Diseases that start with the letter “M”: Lesser chorea, Slow infections of the central nervous system, Medulloblastoma, Herniated disc, Thoracic disc herniation, Lumbar disc herniation, Cervical disc herniation, Intercostal neuralgia, Meningeal syndrome, Meningioma, Meningitis, Meningococcal meningitis, Meningomyelitis , Meningoencephalitis, Metabolic myopathy, Metastatic brain tumors, Metachromatic leukodystrophy, Weather sensitivity, Myasthenia gravis, Migraine stroke.
Meningoencephalitis is a disease of a neuroinfectious nature, occurring with simultaneous damage to the substance of the brain and its membranes. It is expressed by variable focal, membrane, infectious symptoms. The diagnosis is made on the basis of a neurological examination, assessment of cerebrospinal fluid, MRI and CT results of the brain, and examinations designed to identify the pathogen. Complex treatment consists of prescribing antibacterial, antiviral, antifungal drugs in combination with symptomatic and pathogenetic drugs.
Meningoencephalitis viral, bacterial, parasitic
The term “meningoencephalitis” includes two nosological forms: “encephalitis” and “meningitis”.
The definition describes the morphological changes that occur against the background of pathology - damage to the white matter and meninges. The pathology is characterized by high mortality, disability, and a large number of disorders. Diagnosis of the symptoms of the disease at the beginning of its development, prevent dangerous consequences, eliminate damage to functional centers. The effectiveness of treatment depends on the cause, pathogen, and extent of the inflammatory focus.
The initial signs of pathology are neurological disorders. Neurologists conduct differential diagnostics that allow one to suspect meningoencephalitis and timely prescribe neuroimaging methods (brain MRI and CT).
Development of the disease
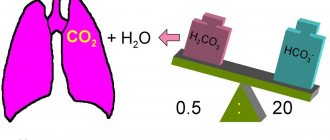
Inflammation is a response to the introduction of a pathogen into brain tissue. Its purulent or serous nature is associated with the type of infectious factor. An inflammatory focus forms around blood vessels, which causes cerebrovascular accident. As a result, secondary tissue ischemia and a compensatory increase in the production of cerebrospinal fluid occur, which affects the development of intracranial hypertension.
The membranes of the brain damaged by infection become irritated and cause meningeal syndrome. Inflammatory foci can have varying degrees of distribution in the cerebral substance. Focal manifestations are formed due to neurological insufficiency of brain functions. Persistent neurodeficiency is the result of massive death of brain neurons.
Meningoencephalitis - what is it?
There are congenital and acquired forms. Meningoencephalitis in children occurs due to intrauterine infection (cytomegalovirus, chlamydia, meningococcal). Immediately after birth, it is difficult to identify the nosology, since the child cannot talk about sensations.
In the first month of life, the first signs appear. Only the acute variety is accompanied by multiple changes, which often lead to death. Analysis of cerebrospinal fluid helps to suspect inflammation of the brain and membranes at the beginning of development.
The procedure is invasive and is prescribed according to strict indications. The harmlessness of MRI for meningoencephalitis makes it possible to prescribe examinations for newborns and infants. The high cost of equipment excludes the possibility of installing devices everywhere.
The main causes of mortality from inflammatory processes of the soft membrane and brain parenchyma:
- Intracerebral edema;
- Infectious shock;
- Cerebral hypertension;
- Kidney failure.
The consequences of the disease in subacute and chronic forms develop over several years.
MRI meningoencephalitis
Classification
Neurology divides meningoencephalitis according to the type of etiology, the nature of the changes caused, and the type of development. Confirmation of the type of disease occurs at the diagnostic stage, which is a central factor in choosing treatment tactics.
Etiological types of disease:
- Viral—the source includes herpes simplex, influenza, measles, rabies, cytomegalovirus, and enterovirus viruses. It has a serous type of inflammatory consequences.
- Bacterial - has a purulent inflammatory nature caused by pneumo-, strepto-, meningococci, Haemophilus influenzae, Klebsiella.
- Protozoan—a rare species caused by protozoa (amoeba, toxoplasma).
- Fungal—diagnosed mainly in individuals with secondary immune deficiency. Often accompanies the development of neuroAIDS.
According to the type of inflammatory course, meningoencephalitis is divided into:
- Serous - characterized by the formation of serous discharge. Blood lymphocytosis is typical. The cerebrospinal fluid is clear.
- Purulent—pus forms, which causes clouding of the cerebrospinal fluid. Leukocytosis is noted.
- Hemorrhagic—multiple petechial hemorrhages occur in the brain tissue, caused by impaired permeability of the vascular walls.
By type of clinical course:
- Lightning—forms within a matter of hours, in most cases ending in the death of the patient.
- Acute—develops from 1 to 2 days, the clinical picture worsens more slowly than with the fulminant form.
- Subacute—occurs in stages, symptoms worsen over several days, but not more than a week.
- Chronic—inflammation develops over several months with periods of remissions and exacerbations. Acute and subacute forms can become chronic.
ICD 10 code for meningoencephalitis
The international classification of the tenth revision identifies the following types of brain inflammation with code “G04”:
- Meningomyelitis;
- Meningoencephalitis;
- Acute ascending myelitis.
The category excludes multiple sclerosis (“G95”), toxic, alcoholic encephalopathy “G31.2”, “G92”.
Classification of meningoecephalitis by course:
- Chronic – long-term development with a slow increase in symptoms;
- Subacute - erased signs of nosology increase over two to three years;
- Acute – rapid progression of symptoms helps early diagnosis;
- Fulminant – rapid cerebral damage causes death.
The difficulties of verifying pathology are complicated by the variety of etiological factors.
Purulent meningoencephalitis: diagnosis
When a patient comes to the hospital with complaints about an existing disease, the diagnostic search begins with interviewing the patient and his relatives regarding a current or recently suffered infectious disease, identifying a history of TBI, the fact of vaccination, a tick bite, etc. Further diagnostic studies include the following:
- Neurological examination;
- Laboratory tests (CBC, OAM, blood biochemistry, bacteriological culture of blood and all body media for sterility, PCR);
- CT, MRI of the brain;
- Lumbar puncture. With purulent inflammation, the fluid is cloudy with a flaky sediment, with serous inflammation it is transparent, with hemorrhagic inflammation it contains elements of blood. In order to identify the pathogen, cerebrospinal fluid is examined under a microscope, cultured on various nutrient media, and PCR diagnostics;
- Stereotactic brain biopsy. This procedure is performed in complex diagnostic cases. Allows you to diagnose meningoencephalitis of parasitic etiology and exclude a tumor process.
Causes of meningoencephalitis
Viral forms provoke chronic and subacute varieties. An acute course can be observed in people with immunodeficiencies. Pathogenic bacteria quickly destroy the arachnoid, subarachnoid membranes, and brain parenchyma. Parasitic (amebic) species progress slowly.
Features of influenza hemorrhagic meningoencephalitis
Nosology is a consequence of influenza. An acute respiratory viral infection provokes a rise in temperature and enlargement of the pharyngeal tonsils. Long-term persistence of infection causes epileptic convulsions.
Fever increases brain destruction, but no antiviral treatment has been developed. Vaccination and strengthening the immune system are the main measures to counter the spread of influenza hemorrhagic infection.
Principles for diagnosing viral meningoencephalitis:
- Absence of bacteria in brain preparations when stained by Gram;
- Cerebrospinal fluid pleocytosis;
- Detection of enteroviruses, arboviruses, herpesviruses using polymerase chain reaction (PCR).
Severe and fatal cases are caused by enteroviruses. Over serotypes of pathogens have been identified, causing a variety of clinical manifestations of the disease. Enteroviral neuroinfection often leads to death and disability.
After a bite from ticks, insects, or mosquitoes, the inflammatory process of cerebral tissues is caused by arboviruses if the carrier was infected with microbes. In addition to humans, these pathogens infect horses and dogs, which can also be a source of infection for humans.
Common encephalitis caused by arboviruses:
- West Nile fever;
- Encephalitis St. Louis;
- California uniform.
The prevalence of diseases has been increasing in recent years.
Symptoms of herpetic encephalitis
Activation of herpetic neuroinfection is the cause of death in approximately seventy percent of adults and children. The lack of antiherpetic therapy excludes the possibility of effective treatment. Only a strong immune system can cope with the herpes virus. The weak body of a pregnant woman in the presence of infection becomes a source of infection of the fetus in utero.
Herpes simplex virus type 2 (HSV-2) becomes the source of a mild transient type of neuroinfection. Meningoencephalitis is activated in adolescents with an active sexual life.
In newborns, herpes simplex virus type 1 or 2 is part of the associated infections. A generalized disease affecting many organs is caused by HSV in patients with immunodeficiencies, including AIDS. The lack of pharmaceuticals causes the death of 2/3 of infants.
The first signs of herpesvirus neuroinfection:
- High fever;
- Strong headache;
- Behavioral disorders;
- General cerebral symptoms.
The drug virolex (acyclovir) increases your chances of survival. In severe cases, the drug is ineffective.
Rare forms of viral encephalitis
Damage to the central nervous system is caused by the varicella zoster virus, which occurs after an illness. Nosology has symptoms:
- Cerebellar ataxia – incoordination of muscle activity, unsteady gait;
- Acute encephalitis.
Acute manifestations are rare. The chickenpox virus is characterized by a chronic course with cycles of remissions and exacerbations, since the pathogen persists in the nerve ganglia. Reactivation of chickenpox is possible with a decrease in immunity.
Rare types of viral meningoencephalitis:
- Cytomegalovirus - destroys cerebral tissue only in immunodeficiencies;
- Mumps – caused by the mumps virus. It is characterized by a mild course, but causes inflammation of the auditory nerve.
The lack of a complete diagnosis excludes the possibility of early detection of neuroinfection.
Clinic of bacterial meningoencephalitis
Pathogenic bacteria enter the brain through the blood and lymphatic fluid. The penetration of microorganisms from the primary focus of internal organs is dangerous due to the resistance of the agents to the antibiotics used to eliminate the disease.
Types of bacterial meningoencephalitis:
- Brucellosis;
- Toxoplasmosis;
- Syphilitic;
- Tuberculous;
- Meningococcal.
Signs are determined by the type of etiological factor. Damage to cerebral tissue appears against the background of a primary infection of internal organs. Congenital types arise due to the entry of microorganisms into the fetus during childbirth.
Tuberculous encephalitis develops in people with primary tuberculosis of different localization. The peak of infection occurs in the spring-autumn period, when immune activity is reduced. The nosology has no specific manifestations. Diagnosed by laboratory, clinical and instrumental methods.
Mycobacterial infection is difficult to treat. Of the bacterial species, nosology is the most dangerous. Main clinical signs of pathology:
- Poor concentration;
- Strong headache;
- General cerebral disorders;
- Photophobia;
- Vegetative manifestations;
- Neurological disorders;
- Hydrocephalus.
Acute manifestations of the disease are characterized by an increase in temperature to thirty-nine degrees. Clinical manifestations of the disease are accompanied by fever, joint pain, sleep disturbance, abnormal meningeal signs, and fever. The average duration of the disease is about ten days. Associated signs of nosology are lack of appetite, excessive sweating, cerebellar disorders, mobility impairment, positive Rehberg test. (a person cannot touch the tip of his nose with his index finger).
The temperature curve against the background of inflammatory changes in the cerebral parenchyma and meninges has a specific course. Initially, the fever increases to 39 degrees. After 5-7 days, the fever subsides to low-grade levels (38.5 degrees). A second wave is observed on the tenth day. Focal neurological symptoms appear with neuritis, radiculitis, changes in the activity of the heart, pulmonary system, dizziness, convulsions, paresthesia (lack of sensitivity).
The brucellosis species provokes pyramidal symptoms with paresis, paralysis, and muscle cramps.
Characteristics of parasitic meningoencephalitis
Amoebas are found in young children and newborns. The parasites cause inflammation of the brain with a high mortality rate.
Pathogens enter through the upper respiratory tract. The source of infection is reservoirs, tap water, contaminated vegetables and fruits.
Clinical manifestations of amoebic encephalitis, meningitis:
- Granulomatous inflammation of the white matter takes several months to form. Damage to the membranes clinically resembles a volumetric intracerebral formation with the formation of several centers of activity - convulsions, personality disorders, paralysis, paresis;
- Acute variety - lasts two weeks. It begins with lightning speed, accompanied by nausea, headaches, and a significant increase in temperature. Multiple foci cause death in infants and children.
Early detection and proper drug therapy eliminate the risk of serious complications.
Etiology
The main cause of pathology is infection. Neurotropic pathogens enter the brain areas, thus causing primary infection. Secondary infection is the result of the expansion of the process from infected foci (sinusitis, otitis), with general processes (rubella, influenza). The cause of the disease is bacteria and viruses, sometimes pathogenic fungi. Infection occurs when:
- Entry of the pathogen into the nasopharynx through alimentary or airborne droplets. Through the bloodstream, it is possible to bring the pathogen into the cranial cavity, where it causes inflammatory changes and the further formation of meningoencephalitis.
- Insect bite (tick, mosquito). Viral meningoencephalitis and encephalitis have a transmissible transmission route (tick-borne encephalitis, Japanese mosquito encephalitis, St. Louis encephalitis). The pathogen is released from an insect bite into the blood and enters the brain, which causes the development of meningoencephalitis.
- Presence of infection in the body. Meningoencephalitis can become a complication of tuberculosis, purulent maxillofacial diseases, and syphilis. In some cases, it develops as a consequence of certain acute respiratory viral infections.
- Traumatic brain injury. Contact infection occurs with open injuries with skull fractures. Meningoencephalitis, as a post-traumatic complication, occurs in 1.3-3.5% of patients.
- Vaccination. The infection develops when the immune system is weakened, after the administration of a live vaccine. The pathogen passes the blood-brain barrier and causes meningoencephalitis.
- The pathogen does not always lead to the development of the disease. This becomes possible in the presence of a weakened, immature immune system, a weakened body, or the presence of initial or secondary immunodeficiency.
Characteristics of autoimmune encephalitis
The formation of antibodies to brain tissue causes demyelination. The process is long but progressive. Rasmussen's encephalomyelitis is a typical manifestation of an autoimmune lesion of the cerebral parenchyma. Depending on the characteristics of the development of the process, the duration is from five to fifteen years. In most cases, the clinical peak occurs at six years of age.
Nosology has been thoroughly studied by scientists. The causes of the occurrence could not be established, but the link to which immunoglobulins are formed was identified. The presence of NMDA receptors is a weak point that is susceptible to destruction by the immune system.
There are case studies showing the nonspecificity of glutamate receptor antibodies for Rasmussen's encephalomyelitis. Other anti-inflammatory cytokines formed during the nosology have been identified.
Meningoencephalitis of newborns
The most common pathogen is viruses. Intrauterine infection of a baby occurs from a mother suffering from glandular fever, measles, rubella, herpetic infection, and mumps.
The most common symptoms are focal disorders, hyperkinesis, hydrocephalus. Nonspecific manifestations of meningoencephalitis in newborns:
- Eye twitching;
- Difficulty feeding from the breast;
- High fever;
- Intoxication syndrome;
- Vomiting reflex;
- Diarrhea;
- Strabismus;
- Increased heart rate (tachycardia);
- Muscle twitching.
Neurologists define neurological disorders in the form of Kernig's sign (the inability to bring the head to the chest due to stiff neck muscles). Cerebrospinal fluid contains an increased amount of lymphocytes and protein.
Meningoencephalitis: classification
Today, neurologists divide meningoencephalitis into various types according to several criteria: etiology, nature of morphological changes and type of course. Based on etiology, the following types of encephalitis are distinguished:
- Viral - pathogens can be influenza viruses, herpes simplex, measles, rabies, cytomegalovirus, enteroviruses. The serous nature of inflammatory changes predominates;
- Bacterial - pathogens can be strepto-, meningo-, pneumococci, Klebsiella, Haemophilus influenzae. The inflammation has a purulent nature of inflammatory changes;
- Protozoan - extremely rare. Infectious agents are amoebas, toxoplasma and other protozoa;
- Fungal – mainly observed in immunocompromised individuals. Can be diagnosed as part of neuroAIDS.
Manifestations of meningoencephalitis in adults
Various symptoms of the disease in an adult are caused by different pathogens and characteristics of the course. The incubation period of the disease lasts several weeks.
Symptoms of the clinical stage:
- Muscle stagnation;
- Decreased appetite;
- Constant fatigue;
- Headaches without the effectiveness of painkillers.
Inflammatory changes in the meninges lead to meningeal syndrome with special manifestations:
- Nausea;
- Speech disorders;
- Interruptions of heart activity;
- Respiratory disorders.
The occurrence of the described manifestations leads to death. The progression of individual symptoms becomes a cause of disability.
Clinical picture of the disease
The clinical picture of meningoencephalitis combines general infectious, meningeal, liquor-hypertensive, and focal symptoms. Infectious manifestations include high body temperature, a general painful condition, decreased appetite, and sometimes skin rashes. Against the background of an ongoing infection, signs of brain damage appear.
Increased pressure in the cerebrospinal fluid causes severe headache, nausea, and vomiting, which does not provide relief. Increasing intracranial pressure leads to a disorder of consciousness with disorientation, mental agitation or, on the contrary, retardation. In the fulminant form, the patient often falls into a coma.
Focal neurological failure depends on the location and type of inflammation and is expressed to varying degrees. Manifests itself in the form of hemiparesis, sensorimotor aphasia, hyperkinesis, cerebellar syndrome, vestibular ataxia, and cognitive impairment. Oculomotor and visual disorders, ptosis, facial distortion, swallowing disorders, and dysarthria are the result of damage to the cranial nerves.
Consequences of meningoencephalitis
In addition to high mortality, the disease is characterized by dangerous conditions leading to disability. Severe consequences of inflammation of the white matter and meninges:
- Paralysis of limbs;
- Epileptic seizures;
- Mental retardation in children;
- Hydrocephalus;
- Psychoses;
- Hallucinosis.
The conditions are irreversible. Early verification and competent therapy prevent negative consequences in bacterial types of encephalitis and meningitis. For other forms of nosology, the prognosis is unfavorable.
Treatment
An integrated approach to treatment includes a combination of pathogenetic, etiotropic and symptomatic therapy in the intensive care unit:
- Antibacterial treatment includes cephalosporins with ampicillin. The adjustment occurs after isolating the pathogen and determining sensitivity.
- Antiviral drugs are included in treatment when determining the viral etiology. Ganciclovir is prescribed for herpes, ribavirin for arbovirus. Additionally, interferon is prescribed.
- Among antifungal drugs, fluconazole B and amphotericin B have a powerful effect. Sometimes they are combined in especially severe cases.
- Antiparasitic drugs are combined with antibiotics and antifungal agents.
- Diuretics and glucocorticosteroids reduce cerebral edema. The integrity and viability of neurons is ensured by neuroprotectors and neurometabolites.
Symptomatic treatment relieves the main signs of the disease. It includes cardiovascular drugs, oxygen therapy, mechanical ventilation, anticonvulsants and psychotropic drugs. Rehabilitation measures are aimed at restoring nervous functions (massage, physiotherapy, exercise therapy, acupuncture).
Diagnosis of inflammation of the brain and soft membranes
The most accurate laboratory method for verifying nosology at the beginning of development is cerebrospinal fluid analysis. Turbidity in the cerebrospinal fluid that bathes the brain and spinal cord indicates the presence of infection. Determination of additional impurities, accumulations of leukocytes and lymphocytes indicates a bacterial infection. With pathology, an increase in the content of glucose and protein occurs.
Clinical and instrumental methods for examining the cerebral parenchyma - radiography, CT, MRI, electroencephalography (EEG). Neuroimaging determines the spread of inflammation, the depth of the lesion, and concomitant pathology.
Meningitis
Encephalitis
Fungus
Vomit
Rubella
Measles
30189 07 June
IMPORTANT!
The information in this section cannot be used for self-diagnosis and self-treatment.
In case of pain or other exacerbation of the disease, diagnostic tests should be prescribed only by the attending physician. To make a diagnosis and properly prescribe treatment, you should contact your doctor. Meningitis: causes, symptoms, diagnosis and treatment methods.
Definition
Meningitis is an infectious inflammation of the meninges of the brain and spinal cord, accompanied by intoxication, fever, increased intracranial pressure syndrome, meningeal syndrome, as well as inflammatory changes in the cerebrospinal fluid.
The meninges are connective tissue membranes that cover the brain and spinal cord. There are dura mater, arachnoid and pia mater.
The dura mater of the brain has a dense consistency and thickness of 0.2-1 mm; in places it fuses with the bones of the skull. The arachnoid membrane is a thin, translucent, non-vascular connective tissue plate that surrounds the brain and spinal cord. The soft shell is a thin connective tissue plate directly adjacent to the brain, corresponds to its relief and penetrates into all its recesses. In its thickness is the vascular network of the brain.
The most common inflammation is inflammation of the pia mater, and the term “meningitis” is used.
Causes of meningitis
The meninges can be involved in the inflammatory process primarily and secondary. Meningitis that occurs without a previous general infection or disease of some other organ is called primary. Secondary meningitis develops as a complication of an existing infectious process. Secondary ones include tuberculous, staphylococcal, pneumococcal meningitis. The primary ones are meningococcal, primary mumps, enteroviral meningitis and others.
The disease is transmitted by airborne droplets, household contact or nutrition.
Purulent inflammation of the meninges can be caused by various bacterial flora (meningococci, pneumococci, and less commonly, other pathogens). The cause of serous meningitis is viruses, bacteria, fungi.
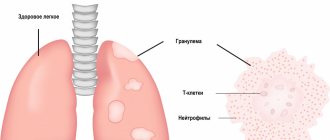
According to the forecast, the most dangerous is tuberculous meningitis, which occurs when there is a tuberculous lesion in the body. The development of the disease occurs in two stages. At the first stage, the pathogen, through the bloodstream, infects the choroid plexuses of the ventricles of the brain with the formation of a specific granuloma in them. In the second, inflammation of the arachnoid and soft membranes is observed (as a rule, the membranes of the base of the brain are affected), which causes acute meningeal syndrome.
The development process of meningococcal meningitis also consists of several stages:
- contact of the pathogen with the mucous membrane of the nasopharynx;
- entry of meningococcus into the blood;
- penetration of the pathogen through the blood-cerebrospinal fluid barrier, irritation of pia mater receptors by toxic factors and inflammation.
The course of the infectious process depends on the pathogenic properties of the pathogen (the ability to cause disease) and the state of the human immune system.
Previous viral diseases, sudden climate change, hypothermia, stress, concomitant diseases, therapy that suppresses the immune system can be significant for the occurrence and course of meningitis.
Classification of the disease
According to the type of pathogen:
- Viral meningitis (influenza, parainfluenza, adenovirus, herpes, arbovirus (tick-borne), mumps, enterovirus ECHO and Coxsackie).
- Bacterial meningitis (meningococcal, tuberculous, pneumococcal, staphylococcal, streptococcal, syphilitic, brucellosis, leptospirosis).
- Fungal (cryptococcal, candidiasis, etc.).
- Protozoal (toxoplasmosis, malaria).
- Mixed.
According to the nature of inflammation:
- Serous.
- Purulent.
According to the mechanism of occurrence:
- Primary.
- Secondary.
With the flow:
- Spicy.
- Subacute.
- Fulminant.
- Chronic.
By severity:
- Easy.
- Medium-heavy.
- Heavy.
According to the prevalence of the process:
- Generalized.
- Limited.
According to the presence of complications:
- Complicated.
- Uncomplicated.
Symptoms and syndromes of meningitis
There are a number of syndromes common to all meningitis:
- meningeal syndrome - manifested by rigidity (increased tone) of the neck muscles and long back muscles, hypersthesia (increased sensitivity) of the sensory organs, headache, vomiting, changes in the cerebrospinal fluid;
- cerebral syndrome - manifested by drowsiness, impaired consciousness, nausea, vomiting, dizziness, psychomotor agitation, hallucinations;
- asthenovegetative syndrome – manifested by weakness, decreased ability to work;
- convulsive syndrome;
- general infectious syndrome - manifested by chills and fever.
Meningococcal meningitis ranks first among purulent meningitis.
Its incubation period ranges from 1 to 10 days, with an average of 2-4 days. The disease usually begins acutely against the background of complete health or shortly after nasopharyngitis. Patients can indicate not only the day, but also the hour of illness; they are worried about chills, body temperature above 38℃, severe bursting headache, aggravated by any noise and movement of the head. Patients may experience pain in various parts of the body, and touching causes excruciating sensations. Vomiting is not associated with food intake and does not bring relief. Soon, stiffness of the neck and long back muscles sets in. Patients take a “meningeal” position. Infants cry constantly, they may experience bulging fontanelles and gastrointestinal disorders. Pneumococcal meningitis, as a rule, is observed in young children against the background of an existing pneumococcal process (pneumonia, sinusitis).
With streptococcal meningitis, hepatolienal syndrome (enlarged liver and spleen), renal failure, adrenal insufficiency, petechial rash (hemorrhages due to damage to the capillaries, as a result of which blood, spreading under the skin, forms round spots, the size of which does not exceed 2 mm).
Purulent meningitis caused by Pseudomonas aeruginosa and fungi are rare. The diagnosis is established only after additional laboratory tests.
Serous tuberculous meningitis is characterized by a gradual onset, although in rare cases it can manifest itself acutely. At the onset of the disease, patients complain of fatigue, weakness, irritability, and sleep disturbances. The temperature is usually no higher than 38℃, and there is an intermittent moderate headache. On the 5-6th day of illness, the temperature rises above 38℃, the headache intensifies, nausea, vomiting, and drowsiness appear. Unconsciousness develops quickly. A divergent strabismus, a low position of the upper eyelid in relation to the eyeball, and pupil dilation may be observed.
When diagnosing mumps meningitis, it is important to identify recent contact with someone with mumps.
Clinical manifestations of damage to the meninges may develop even before the enlargement of the salivary glands.
Enteroviral meningitis is characterized by two- and three-wave fever with intervals between waves of 1-2 or more days. Other manifestations of enterovirus infection are almost always observed (muscle pain, skin rash, herpangina).
For the diagnosis of measles and rubella meningitis, an indication of contact with a patient with these diseases, as well as typical clinical symptoms of measles or rubella, is of great importance.
Diagnosis of meningitis
To confirm the diagnosis of meningitis, the doctor may prescribe a set of laboratory and instrumental studies:
- clinical blood test with determination of hemoglobin concentration, number of erythrocytes, leukocytes and platelets, hematocrit and erythrocyte indices (MCV, RDW, MCH, MCHC), leukoformula and ESR (with microscopy of a blood smear in the presence of pathological changes);