Asthenia means weakness that occurs in the absence of exertion, lasts for a long time and does not go away even after a long rest. The main difference between asthenia and physiological fatigue is the ineffectiveness of sleep and its chronic course. In foreign literature, the term “chronic fatigue syndrome” is sometimes used to refer to asthenia.
Every fifth (10-25%) patient seeking medical help complains of asthenia [1]. In many cases, it is possible to establish a connection between asthenia and the effects of pathogenic biological or psychological factors. In particular, asthenia is a characteristic complaint of patients with organic diseases of the brain (chronic cerebrovascular insufficiency, post-traumatic encephalopathy, etc.) [1-3]. Such patients are especially susceptible to rapid mental exhaustion. Prescribing nootropic drugs, normalizing metabolic processes in the central nervous system, improves the well-being of such patients.
In many cases, asthenia is accompanied by mild to moderate cognitive impairment, autonomic dysfunction, emotional disturbances, including severe depression and anxiety. Thus, it was shown that 28% of patients with long-term (more than 6 months) current asthenia develop severe anxiety-depressive syndrome [3]. According to one of the multicenter placebo-controlled randomized studies [4], cytoflavin not only reduced the severity of asthenia in patients with asthenoneurotic syndrome against the background of chronic cerebral ischemia, but also improved cognitive functions and quality of life.
According to research by D.I. Laseeva and O.V. Dikova [5], cytoflavin had a positive effect on the emotional state in patients with eczema. In our previous study [6], we also observed more pronounced positive dynamics in women with depression due to organic brain disease who received cytoflavin as an additional therapy, compared with the control group (the study is being prepared for publication). In addition, in the same group of patients, we observed a normalization of autonomic disorders under the influence of cytoflavin.
Cytoflavin produced by NTFF POLYSAN LLC includes succinic acid, riboxin, nicotinamide and riboflavin, which are important components of normal metabolic processes in the brain. The drug is well tolerated and is used for encephalopathies of various origins (toxic, posthypoxic), for acute and chronic cerebrovascular accidents [7, 8]. In acute conditions, cytoflavin is used intravenously, and in chronic diseases it is prescribed in tablet form, 2 tablets 2 times a day for a course of at least 25 days [3].
The purpose of the study was to study the effect of cytoflavin as an additional therapy in patients with organic emotionally labile (asthenic) disorder.
Material and methods
The present study was observational.
The study included 100 patients, 49 men and 51 women, with organic emotionally labile (asthenic) disorder (F06.6 according to ICD-10), who underwent inpatient treatment at the Scientific and Practical Center for Psychoneurology of the Moscow Department of Health in 2012-2013.
The criteria for inclusion in the study were: severe asthenic disorders (75 or more points on the asthenic state scale) lasting at least 3 months as the main reason for seeking medical help; development of an asthenic state against the background of an organic brain disease due to severe perinatal pathology with developmental delay, chronic cerebral circulatory failure or traumatic brain injury; age over 25 years and under 60 years; complete secondary or higher education; absence of neurometabolic therapy for 3 months before the study. Exclusion criteria were: psychotic disorders or suicidal intentions; uncorrectable visual or hearing impairment; serious neurological or somatic diseases; alcoholism or drug addiction; pregnancy; history of allergic reactions or hypersensitivity to cytoflavin.
All patients were divided into two groups - the main and control groups of 50 people in each. Patients in the main group received cytoflavin in addition to basic therapy.
Cytoflavin was prescribed twice a day, 2 tablets. The duration of therapy was 3-4 weeks. Patients in the control group received only basic therapy. Basic therapy included antidepressants, vascular drugs, and in some cases drugs with sedative and/or antipsychotic effects. All patients were consulted by psychologists and psychotherapists, took courses in hydro- and electrophysiotherapy, received massage of the collar area, and did physical therapy.
Tolerability of cytoflavin was assessed based on side effects in two groups of patients.
All patients underwent an EEG to monitor high-amplitude paroxysmal τ-activity in the central leads or the presence of epileptic brain activity.
The effect of cytoflavin on the symptoms of the disease was assessed by the dynamics of asthenia indicators, the results of cognitive tests, changes in the level of depression, anxiety, autonomic disorders and quality of life after the course of treatment in comparison with the condition of patients in the first days of hospital stay, depending on taking cytoflavin.
The severity of asthenia symptoms was assessed using the asthenic state questionnaire. The technique was developed by L.D. Malkova and adapted by T.G. Chertovaya on the basis of clinical and psychological observations and the MMPI questionnaire. The questionnaire contains 30 questions, the answers to which are ranged from 1 point (no, incorrect) to 4 points (absolutely true). An indicator of 51-74 points is interpreted as mild asthenia, 75-100 points - moderate asthenia, 101-120 points - severe asthenia.
The severity of depression and anxiety was assessed using the Hospital Depression and Anxiety Scale and the Beck Depression Inventory [9]. The Hospital Scale consists of 14 items, 7 of which assess symptoms of depression and 7 of which assess symptoms of anxiety. The Beck Inventory consists of 21 items assessing symptoms of depression.
Autonomic disorders were assessed using the Autonomic Disorders Scale [10]. The scale consists of 2 parts. The Objective Autonomic Disorders subscale consists of 13 items and is completed by the clinician. The subjective autonomic disorders subscale consists of 11 items and is completed by the patient.
Cognitive function was examined using the Montreal Cognitive Assessment Scale (MoCa) [11]. The scale consists of 12 tasks assessing attention and concentration, memory, visual-constructive skills, abstract thinking, and speech functions. The maximum number of points is 30.
Quality of life was assessed using the SF-36 questionnaire (36-item short form Health Survey) [1, 12]. The questionnaire contains 36 items, on the basis of which 8 subscales are formed: physical functioning, role limitations due to physical problems, physical pain, general health, energy, social functioning, role limitations due to emotional problems, mental health.
Statistical analysis of the obtained data was carried out using the SPSS17 software package. The dynamics of psychological and other indicators were assessed using the Repeated measures ANOVA test, in which the grouping factor was the presence or absence of cytoflavin therapy. Since in a previous study we found differences in the severity of the effect of cytoflavin in men and women [6], in this work we included gender in the analysis as a second grouping factor. If there were between-group differences in testing, baseline test performance was also included in the analysis as a covariate.
According to the World Health Organization, more than 90% of adults on the planet drink alcoholic beverages. Moreover, about 10% of men and 3-5% of women drink alcohol daily. Since excessive alcohol consumption causes numerous disruptions in the functioning of almost all organs and systems of the body, leading to the emergence of multiple organ pathologies, it is not surprising that in most countries of the world, diseases associated with alcohol consumption are in 3-4th place among the causes of death [2 , 9]. The problem of alcohol dependence is also relevant for Ukraine, where only 628,379 people, or 1344.1 patients per 100,000 population, were registered at the dispensary drug treatment center as of 01/01/07 [5].
Alcohol dependence syndrome is a condition caused by chronic intoxication. It is no coincidence that the treatment of such patients begins with the elimination of the metabolic consequences of prolonged exposure to ethanol on the body. In this regard, a drug such as cytoflavin, whose spectrum of action is adequate to the tasks of detoxification, attracts attention. Cytoflavin is produced in the form of a solution for intravenous injection. 1 ml of solution contains 100 mg of succinic acid, 10 mg of nicotinamide, 20 mg of riboxin (inosine), 2 mg of riboflavin mononucleotide (riboflavin), as well as excipients - N-methylglucamine (meglumine), sodium hydroxide and water for injection.
The pharmacological effects of cytoflavin are due to the complex influence of the substances that make up its composition. The drug stimulates cellular respiration and energy production in cells, improves the processes of oxygen utilization by tissues, and restores the activity of antioxidant enzymes. It activates intracellular protein synthesis, promotes the utilization of glucose, fatty acids and the resynthesis of γ-aminobutyric acid (GABA) in neurons through the Roberts shunt. It also improves coronary and cerebral blood flow, activates metabolic processes in the central nervous system, restores reflex reactions, sensitivity and intellectual-mnestic functions of the brain. It has an awakening effect when prescribed to patients with a depressed consciousness due to anesthesia. The intracellular interaction of nicotinamide, riboxin and riboflavin mononucleotide stimulates the formation of important endogenous redox enzymes - flavin adenine nucleotide (FAD) and nicotinamide adenine dinucleotide phosphate (NADP), which play an important role in cellular and tissue respiration. With intravenous infusion at a rate of about 2 ml/min (in terms of undiluted cytoflavin), succinic acid and riboxin (inosine) are utilized almost instantly and are not detected in the blood plasma. Riboxin (inosine) is metabolized in the liver to form glucuronic acid, followed by its oxidation. A small amount is excreted by the kidneys. Nicotinamide is quickly distributed throughout all tissues, penetrates the placenta and into breast milk, is metabolized in the liver to form nicotinamide - methylnicotinamide, and is excreted by the kidneys. The plasma half-life is about 1.3 hours, the steady-state volume of distribution is about 60 L, and the total clearance is about 0.6 L/min. Riboflavin is distributed unevenly - the largest amount is in the myocardium, liver, and kidneys. The plasma half-life is about 2 hours, the steady-state volume of distribution is about 40 L, and the total clearance is about 0.3 L/min. Penetrates through the placenta and into mother's milk. Plasma protein binding is 60%. Excreted by the kidneys, partly in the form of a metabolite; in high doses, mainly unchanged.
Cytoflavin is used as part of complex therapy in the treatment of acute cerebrovascular accident, stage 1-2 discirculatory (vascular) encephalopathy and the consequences of cerebral circulatory disorders (chronic cerebral ischemia), toxic and hypoxic encephalopathy in acute and chronic poisoning, endotoxicosis, and also after depression of consciousness due to anesthesia. In adults, it is used exclusively intravenously in a dilution of 100-200 ml of 5-10% glucose solution or 0.9% sodium chloride solution 1-2 times a day, with an interval between administrations of 8-12 hours for 5 days. With rapid drip administration, undesirable reactions may occur that do not require discontinuation of the drug: hyperemia of the skin of varying severity, sensations of heat, bitterness and dry mouth, sore throat. With prolonged use of high doses, transient hypoglycemia, hyperuricemia, and exacerbation of gout may occur. Very rarely, short-term pain and discomfort in the epigastric region and sternum, shortness of breath, nausea, headache, stupor, “tingling” in the nose, blanching of the skin of varying severity, and itching may occur.
Contraindications to the use of cytoflavin are: individual sensitivity to the components of the drug, the period of breastfeeding. For patients who are on mechanical ventilation, it is not recommended to administer the drug when the partial pressure of oxygen in arterial blood decreases to less than 60 mmHg. The drug is prescribed with caution for nephrolithiasis, gout, and hyperuricemia. In case of overdose, symptomatic treatment is necessary, since there is no specific antidote. In critical conditions, the drug should be prescribed after normalization of central hemodynamic parameters. When prescribing, it is necessary to take into account a possible decrease in blood glucose levels; urine during treatment with the drug may acquire a more intense yellow color.
Cytoflavin ingredients such as succinic acid, inosine and nicotinamide are quite compatible with other drugs. At the same time, riboflavin, which is part of the drug, reduces the activity of a number of antibiotics: doxycycline, tetracycline, oxytetracycline, erythromycin and lincomycin. In addition, it is incompatible with streptomycin. Chlorpromazine, imizine, amitriptyline, by blocking flavin kinase, activate the inclusion of riboflavin in flavin adenine mononucleotide and flavin adenine dinucleotide and increase its excretion in the urine. Thyroid hormones accelerate the metabolism of riboflavin. It also reduces and prevents the side effects of chloramphenicol (disturbance of hematopoiesis, optic neuritis). Cytoflavin is compatible with drugs that stimulate hematopoiesis, antihypoxants, and anabolic steroids. Thus, the pharmacological properties of cytoflavin suggest that it may be useful when prescribed to alcohol-dependent patients during the detoxification phase.
The purpose of this work is to evaluate the effectiveness and safety of cytoflavin in the complex therapy of patients with alcoholism at the stage of relieving alcohol withdrawal syndrome.
Material and methods
An open comparative clinical study was conducted in parallel groups (without placebo control). The total duration of the study was 10 days. During this period, 7 patient visits took place: visit 1 was devoted to screening (preliminary examination with setting the date of hospitalization); daily visits from 2 to 6 (days 1-5 of treatment, respectively) and final visit 7 covered the period of relief of alcohol withdrawal syndrome and acute post-intoxication disorders[].
We observed 60 patients who, in accordance with ICD-10 criteria, were diagnosed with alcohol withdrawal syndrome (F-10.3). All patients were routinely (after a screening visit the day before) hospitalized in the departments of the Kharkov City Clinical Narcological Hospital No. 9, which is the clinical base of the Institute of Neurology, Psychiatry and Narcology of the Russian Academy of Medical Sciences of Ukraine.
The patients were randomly divided into 2 groups: 30 patients made up the main group and 30 - the control group. Patients in the control group received standard therapy without cytoflavin. The average values of age, body weight and some indicators of alcohol history in patients of the main and control groups at the start of the study are presented in Table. 1
.
These data indicate that the selected groups were quite comparable in terms of the main specified parameters and, therefore, suitable for analyzing the results of standard and study types of treatment.
The detoxification therapy scheme for patients dependent on alcohol was complex (Table 2)
.
Both the main and control groups received the following basic therapy: intravenous drip: NaCl 0.9% up to 1200 ml + MgSO4 25% up to 30 ml + vitamins B1/B6 up to 10 ml + KCl 10% up to 10 ml; intramuscularly pyrogenal - 25-100 mcg and unithiol 5% - 5.0 ml; orally: pyrroxan - 0.03 (2 tablets) 4 times a day; neurovitan - 1 tablet 3 times a day, gidazepam - 0.05 in the morning and 0.1 in the afternoon and evening, carbamazepine 200 mg 2 times a day); rational psychotherapy (20 minutes daily). In addition, in the main group, in accordance with the purpose of the work, cytoflavin 10 ml, diluted in 200 ml NaCl 0.9%, was used intravenously once a day.
During the study, a complex of clinical, psychometric and laboratory research methods were used to assess the current condition of the patients and, accordingly, the effectiveness and tolerability of the treatment used.
The clinical-psychopathological method was the main one in assessing the condition of patients throughout the study. Interpretation of data obtained using any other methods was carried out in the process of comparison with the results of a clinical-psychopathological study, which was carried out in accordance with the ICD-10 criteria [8].
During treatment, patients in both groups underwent a daily test for the presence of alcohol vapor in their exhaled air (alco-test). To monitor alcohol withdrawal syndrome throughout treatment, vital indicators (blood pressure, heart rate, body temperature, etc.) were monitored daily and 4 times (upon admission, as well as on the 3rd, 5th and 10th days of treatment). ) assessment of the severity of withdrawal symptoms using the screening test CIWA-Ar (The Clinical Institute Withdrawal Assessment for Alcohol-Revised) [4, 6]. Twice, upon admission and on the 10th day of observation, the intensity and structure of pathological craving for alcohol (PCA) was assessed using N.V.’s glossary. Cherednichenko-V.B. Altshuler [7].
Statistical processing of the obtained data was carried out using methods of mathematical statistics (variance, correlation, regression analysis) [1, 3] using SPSS 15.0 and Excel 2003.
Results and discussion
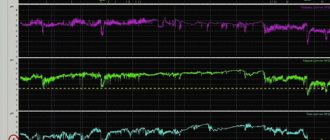
Changes in hemodynamic parameters - systolic and diastolic blood pressure, heart rate, as well as body temperature are the most important objective manifestations of that powerful homeostatic stress, which, in fact, is always the transition from systematic alcoholism to sobriety. For this reason, close attention was paid to these indicators (Fig. 1, 2)
.
Figure 1. Dynamics of average values of systolic and diastolic blood pressure in patients of the main (A) and control (B) groups.
Here and in Fig. 2: *—statistically significant differences between groups (p<0.05). Figure 2. Dynamics of average values of heart rate and body temperature in patients of the main (A) and control (B) groups. It is not difficult to notice that changes in all the mentioned physiological parameters are of the same type. First (from the 1st to the 3rd-5th visits) their increase is observed, then (from the 3rd to the 7th visits) - a decrease. Noteworthy is the fact that at the stage of relieving the withdrawal syndrome in patients receiving standard therapy along with cytoflavin therapy (the main group), normalization of hemodynamic parameters occurred significantly earlier than in patients in the control group.
As a result, from the 3rd to the 7th visits (2-10th days from the start of the therapeutic program), hemodynamic parameters (systolic and diastolic blood pressure, heart rate) were significant in the main group ( p
<0.05) lower than in the control group
(see Fig. 1 and 2)
. There were no significant differences in body temperature between the main and control groups throughout the study. From the above data it follows that cytoflavin, at the stage of relieving alcohol withdrawal syndrome, significantly reduces the strength of homeostatic stress associated with the transition from systematic alcoholism to sobriety, which is manifested by accelerated normalization of hemodynamic parameters.
The dynamics of the average results of the screening test to assess the severity of alcohol withdrawal syndrome CIWA-Ar during the relief of alcohol withdrawal syndrome in patients of the main and control groups is presented in Table. 2
. It was found that the various manifestations of alcohol withdrawal syndrome taken into account by CIWA-Ar (nausea and/or vomiting, tactile, visual, auditory disturbances, tremors, paroxysmal sweating, anxiety, headache and/or heaviness in the head, agitation, disorientation and confusion) consciousness), reach their maximum severity at the time of visit 4 (3rd day of cessation of alcoholism), and then begin to decrease.
In the main group of patients, the reduction of some symptoms of withdrawal syndrome occurred faster than in the control group, which was reflected in significantly lower degrees of severity of nausea or vomiting (visit 4), tremor (visits 4-6), paroxysmal sweat (visits 4-6), heaviness in head or headache (visits 4-6), and, as a result, the severity of alcohol withdrawal syndrome in general (visits 4-6).
PVA is a core symptom of alcohol dependence syndrome. It is PVA that becomes the main cause of alcoholic excesses during treatment and relapses of alcoholism in the post-therapeutic period. The dynamics of the average severity of PVA, its components and their components in the examined main and control groups during treatment are presented in Table. 3
.
It shows that over the course of 10 days of observation, the intensity of PVA decreased markedly, which can be easily explained by the relief of the painful effects of alcohol withdrawal syndrome.
Along with the general features in the nature of PVA reduction, significant differences were found between the groups. In a component-by-component comparative analysis, it was found that in the main group the severity of disturbances in appetite, dreams, facial reactions, and the autonomic component of PVA on the 10th day of treatment was significantly less than in the control group.
Since the main group differed from the control group only in that it used cytoflavin in addition to basic therapy, all of the above differences should be considered the result of the action of this drug.
Compliance with the sobriety regime by patients was assessed at each visit based on the results of an alcohol test, as well as through a retrospective anamnestic analysis of the period since the previous visit. The dynamics of the number of people who had alcoholic excesses during treatment, according to positive alcohol test results during visits, is presented in Fig. 3
.
Figure 3. The number of people who had alcoholic excesses according to positive alcohol test results in absolute (I) and relative (II) values during treatment (when calculating relative values, the decrease in the number of groups during treatment was taken into account).
* — differences between the main (A) and control (B) groups are significant (p<0.05). It can be seen that the first alcoholic excesses began at the stage of relieving the withdrawal syndrome, in hospital conditions (visit on the 6th or 5th day from the start of treatment). At the same time, the frequency of alcoholic excesses in the control group was slightly higher than in the main group, which may be explained by the ability of cytoflavin to suppress the vegetative component of PVA (as mentioned above). However, the differences between the comparison groups in the frequency of alcoholic excesses were not statistically significant, so this assumption needs further testing.
The results obtained in this study allow us to draw the following conclusions: cytoflavin accelerates the reverse development of such manifestations of alcohol withdrawal syndrome as arterial hypertension, tachycardia, nausea, vomiting, tremor, sweating, heaviness in the head and headache. Moreover, it is reliable ( p
<0.05) the integral indicator of the severity of alcohol withdrawal on the CIWA-Ar scale decreases (by the 5th day of treatment - by 31.35% compared with the same complex pharmacotherapy, but without cytoflavin);
2) cytoflavin contributes to the reduction of PVA due to a significant ( p
<0.01) decrease in the intensity of its vegetative component, assessed using N.V.’s glossary. Cherednichenko-V.B. Altshuler (by the 5th day of treatment - by 45.64% compared with the same complex psychopharmacotherapy, but without cytoflavin); 3) the introduction of cytoflavin into complex pharmacotherapy is not accompanied by adverse events, which allows us to consider this drug not only effective, but also a safe means for complex detoxification of patients dependent on alcohol.
[]It should be noted that the term “visit” is used conditionally in this work, since all patients who took part in the study were in the hospital.
results
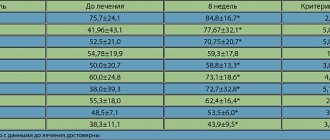
In the table
The characteristics of the patients are presented, including group average indicators on the scales studied.
The distribution of men and women, mean age and level of education did not differ between the groups of patients receiving cytoflavin and the control group.
The average group indicators of asthenia were: 80.3±2.6 and 82.3±3.8 points in the main and control groups, respectively. However, despite the small differences between the group average indicators, they were significant with less severity of asthenia in the main group. At the same time, the level of depression according to Beck and the severity of autonomic disorders according to a questionnaire filled out by a doctor were greater in the group of patients receiving cytoflavin. Indicators of depression and anxiety, identified using the Hospital Depression and Anxiety Scale, as well as the severity of subjective autonomic disorders did not differ in the study and control groups. The frequency of paroxysmal activity according to EEG examination was low in the examined population of patients with asthenia of organic nature. Thus, paroxysmal τ-activity upon admission was detected in 3 patients receiving cytoflavin and in 5 patients in the control group. During re-examination before discharge, paroxysmal τ-activity was detected in the same 8 patients. Epileptic activity was not detected in any case, either during the initial or re-examination.
Cytoflavin was well tolerated; 16 patients receiving cytoflavin and 15 patients in the control group noted moderate sedative effects of standard antidepressant therapy (drowsiness, mild lethargy, slight dizziness). No other complaints were identified in the group of patients receiving Cytoflavin. There were also no new cases of epileptic activity or paroxysmal high-amplitude activity on the EEG recorded after the course of treatment.
The effect of cytoflavin on the level of asthenia and cognitive functions
After an inpatient course of treatment, the level of asthenia decreased to 57.3±6.8 points in the main group and 58.4±6.8 points in the control group, while the positive dynamics of this indicator was highly reliable ( p
<0.001). At the same time, the magnitude of changes in the severity of asthenia symptoms in accordance with the indicators of the asthenic state questionnaire did not differ in the two groups, either with or without using the baseline level of asthenia as a covariate.
The results of the Montreal Cognitive Impairment Scale tests also significantly improved in both examined groups of patients ( p
<0.001).
However, no effect of the drug was detected in the general group of subjects ( p
= 0.224).
It is important to note that in 53 subjects the total score on the Montreal scale already during the initial examination reached the “ceiling” value of 27 to 30 points, i.e. any dynamics of this indicator during repeated examination was impossible. Accordingly, we re-analyzed the dynamics of the results of the cognitive tests of the Montreal scale depending on the drug intake in a group of 35 patients who completed these tests with a score of 21 to 26 points. A significant improvement in the results of performing cognitive tests before discharge compared to the first days of hospitalization was also found in this group of patients ( p
<0.001). It is important that patients receiving cytoflavin (11 patients) demonstrated a more pronounced improvement in the results of cognitive tests upon re-examination compared to the group of patients (24 people) receiving standard therapy (Fig. 1).
Figure 1. Dynamics of the total score on the Montreal Cognitive Impairment Scale depending on cytoflavin intake. Here and in Fig. 2-4: solid line – main group of patients, dotted line – control group. When excluding from the analysis patients who performed Montreal scale tests at a level of 26 points, this trend reached significance ( p
= 0.009).
Effect of cytoflavin on emotional disorders
In both groups of patients, a decrease in the level of depression on the Beck depression scale was recorded before discharge ( p
<0.001).
A more pronounced decrease in depression was found in the group of patients receiving cytoflavin compared to the control group ( p
= 0.004).
However, patients receiving the drug were significantly different from the control group in higher levels of depression during hospitalization ( p
= 0.011).
Thus, in 8 patients from the main group, depression exceeded 35 points on the Beck scale, while in the control group not a single patient had such a high score. In addition, in 4 patients characterized by very low depression scores on admission (3-6 points), dynamics was impossible. Accordingly, we re-analyzed the effect of cytoflavin on the severity of depression after excluding 8 patients with Beck scale scores of 40-47 (Fig. 2)
.
Figure 2. Dynamics of depression according to the Beck scale depending on cytoflavin intake. The trend toward a more pronounced decrease in depression in patients receiving Cytoflavin compared with the control group remained significant in repeated analysis ( p
= 0.045). It should be noted that the positive effect of cytoflavin on the dynamics of depression was more pronounced in men, but gender differences in this indicator did not reach statistical significance.
Depression and anxiety, as measured by the Hospital Depression and Anxiety Scale, also decreased significantly before discharge in both groups of patients ( p
<0.001), however, the decrease in anxiety level was significantly greater in the group that did not receive cytoflavin (
p
= 0.008) compared with patients treated with cytoflavin
(Fig. 3)
.
Figure 3. Dynamics of depression and anxiety according to the Hospital Depression and Anxiety Scale depending on cytoflavin intake. The dynamics of anxiety depending on the intake of cytoflavin did not differ between men and women; in other words, a more pronounced decrease in anxiety in patients who did not receive cytoflavin was observed both in the group of men ( p
= 0.043) and in the group of women (
p
= 0.079).
Effect of cytoflavin on autonomic disorders
The severity of objective and subjective autonomic disorders significantly decreased in the examined group of patients with emotionally labile disorder after an inpatient course of treatment compared to the period before treatment ( p
<0.001).
Patients treated with cytoflavin showed a tendency towards a more pronounced normalization of autonomic functions according to the corresponding questionnaire compared to patients not treated with cytoflavin ( p
= 0.076). This trend was expressed to the same extent in both the subgroup of men and the subgroup of women.
As noted above, autonomic disorders, as examined by a physician, were significantly more pronounced in the group of patients receiving Cytoflavin. However, as can be seen in Fig. 4
, there were no intergroup differences in the dynamics of objective symptoms of autonomic dysfunction depending on the intake of cytoflavin (
p
= 0.24).
Figure 4. Dynamics of autonomic disorders according to the questionnaire by A.M. Vein depending on the intake of cytoflavin.
Effect of cytoflavin on quality of life
Group mean scores on all 8 SF-36 subscales improved at re-examination compared with examination at admission ( p
<0.001), but these changes did not depend on cytoflavin intake.
Cytoflavin
Metabolic drug. Pharmacological effects are due to the complex action of the components that make up the drug Cytoflavin®.
Succinic acid is an endogenous intracellular metabolite of the Krebs cycle, which performs a universal energy-synthesizing function in the cells of the body. With the participation of the coenzyme flavin adenine dinucleotide (FAD), succinic acid is quickly transformed by the mitochondrial enzyme succinate dehydrogenase into fumaric acid and then into other metabolites of the tricarboxylic acid cycle. Stimulates aerobic glycolysis and ATP synthesis in cells. The end product of succinic acid metabolism in the Krebs cycle is carbon dioxide and water. Succinic acid improves tissue respiration by activating electron transport in mitochondria.
Inosine is a purine derivative, a precursor to ATP. It has the ability to activate a number of Krebs cycle enzymes, stimulating the synthesis of key nucleotide enzymes - FAD and NAD.
Nicotinamide (vitamin PP), nicotinic acid amide. Nicotinamide in cells, through a cascade of biochemical reactions, is transformed into the form of nicotinamide adenine nucleotide (NAD) and its phosphate (NADP), activating nicotinamide-dependent enzymes of the Krebs cycle, necessary for cellular respiration and stimulation of ATP synthesis.
Riboflavin (vitamin B2) is a flavin coenzyme (FAD) that activates succinate dehydrogenase and other redox reactions of the Krebs cycle.
Thus, all components of the drug Cytoflavin® are natural metabolites of the body and stimulate tissue respiration. Metabolic energy correction, antihypoxic and antioxidant activity of the drug, which determine the pharmacological properties and therapeutic effectiveness of the components, is due to the complementary action of succinic acid, inosine, nicotinamide and riboflavin.
Pharmacokinetics
Cytoflavin® has high bioavailability.
When taken orally, succinic acid is absorbed from the gastrointestinal tract, enters the blood and tissues, participating in energy metabolism reactions, and completely decomposes to the final metabolic products (carbon dioxide and water) after 30 minutes.
Inosine is well absorbed from the gastrointestinal tract. Tmax in the blood is 5 hours, the average retention time in the blood is 5.5 hours, Vd at steady state is about 20 l. Inosine is metabolized in the liver to form inosine monophosphate, followed by its oxidation to uric acid. A small amount is excreted by the kidneys.
Nicotinamide is quickly distributed in all tissues (Vd at steady state is about 500 l). Tmax in the blood is 2 hours, the average retention time in the blood is 4.5 hours. Metabolized in the liver to form N-methylnicotinamide. Excreted by the kidneys. Nicotinamide penetrates the placental barrier. Passes into breast milk.
Riboflavin is quickly absorbed from the gastrointestinal tract, distributed unevenly (the largest amount in the myocardium, liver, kidneys), and is transformed into flavin adenine mononucleotide (FMN) and FAD in mitochondria. Penetrates through the placental barrier. Excreted in breast milk. It is excreted by the kidneys, mainly in the form of metabolites.
Discussion
The results of the study indicate that cytoflavin at a dose of 4 tablets per day (in 2 doses) has a positive effect on cognitive functions in patients with organic brain damage. Data from a previous study [6] regarding the positive effect of cytoflavin on depressive symptoms in patients with severe asthenia were confirmed. At the same time, in contrast to a multicenter study that included patients with cerebrovascular disease [4], we did not detect an additional effect of cytoflavin on the overall positive dynamics of asthenic symptoms in patients with emotionally labile disorder. We observed a pronounced regression of asthenia symptoms regardless of cytoflavin intake. It should be noted that the average age of the examined patients was significantly lower compared to the specified multicenter study [6], which included patients with cerebrovascular disease and demonstrated a more pronounced reduction in asthenia during treatment with cytoflavin. It can be assumed that the effectiveness of cytoflavin manifests itself mainly in patients with reduced neurotrophic resources. Indirect confirmation of this hypothesis is a more pronounced improvement in cognitive status while taking cytoflavin in patients with cognitive impairment compared to the control group in our study.
In patients treated with cytoflavin, a significantly more pronounced decrease in the Beck depression score and normalization of autonomic regulation were found compared to the control group. Interestingly, in our previous study involving patients with organic depression, a similar effect of cytoflavin was observed only in a subgroup of women. In the present study, the effect of cytoflavin was more pronounced in the subgroup of men with emotional labile disorder compared to the subgroup of women. Our data are consistent with previous experimental and clinical studies demonstrating the antidepressant effect of nootropics [13–15]. Numerous neuroimaging and experimental studies have revealed a deficit in neurotrophic processes in patients with chronic depression, leading to hypotrophic changes in the frontal cortex and other brain structures in such patients [16-18]. Thus, the effectiveness of prescribing cytoflavin as an additional method of treating depression seems pathogenetically justified.
It is well known from clinical practice that most nootropic drugs have a stimulating effect on the functions of the central nervous system. It is likely that the stimulating effect of cytoflavin was the reason for less regression of anxiety symptoms in the group of patients receiving the drug compared to the control group. Accordingly, the possibilities and limitations of nootropic therapy in patients with anxiety disorders require further research.
Thus, the data from the present observational study indicate that cytoflavin is well tolerated by patients with organic emotionally labile (asthenic) disorder and helps to normalize cognitive functions, mood and autonomic regulation in such patients. The effectiveness of cytoflavin as a treatment for asthenia in young patients requires further research.