color of the skin | Pale, cyanotic | Body – pink, arms and legs – bluish | Pink body, limbs |
The condition is assessed in the first and fifth minutes of life. Accordingly, the child receives two ratings: for example, 8/10. If the score is 7 or lower, the baby’s condition is assessed additionally at the 10th, 15th and 20th minutes.
Depending on the Apgar score, the degree of asphyxia is determined:
- 1-3 points – heavy;
- 4-5 points – average;
- 6-7 points – mild or moderate.
The Apgar score is not highly sensitive. Therefore, if a child has abnormalities, additional diagnostics are necessary to assess asphyxia.
How to sign up
To make an appointment with a doctor at our clinic, you can use any of the following methods:
- online form on the website;
- by phone +7 (495) 775-73-60;
- through your Personal Account or Mobile Application.
If necessary, you can get emergency help by phone.
JSC "Medicine" (clinic of academician Roitberg) is located in the center of Moscow at the address 2nd Tverskoy-Yamskaya lane, building 10. The clinic is located near the metro stations "Mayakovskaya", "Tverskaya", "Chekhovskaya", "Belorusskaya".
Diagnostics
Asphyxia can be diagnosed during gestation (primary, or intrauterine) by:
- monitoring of fetal heart rate, which is carried out during cardiotocography;
- analysis of motor activity, breathing and muscle tone of the fetus, which is carried out during ultrasound examination.
In case of secondary or extrauterine asphyxia, the diagnosis is made taking into account the presence of signs of a pathological condition, the external condition of the baby, the severity of the lack of oxygen and further tests that are carried out after completing the emergency care algorithm for the child.
For diagnosis use:
- Apgar score;
- a blood test from the scalp, vessels of the fetal umbilical cord, during which the oxygen tension, carbon dioxide tension and blood acidity are determined.
In some cases, an ultrasound examination of the brain is also prescribed, which determines how much the central nervous system is affected. The examination also makes it possible to distinguish hypoxic damage to the nervous system from traumatic one.
Damage and traces characteristic of mechanical asphyxia
The strangulation groove (mark) from hanging is characterized by clarity, unevenness, and openness (the free end of the loop is not pressed against the neck); shifted to the top of the neck.
The groove from violent strangulation with a noose runs along the entire neck without a break (if there were no interfering objects, such as fingers, between the noose and the neck), is uniform, often non-horizontal, accompanied by visible hemorrhages in the larynx, as well as in places where knots, rope overlaps are located, and is located closer to the center of the neck.
Traces from hand strangulation are scattered throughout the neck in the form of hematomas in places of maximum compression of the neck with fingers and/or in places where folds and pinched skin form. Nails leave additional marks in the form of scratches.
When strangling with the knee, as well as pinching the neck between the shoulder and forearm, there is often no visual damage to the neck. But criminologists easily differentiate these types of strangulation from all others.
With compression asphyxia, due to large-scale disturbances in the movement of blood, severe blue discoloration of the face, upper chest, and limbs of the victim is observed.
Treatment
Clinical recommendations for asphyxia include the provision of first aid to the newborn as a priority. This is the most important step, which, if carried out competently, reduces the severity of the consequences of the pathological condition and the risk of complications. The key goal of resuscitation measures for asphyxia is to achieve the highest possible Apgar score by 5-20 minutes of the newborn’s life.
The stages and principles of ABC resuscitation allow for consistent and effective resuscitation of a newborn born with asphyxia. Source: Carrying out therapeutic hypothermia in newborns born with asphyxia. K. B. Zhubanysheva, Z. D. Beisembaeva, R. A. Maykupova, T. Sh. Mustafazade. Science of Life and Health, 2021. p. 60-67:
- Principle A (“airway”) is to ensure a clear airway during the first stage of resuscitation. To do this, you need to create the correct position: tilt your head back, lower it 15 degrees. After this, suck out mucus and amniotic fluid from the nose, mouth, trachea, and lower respiratory tract.
- Principle B (“breath”) – create ventilation, provide breathing. To do this, a jet oxygen flow is created - artificial ventilation of the lungs is performed using a resuscitation bag. If the child does not cry, tactile stimulation is added: stroking along the back, patting the feet.
- Principle C (“cordial”) – restore heart function. Indirect cardiac massage helps with this. If necessary, adrenaline, glucose, hydrocortisone and other drugs are administered. In this case, the auxiliary ventilation from the previous stage cannot be stopped.
Care for a newborn child who has suffered asphyxia is carried out in a maternity hospital. Babies with a mild form are placed in a special tent with a high oxygen content. In cases of moderate or severe asphyxia, infants are placed in an incubator - a special box where oxygen is supplied. If necessary, the airways are re-cleaned and freed from mucus.
The scheme of further treatment, recovery and care is determined by the attending physician. General care recommendations include:
- maintaining normal body temperature, blood pressure, heart rate;
- creating maximum comfort: optimal ambient temperature, comfortable position;
- carrying out respiratory therapy;
- conducting infusion therapy - administering fluid to meet needs Source: Protocol for therapeutic hypothermia for children born with asphyxia. Ionov O.V., Balashova E.N., Kirtbaya A.R., Antonov A.G., Miroshnik E.V., Degtyarev D.N. Neonatology: News. Opinions. Training, 2014. p. 81-83.
During rehabilitation, regular monitoring :
- baby's weight (twice a day);
- neurological and somatic status;
- volume of fluid consumed;
- nutrition composition;
- basic vital signs: pulse, blood pressure, saturation, respiratory rate;
- laboratory characteristics of blood, urine;
- X-rays of the chest, abdominal cavity;
- ultrasound examination of the abdominal cavity;
- neurosonography;
- electrocardiograms, echocardiograms.
After discharge, the baby should be regularly monitored by a pediatrician or neurologist.
Mechanical asphyxia - what is it?
For the diagnostic classification of diseases associated with strangulation, the International Classification of Diseases, Tenth Revision, is used. Mechanical asphyxia ICD 10 has code T71 if suffocation occurs due to compression (strangulation). Strangulation due to obstruction – T17. Compression asphyxia due to crushing by earth or other rocks – W77. Other causes of mechanical suffocation - W75-W76, W78-W84 - including suffocation with a plastic bag, inhalation and ingestion of food, foreign body, accidental suffocation.
Mechanical asphyxia develops rapidly, begins with a reflex holding of breath, and is often accompanied by loss of consciousness during the first 20 s. Vital signs in classical strangulation go through 4 stages in sequence:
- 60 s – onset of respiratory failure, increase in heart rate (up to 180 beats/min) and pressure (up to 200 mmHg), the attempt to inhale prevails over the attempt to exhale;
- 60 s – convulsions, blueness, decreased heart rate and pressure, the attempt to exhale prevails over the attempt to inhale;
- 60 s – short-term cessation of breathing;
- up to 5 minutes – intermittent irregular breathing persists, vital signs fade, the pupil dilates, and respiratory paralysis occurs.
In most cases, death occurs within 3 minutes when breathing stops completely.
Sometimes this can be caused by sudden cardiac arrest. In other cases, episodic palpitations may persist for up to 20 minutes after the onset of suffocation.
Consequences and complications
The pathology is quite dangerous and is one of the most common causes of child mortality. How favorable the prognosis will be depends on the severity of the baby’s condition and the Apgar indicator. If the score increases, the prognosis is considered favorableSource: Modern methods of treating neonatal asphyxia. Cherednikova E.N., Sherstnev D.G. Bulletin of Medical Internet Conferences, 2021. p.824.
However, with severe pathology, serious complications develop during the first year of life. Early consequences that may appear in the first few days after resuscitation include :
- respiratory arrest (the most common and dangerous complication);
- pulse failure;
- convulsions;
- cerebral edema;
- disruption of the urinary and digestive systems.
Later disorders include the following diagnoses:
- syndrome of increased excitability (hyperexcitability);
- increased intracerebral pressure (hypertension syndrome);
- lesions of the central nervous system (perinatal encephalopathy);
- disruptions in the functioning of the endocrine and vegetative-vascular systems (hypothalamic disorders).
With timely and competent medical intervention, as well as a high-quality recovery period, asphyxia of newborns may not have dangerous consequences in the future. Mild forms of asphyxia have almost no effect on the child; after the illness, his further development will proceed in the same way as in other babies.
Famous people who died from suffocation
History is replete with references to executions by hanging. Such a sentence was passed on robbers, murderers and other criminals who committed serious atrocities. Noble nobles laid their heads on the block, unlike ordinary people. Here will be listed those who, for various reasons, died from strangulation.
Decembrists
The sentence passed by the Supreme Criminal Court to hang five Decembrists was a mitigation of the painful death penalty by quartering. On July 13 (25), 1826, in the crownwork of the Peter and Paul Fortress, the lives of S. I. Muravyov-Apostol, P. G. Kakhovsky, K. F. Ryleev, P. I. Pestel, M. P. Bestuzhev-Ryumin were cut short. The first three fell from the noose and were hanged a second time. The previously existing tradition of pardoning those executed and replacing hanging with hard labor was abolished by Military Article No. 204 under Peter I.
Isadora Duncan
The tragic death of the famous dancer on September 14, 1927 occurred by an absurd accident. During a car ride in Nice, the artist’s fluttering scarf got tangled in the rear wheel of a convertible and literally pulled Isadora out of the car at full speed, breaking her spine.
Jacques Offenbach
The famous composer died of an attack of suffocation on October 5, 1880. His friend Johann Strauss, having learned about the sad event, interrupted his tour and rushed to Paris for the funeral.
Robin Williams
Around noon on August 11, 2014, the wife began knocking on the famous actor’s bedroom, concerned that he had not come out for breakfast. After breaking the door, she found Robin sitting by a chair with a belt fastened around his neck. The other end of the belt was inserted between the frame and the door leading to the wardrobe. Close friend Rob Schneider suggested that Robin was experiencing suicidal thoughts while taking a new drug for Parkinson's disease.
Prevention of newborn asphyxia
The expectant mother should be involved in the prevention of the pathological condition during pregnancy. To do this you should:
- attend routine gynecological consultations;
- adhere to the recommendations of the obstetrician-gynecologist;
- be sure to take vitamin complexes if prescribed by a doctor;
- monitor the condition of the fetus and placenta during routine ultrasound examinations;
- treat any diseases only under the supervision of a doctor, do not self-medicate;
- follow a daily routine, do not overload the body;
- get rid of bad habits;
- to walk outside.
In obstetrics, considerable attention is paid to the development of effective preventive methods that can reduce the risk of asphyxia during childbirth and during the first days of a baby’s life.
Sources:
- Modern methods of treating newborn asphyxia. Cherednikova E.N., Sherstnev D.G. Bulletin of Medical Internet Conferences, 2016. p.824
- Protocol for therapeutic hypothermia for children born with asphyxia. Ionov O.V., Balashova E.N., Kirtbaya A.R., Antonov A.G., Miroshnik E.V., Degtyarev D.N. Neonatology: News. Opinions. Training, 2014. p. 81-83
- Carrying out therapeutic hypothermia in newborns born with asphyxia. K. B. Zhubanysheva, Z. D. Beisembaeva, R. A. Maykupova, T. Sh. Mustafazade. Science of Life and Health, 2021. p. 60-67
- Asphyxia of newborns. Zhetpisova L.B. West Kazakhstan Medical Journal, 2011
- Fetal hypoxia and asphyxia of the newborn. Kuznetsov P.A., Kozlov P.V. General Medicine, 2021. p. 9-15
The information in this article is provided for reference purposes and does not replace advice from a qualified professional. Don't self-medicate! At the first signs of illness, you should consult a doctor.
Causes
The causes of asphyxia are very different, in particular, asphyxia in a child can develop due to allergies to certain foods, care products or medications.
Choking can occur as a result of:
- compression from outside the respiratory tract (for example, asphyxia during childbirth);
- pathological processes of the lungs and respiratory tract (edema, burns, spasms);
- ingestion of liquid or foreign bodies (water, vomit, blood) into the respiratory tract;
- tongue retraction;
- overdose of drugs, resulting in relaxation of the respiratory muscles;
- some diseases (botulism, myasthenia, etc.);
- asthmatic attacks, allergic edema, pleurisy;
- traumatic brain injury, stroke;
- prolonged convulsive conditions (tetanus);
- exposure to toxic substances (cyanides, nitrites, etc.).
Occupational conditions associated with the need to breathe a forced gas mixture can also provoke suffocation, which can lead to a disruption in the oxygen supply.
Asphyxia of newborns can be caused by aspiration of amniotic fluid, intracranial birth injuries, and fetoplacental insufficiency.
Prices
| Name of service (price list incomplete) | Price |
| Online opinion of a pediatrician (SPECIAL) | 0 rub. |
| Appointment (examination, consultation) with a pediatrician, primary, therapeutic and diagnostic, outpatient | 1750 rub. |
| Consultation (interpretation) with analyzes from third parties | 2250 rub. |
| Prescription of treatment regimen (for up to 1 month) | 1800 rub. |
| Consultation with a candidate of medical sciences | 2500 rub. |