Back pain can be a symptom of lumbodynia, radiculitis and lumbar sciatica syndrome. In the latter case, low back pain spreads to one or both lower limbs. If the pain is acute, of a pronounced nature, this is acute lumboischialgia. If the pain is moderate and bothers you for a long time with periodic exacerbations, this is chronic lumboischialgia.
What does the word lumboischialgia mean?
Sciatica is pain in the lower back that extends to one or both lower limbs. It is a reflex syndrome and belongs to the non-radicular phase of lumbar osteochondrosis, as well as lumbodynia and lumbago. Therefore, it would be more correct to say that there is lumboischialgia syndrome on the right or lumboischialgia syndrome on the left.
What is “discogenic lumboischialgia”?
If during diagnosis it is established that the cause of such complaints is a disc herniation or protrusion, then we can say that this is discogenic lumboischialgia.
How is it going?
If the pain occurs acutely and is of a pronounced nature, then this is acute lumboischialgia. If the pain is moderate and bothers you for a long time, periodically exacerbating, this is chronic lumboischialgia.
What can lumboischialgia be?
Depending on the nature of neurological disorders, vascular, muscular-tonic, and muscular-dystrophic forms of lumboischialgia are distinguished.
What causes lumboischialgia syndrome to appear?
Vertebrogenic lumboischialgia syndrome most often occurs after hypothermia, as well as after increased stress on the muscles of the lower back and legs. As a result, tonic muscle strain occurs and pain appears in the lower back and leg.
Prevention
- it is necessary to promptly treat diseases and get rid of problems in the joints, blood vessels, and spine;
- Avoid situations with hypothermia and injuries if possible;
- control of correct posture and weight control;
- wear comfortable shoes;
- you need to lift heavy objects correctly, and it is better to avoid lifting heavy objects;
- sedentary work requires a comfortable workplace, short breaks and warm-up for a few minutes;
- if the activity involves long car trips, you need to stop more often to warm up;
- lead a healthy active lifestyle;
- chronic lumbar ischialgia requires regular sanitary and spa treatment;
Any form of lumbar ischialgia requires a mandatory clinical examination. At the “Medical Center YES!” The neurologist, after examining and collecting anamnesis, will definitely prescribe additional instrumental and laboratory examination of the patient, necessary to assess the condition of the spine, bones and joints, in order to differentiate the disease, to identify, if any, pathologies of the blood vessels of the abdominal cavity and lower extremities . Additional studies help exclude fractures, tumor processes and other conditions and diseases.
Make an appointment with a neurologist at the “YES Medical Center!” possible by phone or by filling out the form on the website.
Our licenses for medical activities
All rights reserved by copyright law. No part of the contents of the site may be used, reproduced, transmitted by any electronic, copying or other means without the prior written permission of the copyright owner.
Symptoms of lumbar sciatica and diagnosis of lumbar sciatica
The main complaints are pain in the lower back and legs. Both lumbar sciatica on the right and lumbar sciatica on the left are equally common, but bilateral lumbar sciatica is much less common. The pain is usually not as severe as with lumbago and the radicular stage of lumbar osteochondrosis (radiculitis). However, they are more intense than with chronic lumbodynia. Most often, the pain is severe or moderate in nature.
According to the subjective characteristics, it is aching, burning, squeezing, localized in the lower back or leg.
Vascular disorders in lumboischialgia
Vessels are narrowed
Studies have shown that the vascular tone of the legs in patients with lumboischialgia is most often increased. This is a vasospastic variant of this syndrome. In other words, the vessels are narrowed in this case.
And if vascular tone is increased, then patients note chilliness in the leg. She may be paler and colder to the touch than healthy. And the temperature in the lower leg and foot of the diseased leg is slightly lower than the healthy one. The most interesting thing is that after physical activity the temperature difference only increases. On the sore leg, the temperature drops even more, while under normal conditions it should rise. Temperature asymmetries are detected not only on sore and healthy legs. In some cases, even in a limited area of the affected leg, the temperature may be different at nearby points.
Vessels are dilated
When vascular tone is reduced, this is a vasodilatory variant of lumbar ischialgia syndrome. However, this manifestation is much less common. But if vascular tone is reduced, then a feeling of heat or warmth appears in the affected limb, and its temperature rises. (V. P. Veselovsky)
Symptoms of the disease
The main symptom of lumboischialgia is acute lumbago (sharp pain of a shooting nature) in the buttocks and back of the legs, radiating to the lower extremities. The pain is provoked by sudden movements, lifting heavy objects, sneezing, coughing. Attacks can last several minutes or several days.
The patient may experience other symptoms:
- decreased or loss of sensitivity in the skin of the buttocks and affected leg;
- stiffness in the lower back;
- muscle tension;
- pain when standing on your leg;
- cramps in the calf muscle;
- numbness of the toes;
- pallor of the skin in the sacral area;
- increased body temperature;
- chills and fever;
- weakness in the legs;
- indigestion;
- difficulty and pain in urination and defecation;
- itching, burning or subcutaneous throbbing.
If left untreated, blood circulation is impaired. Over time, lumbago with sciatica can cause urinary and fecal incontinence, sexual dysfunction, cause a decrease in muscle mass in one limb, and lead to disability.
Autonomic disorders in lumboischialgia
When examining patients, a large number of autonomic disorders are determined. Initially, there is limited pallor of the nail phalanges of the toes. But in the future, the entire foot may turn pale. This process is often accompanied by a feeling of numbness, as well as other unpleasant sensations: burning, tingling, distension. In some cases, the pallor of limited areas of the skin of the leg is replaced by moderate cyanosis. These disorders are clearly identified after hypothermia, especially after work associated with high humidity.
Disc protrusion or herniation
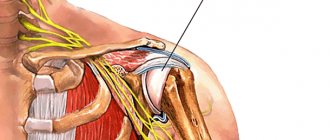
Disc protrusion is a condition when the central gel-like part of the disc (nucleus pulposus) protrudes towards the spinal canal, while the integrity of the outer wall of the disc (annulus fibrosus) is not compromised. A disc herniation occurs when the nucleus pulposus extends beyond the annulus fibrosus. With protrusion or herniation of the disc, the protruding part of the disc can compress the adjacent nerve root and cause sciatica. The consequences of a herniated disc are worse. In this case, the prolapsed disc core not only causes direct compression of the nerve root, but at the same time the disc substance contains an acid, a chemical irritant (hyaluronic acid), which causes inflammation of the nerve. Nerve compression and irritation cause inflammation and pain, often leading to limb numbness, tingling, and muscle weakness.
Factors contributing to the occurrence of lumboischialgia
If a person is bothered by chronic vertebrogenic lumboischialgia, then diseases of various internal organs and the central nervous system are often detected. On the part of the central nervous system, these are, as a rule, residual effects of inflammatory and traumatic brain damage. Based on experimental studies, it has been established that the creation of additional foci of damage even outside the spine contributes to the occurrence of lumbar osteochondrosis. These lesions can be in the brain, muscles and internal organs. (V. P. Veselovsky)
Reflex curvature of the spine with lumboischialgia
In addition to pain and various autonomic disorders, patients with lumboischialgia often have reflex deformities of the lumbar spine. This manifestation is called antalgic scoliosis. It was believed that in most cases it was of a protective nature, as if helping to reduce irritation of the sinuvertebral nerve.
However, quite often, especially in young people, these curvatures remain for a long time, even after a significant reduction in pain. Therefore, reflex deformation of the spine cannot be considered as a physiologically useful mechanism. And also consider that this mechanism is aimed at reducing irritation of sensitive nerve formations, which are the source of pain. It would be more correct to say that there is vertebrogenic lumboischialgia with reflex muscular-tonic syndrome.
Diagnostic methods
Standard methods for diagnosing lumboischialgia syndrome are radiography of the pelvic and sacral region, computed tomography and MRI of the lumbosacral spine. Today, the most sensitive and informative method is magnetic resonance imaging, but the diagnostic method is prescribed by a specialist based on the medical history of a particular patient. An examination of the pelvis and abdomen may also be done to rule out organ damage, which may also be causing pain.
Treatment of lumboischialgia
Before talking about how lumbar sciatica is treated, it is important to note that drug treatment, physiotherapeutic procedures, and exercises for lumbar sciatica are best determined individually. And you need to proceed from the characteristics of each specific case and stage of the process.
- To relieve pain, drug therapy and physiotherapy are prescribed. If there are indications, then medical therapeutic blockades are used. They are performed by a doctor. The medicine is injected paravertebrally, as well as into trigger points on the sore leg. As a rule, droppers with decongestants and anti-inflammatory drugs are prescribed.
- It is recommended to fix the lumbar spine using an orthopedic semi-rigid dynamic corset. This also helps reduce pain, because it reduces the load on the spine.
- Functional disorders (blocks) in the functioning of the spine must be identified. This is done by a chiropractor. And this is necessary because it is the incorrect functioning of the spine that leads to the development of osteochondrosis, and ultimately to the appearance of protrusions and herniations of intervertebral discs. First, manual diagnosis is performed, and then manual therapy. Typically, there are an average of seven to ten procedures per course.
- In order to stimulate recovery processes, physiotherapeutic procedures, reflexology, and massage are prescribed.
- Physical therapy is very important.
Forecasts and possible consequences
First of all, it is worth saying that any back disease is potentially dangerous due to the proximity of the lesion to the nerve structures. The immediate consequences of late or absent treatment are tissue deformation, the formation of muscle knots and metabolic disorders.
Only a doctor can give an individual prognosis for a patient’s recovery. However, statistics say that 95% of cases of lumboischialgia have a benign course . Timely diagnosis is important: the sooner you see a doctor, the higher the likelihood of recovery with minimal possibility of relapse and the easier the treatment will be. To do this, it is necessary to follow preventive measures and take care of your health.
The importance of physical therapy
Gymnastics for lumboischialgia should initially be aimed at eliminating muscle spasms. Equally - to relieve muscle swelling and venous stagnation in them and the roots of the intervertebral foramina. Ultimately, the goal of therapeutic exercise is to optimize the movement pattern. In other words, it is necessary to make the spine work more correctly, without overloading any of its segments. This is necessary to ensure that the disks do not fail prematurely. And new hernia protrusions did not appear in them, and old ones did not increase. All physical therapy should be built taking into account the individual characteristics of the patient. This is posture, features of the location of hernias and protrusions of intervertebral discs. Physical therapy exercises in combination with manual therapy are not only the prevention of relapses in chronic vertebrogenic lumbodynia. They are a prevention of the degenerative-dystrophic process (osteochondrosis of the spine), as such.
Low back pain (LBP) is one of the leading complaints among residents of Western industrialized countries; 84% of the population experiences it during their lifetime [1]. The economic costs associated with PPO and the impact on the healthcare system are comparable to those associated with cardiovascular diseases, diabetes mellitus and depression [2]. The results of an epidemiological study, which included a survey of more than 46,000 residents of European countries and Israel, showed that 24% suffer from chronic LBP, and 8% of the population suffer from neck pain [3]. The prevalence of chronic back and neck pain among the adult population of the Russian Federation is 42.4–56.7% [4]. Pain ranks first in the structure of people seeking medical help. According to a study conducted in Moscow, of 1,300 patients who sought outpatient care, in 24.9% the main reason for seeking treatment was BPO [5].
LBP in 25–57% of cases is accompanied by the development of pain in the extremities [6], these cases account for a disproportionately high amount of treatment costs and compensation for disability [7]. Irradiation of pain to the lower extremities is an important factor in predicting the likelihood of pain becoming chronic; it serves as an indirect indicator of the severity of the disease. Often, it is not possible to identify the primary mechanism leading to irradiation of pain in lumboischialgia, since there are many structures that can cause similar symptoms [8].
When surveying the population of Novosibirsk, it turned out that the majority of patients suffering from pain for a long time prefer to be treated independently. The reasons for refusing medical care are uncertainty about its effectiveness and low availability of qualified care. Only 48.2% of patients periodically consult doctors of various specialties. Of the 233 patients who sought consultation at the clinic, 66% used analgesics irrationally, 60% had unreasonable examinations, and 70% received an incorrect explanation from doctors about the origin of pain [4]. The inability to determine the nature of referred pain within the framework of BPO is a common mistake, as a result of which doctors prescribe unreasonable diagnostic procedures and treatment [8]. Thus, irradiation of pain to the lower extremities with BPO can occur as a result of damage or dysfunction of the structures of the nervous or musculoskeletal system. Possible causes of damage to the structures of the nervous system include both mechanical factors (protrusion of the intervertebral disc) and biochemical factors, which are characterized by an increase in the production of cytokines and other inflammatory mediators. On the one hand, as a result of such changes in the nervous system, disturbances in sensory and motor functions occur, and on the other hand, the appearance of paresthesia and hyperalgesia, usually associated with central sensitization. Isolated nerve damage does not always lead to pain [9], and signs of compression of the spinal cord roots may be absent during neuroimaging studies in patients with BPO [10]. Despite the fact that the clinical determination of the specific mechanism of development of the pain syndrome is a difficult task, the use of expanded protocols for the management of such patients with a detailed neurological examination and assessment of the sensitization of the nervous system to mechanical stimuli could clarify the understanding of the pathogenesis of certain symptoms of lumboischialgia. It is proposed to classify lumboischialgia in accordance with the leading pathogenetic mechanism into four types. Each type is characterized by the predominance of certain processes, for example, the phenomena of central sensitization, denervation as a result of pronounced axonal damage without signs of damage to the central nervous system, peripheral sensitization due to local inflammatory processes in peripheral nerves without signs of denervation, or a musculoskeletal component, which is based on changes structures not related to the nervous system (intervertebral disc, facet joint) [11].
The difficulties in treating such patients are largely associated with insufficient understanding of the mechanisms of development of PPO, the lack of possibility of individualized and differentiated therapy in the current conditions of organizing pain care. In this regard, the first step towards solving this problem should be the study of the pathophysiological mechanisms underlying the formation of pain in general and lumboischialgia in particular.
Mechanism of development of lumboischialgia
According to the mechanisms of development, back pain can be represented by nociceptive, neuropathic and psychogenic components. Nociceptive pain is associated with the activation of pain receptors - nociceptors, while neuropathic pain is a consequence of disease or damage to the somatosensory system [12]. Neuropathic back pain is usually associated with damage to the roots during the formation of a herniated intervertebral disc; it can occur with spinal stenosis, spondylolisthesis, compression of the spinal roots by osteophytes and hypertrophied facet joints. As a rule, such pain radiates to the limbs and is accompanied by other symptoms of root damage. The psychogenic component of back pain is associated with the patient’s personality characteristics, increased levels of anxiety, depression, inadequate understanding of the origin of pain, and may be accompanied by mental disorders.
Judgments about the prevalence and origin of neuropathic back pain have changed significantly in recent years, which is associated with epidemiological studies. It has been shown that in European countries its prevalence is 6–7.7% [13]. According to a clinical and epidemiological study of the prevalence of neuropathic pain, carried out under the auspices of the Russian Society for the Study of Pain, the prevalence of any pain among patients who consulted a neurologist was 39%, and neuropathic pain or its components was 18% of all patients at an outpatient appointment, with This neuropathic component was noted in 35% of patients with back pain [14]. The costs of treating such patients are 70% higher than for patients with nociceptive BPO [15].
To date, the term “neuropathic back pain” remains poorly defined. The data obtained allow us to conclude that the concept of neuropathic back pain is not limited to classical radiculopathy and is implemented by a number of pathophysiological mechanisms [16].
Inflammation
The main cause of lumboischialgia and radiculopathy is considered to be pathology of the intervertebral discs [17]. Of greatest importance are the appearance of gaps in the annulus fibrosus (AF), prolapse or sequestration of the nucleus pulposus (NP), which contribute to the development of inflammation of the spinal roots, often not accompanied by their mechanical compression. Substance P.Ya. is a chemical irritant for nervous tissue and, due to this, contributes to the occurrence of local inflammation, which also affects the development of lumboischialgia [18]. One of the causes of the inflammatory process is considered to be a fracture of the endplates, in which the contents of the ulcer may enter the bloodstream, triggering the degradation of the ulcer matrix [8]. Degenerative changes in intervertebral discs often result in rupture of the disc, triggering inflammatory reactions in the disc that spread throughout its entire length, reaching the outer third of the disc, which is supplied with nerve endings [19]. The substances released in this case can cause activation of nociceptors, leading to the development of discogenic radicular pain syndrome [20]. With a complete rupture of the FC, the contents of the PN and pro-inflammatory mediators can penetrate into the spinal canal, irritating the nerve endings of the incoming or outgoing roots of the spinal cord and causing inflammatory processes in them [19]. The most important pro-inflammatory cytokine is interleukin 6 (IL-6), the concentration of which increases with macrophage infiltration [21]. An increase in IL-6 levels is one of the leading mechanisms for the development of neurological symptoms, in particular neuropathic pain [21]. Increasing levels of pro-inflammatory cytokines such as tumor necrosis factor-alpha and NO, secreted on the surface of PJ cells, contribute to an increase in the neuropathic component of the pain syndrome [18]. The inflammatory process leads to an increase in the density of sodium channels and improved conductivity in the spinal roots of the spinal cord, which contributes to the appearance of foci of ectopic excitation with increased sensitivity of nerve fibers to mechanical stimuli [22].
The above hypothesis of biochemically caused damage to the spinal cord roots was confirmed by the study of local inflammatory processes in the spinal roots in experimental studies, the results of which demonstrated the formation of pain behavior with the phenomena of allodynia and hyperalgesia in the absence of axonal damage [23].
Another study showed that locally induced neuritis of the peroneal and sciatic nerves may be due to compression and stretching of the mechanoreceptors of the nerve trunks [24]. It turned out that after irritation of the spinal roots with the contents of the PU, lower threshold values of mechanical, thermal and pain sensitivity were observed in the presence of minor signs of axonal damage, which may contribute to the irradiation of pain during movement [24]. Patients with nonspecific pain syndrome in the arm after whiplash developed motor impairment due to damage to the median nerve and increased sensitivity of nerve fibers to mechanical stimuli, in particular, pressure and stretch. The data obtained suggest that inflammation associated with trauma may contribute to the spread of the process to undamaged areas of nerve fibers, causing increased sensitivity to mechanical stimuli and damage to peripheral nerve endings [25].
Compression of the spinal roots
Mechanical compression of the spinal roots can be caused by a herniated intervertebral disc, osteophytes, hypertrophied facet joints, and ligamentum flavum [26]. These changes can cause local circulatory disorders, increased endoneurial pressure and deformation of nerve fibers [18]. The combination of increased endoneurial pressure and impaired circulation of spinal tissue can lead to ischemia of nervous tissue with destruction of the myelin sheaths of nerves [26]. Such damage can cause sensory and motor disturbances and the appearance of radiating pain. Contrary to this assumption, there is another point of view that compression of the spinal roots does not always cause the development of pain syndrome [27]; The reason for this phenomenon has not been fully studied. The absence of pain may be due to the degree of compression of the spinal nerve. In the case of rapidly progressing compression of the root, the symptoms that arise are usually associated with the inflammatory process and irritation of the nerve endings [26]. With slowly progressive root compression, symptoms increase gradually [18], but this phenomenon is less studied. Although the extent of acute and chronic nerve damage is difficult to assess in experimental studies, changes in the case of rapidly progressive compression are likely to be more pronounced [17, 18]. Chronic, slowly progressive compression of the spinal roots is characteristic of a gradual narrowing of the lumen of the spinal canal during its stenosis, for which the development of an inflammatory process is uncharacteristic. In this case, pain usually appears after prolonged exercise, in particular walking, prolonged standing [28], causing narrowing of the spinal and/or foraminal canals, contributing to vascular compression and ischemia of the roots [29].
Damage to the central part of nociception
Prolonged delivery of nociceptive stimuli from the peripheral nervous system, resulting from inflammation or compression of nerve structures, can lead to the development of additional reactions from the central nervous system, which are considered as central sensitization [30]. The most significant events occur in the cells of the dorsal horn of the spinal cord. It is here that high-intensity activation of nociceptors, especially C-fibers, is supported, in which phosphorylation of NMDA receptors of specific nociceptive neurons of the dorsal horn takes part. Thus, as part of long-term effects, receptor excitability may change. Thus, under conditions of peripheral sensitization, subthreshold values of C-fiber impulses are capable of causing excitation of the postsynaptic membrane [16]. One of the subtypes of neurons in the dorsal horn of the spinal cord are convergent neurons .
.: wide dynamic range, WDR), which, along with nociceptive ones, are also activated by non-nociceptive impulses. The involvement of WDR neurons in the pathological process enhances the transmission of tactile sensitivity impulses along Aβ fibers, as a result of which non-painful stimuli are perceived as pain. At the same time, nerve damage leads to changes in the properties of Aβ fibers, which acquire the properties of nociceptive fibers, releasing modulating neuropeptides, as a result of which the altered fibers are able to cause central sensitization [31]. This phenomenon is also known as Aβ fiber phenotypic variability. By analogy with nociceptive ones, Aβ fibers can grow into lamina II of the dorsal horn, where afferent nociceptive impulses arrive [32]. Sensitization of WDR neurons and phenotypic variability of Aβ fibers lead to the development of pain in response to non-painful stimuli (allodynia), which in turn triggers the processes of central sensitization. In addition to increased pain impulses, spontaneous activity of central nociceptive neurons can be caused by a decrease in the propagation of sensory impulses (deafferentation) due to damage to the axons of primary afferent neurons [33]. Weakening of inhibitory mechanisms also contributes to increased pain due to the death of interneurons in the pain impulse transmission system of the dorsal horns of the spinal cord [31]. In addition, changes are found in the descending modulatory system of the cerebral cortex, which also leads to increased pain. Secondary changes in cortical and subcortical structures, taking into account cognitive functions and with the participation of emotional reactions, also enhance the phenomena of central sensitization and contribute to the appearance of foci of ectopic excitation and pain [34].
Irradiation of pain syndrome with damage to the musculoskeletal system
A significant group of pain syndromes in lumboischialgia represents damage to the musculoskeletal system [8]. It has been proven that pain in the lower extremities can occur due to damage to the intervertebral disc [20], facet [35] and sacroiliac joints, and muscle structures [36]. This relationship can be explained by convergence theory. In the area of the postcentral gyrus of the cerebral cortex, there is a somatotopic projection of afferent conductors from different parts of the body, in which sensory impulses converge, forming a somatotopic representation of the area in accordance with the area innervated by the spinal nerve [37]. Thus, afferent impulses from the surface of the thigh, lower leg and foot also arrive in the projection area, where information from the spinal root L5 is received. Upon reaching a certain intensity, pain impulses from the facet joints or disc can activate the projection zones of the cortex, due to second-order neurons; the signal is processed in such a way that the source of pain is the fibers of the lower extremities and the musculoskeletal structures of the lumbar region [38].
Identification of the neuropathic component of lumboischialgia
Peripheral neuropathic mechanisms are under constant control of the facilitating and inhibitory influences of the central nervous system. The diversity of pathophysiological mechanisms underlying neuropathic pain reflects a high level of heterogeneity in the plasticity of the central and peripheral nervous systems, but the measure of plasticity is difficult to determine clinically [39].
Interestingly, neuropathic pain occurs only in a proportion of patients who have damage to the nerve structures that can cause its development. Imaging studies reveal obvious spinal root compression/displacement in 4–17% of a population of healthy adults without any history of pain [40]. J. Mogil and M. Max [40] suggest that “like all biological phenomena, this variability is caused by a combination of as yet unidentified genetic and environmental factors” [41]. In turn, clinicians should remember the complex of biopsychosocial influences that ensure the transition of pathological changes into pain and healthy ones into patients.
To answer emerging questions, additional research and, possibly, a different perspective on the concept of neuropathic pain are required. Attention should be paid to the opportunities that currently exist to identify the neuropathic component of back pain and use adequate approaches to its correction. The clinical features of the neuropathic component of GPO need to be clearly defined. For this purpose, questionnaires are used, a clinical examination is carried out, and the method of quantitative sensory testing is used. Identification of the neuropathic component of back pain is based on the recognition of various pain-related symptoms, reflecting the predominance of certain mechanisms of its formation. Symptoms reflecting the presence of a neuropathic component include pain with a burning or electrical sensation, dermatomal pain, spontaneous pain, paroxysmal pain, dysesthesia, allodynia and hyperalgesia [42].
To identify neuropathic pain, screening scales have been developed: LANSS (Leeds Assessment of Neuropathic Symptoms and Signs), S-LANSS (self-report LANSS), DN4 (Douleur Neuropathic 4 Questions), Pain DETECT, Neuropathic Pain Questionnaire, ID Pain, StEP (Standardized Evaluation of Pain). Each scale characterizes neuropathic pain by identifying and assessing symptoms of loss of function and irritation, including spontaneous pain, paresthesia, dysesthesia, allodynia, and motor and sensory deficits. Given the importance of identifying neuropathic pain for further treatment, the reliability, validity and diagnostic accuracy of such scales is imperative. The Pain DETECT [41] and Standardized Evaluation of Pain (StEP) [42] questionnaires have been developed and validated specifically for patients with disorders associated with MPD. These scales allow discrimination between neuropathic and non-neuropathic pain patterns based on verbal descriptors with limited or no clinical examination.
Types of lumboischialgia in accordance with the leading pathogenetic mechanisms
Lumboischialgia with a predominance of central sensitization
Some patients complain of paresthesia, dysesthesia, hyperalgesia, mechanical dynamic allodynia and spontaneous pain caused by central sensitization [33]. To identify the clinical characteristics of the central component, pain descriptors such as “shooting”, “stabbing”, “burning” are used. Patients complain of episodic pain and dynamic mechanical or thermal allodynia. On examination, signs of allodynia are detected by light touch and irritation with needle pricks [43]. The role of central sensitization in the formation of sensitivity disorders has been studied in a number of studies. The leading role of mechanical and thermal hyperalgesia in the development of central sensitization in patients with acute and chronic pain syndrome as a result of whiplash injury has been confirmed [44]. It is believed that mechanical hyperalgesia is one of the components of a complex regional pain syndrome, in the development of which, along with neuroimmune processes, central sensitization plays a significant role [45]. It is advisable to further study the nature of the relationship between mechanical and/or thermal allodynia and central sensitization due to damage to the spinal roots at the lumbar level.
Lumboischialgia with development of denervation
Structural damage to the nerve leads to denervation, resulting in sensory or motor deficits [33]. Radiculopathy is characterized by the presence of objective sensory and/or motor disorders due to disruption of signal transmission along axons at the level of spinal nerves or their roots [46], which is one of the most common causes of neuropathic pain [47]. On examination, there are signs of sensory or motor deficits.
Lumboischialgia with a predominance of peripheral sensitization
Peripheral sensitization is mainly caused by a response to inflammation of the spinal nerve root or set of nerves, resulting in adverse reactions from the nervous system. This phenomenon also occurs with minor lesions of the nervous system, reflecting the slightest changes in the functional state of the nerves [25]. One of the clinical symptoms characteristic of this type is the irradiation of pain into the lower limb, provoked by movement and displacement of anatomical structures. In case of severe pain, the patient takes a forced position in order to immobilize certain parts of the body, minimizing the activation of mechanoreceptors. During the examination, there are no gross changes in the nervous system, however, when carrying out a number of tests (palpation in the projections of the nerves, symptoms of tension), corresponding symptoms are noted [48].
Lumboischialgia in musculoskeletal pathology
Lumboischialgia in musculoskeletal pathology is characterized by the appearance of pain in the lower extremities, which extends to the level of the knee joint or even the foot [20]. The pain is usually dull, aching or pressing in nature [49]. The examination results do not reveal any pathology. Dysfunction of the sacroiliac joints and symptoms of “centralization” of the pain syndrome are possible; other structures involved in maintaining pain are also found [49]. Signs of damage to small-caliber nerve fibers are usually absent, although a higher threshold of superficial sensitivity may be detected [50].
Mixed forms of lumboischialgia
In accordance with the proposed criteria, four leading mechanisms for the development of lumboischialgia can be identified, and in practice they often have much in common. Peripheral sensitization reactions can trigger central sensitization reactions, and inflammatory products released during denervation can disrupt the properties of nerve fibers. The possibility of the appearance of competing types of lumboischialgia in one patient cannot be excluded, since the vast majority of cases of BPO include both nociceptive and neuropathic components. It should be remembered to identify the predominant mechanism for the development of lumbar ischialgia in a given patient, primarily on the basis of his complaints, which is possible with the correct algorithm for examining the patient.
Treatment of patients with lumboischialgia with a neuropathic component
Treatment of a patient with pain syndrome should be carried out in accordance with the recommendations of competent organizations and scientific communities, based on the principles of evidence-based medicine. For drug treatment of pain, it is advisable to use drugs with level of evidence of effectiveness, A or B. According to the European Federation of Neurological Societies Guidelines for the drug treatment of neuropathic pain, drugs with established effectiveness based on class I studies are pregabalin, gabapentin, tricyclic antidepressants (TCAs), duloxetine, venlafaxine (level of evidence A).
Pregabalin (Lyrica) is a modern antiepileptic drug that has proven itself to be an effective treatment for any neuropathic pain, fibromyalgia, and anxiety. Pregabalin is a gamma-aminobutyric acid analogue with high selectivity for the α-2-delta subunit of the neuronal voltage-gated calcium channel. In placebo-controlled clinical studies, pregabalin demonstrated not only high anti-pain activity, but also effectiveness against concomitant mood disorders and insomnia in patients with peripheral diabetic polyneuropathy, postherpetic neuralgia, and spinal central neuropathic pain. A study of the effectiveness of pregabalin (Lyrica) in patients with cervical and lumbar radiculopathy was conducted in real clinical practice. A more than 2-fold reduction in pain was observed in 63% of patients receiving pregabalin monotherapy and in 56% of patients receiving pregabalin as an addition to standard therapy, which included non-steroidal anti-inflammatory drugs, gabapentin, amitriptyline and fentanyl.
A domestic study also demonstrated the high effectiveness of pregabalin (Lyrica) in the treatment of neuropathic pain in spondylogenic lumbosacral radiculopathies. It has been established that in some patients, even in the presence of obvious signs of radiculopathy, the neuropathic component is not dominant in the structure of the pain syndrome, and therefore such patients are required to undergo mandatory testing using the DN-4 questionnaire for the differential diagnosis of nociceptive and neuropathic pain [51].
In the treatment of neuropathic pain, the effectiveness of oxycodone (37-60 mg/day) and tramadol (200-400 mg/day), which have opioidergic and monoaminergic effects, has been shown. It is advisable to prescribe pregabalin or gabapentin, TCAs as first-choice drugs. The use of TCAs requires caution in elderly patients with cardiovascular risk factors. Treatment with amitriptyline should begin with small doses (10-25 mg at bedtime), gradually increasing them according to tolerance. The effective dose is variable, averaging 75 mg/day [52, 53].
Most researchers agree on the effectiveness of an integrated multidisciplinary approach in the treatment of pain, including pharmacotherapy, motor rehabilitation, psychotherapy in combination with reflex methods. It has been shown that the use of reflex anesthesia in complex therapy of neuropathic pain can significantly increase its effectiveness [54, 55].
There is evidence to suggest that back pain is not directly related to structural changes in the spine. Researchers agree that blue pain cannot be fully explained by either genetic or environmental factors. The comorbidity of BPO and other chronic pain syndromes and mental disorders has been proven. Chronic LBP may be a condition pathogenetically close to dysfunctional pain syndromes - fibromyalgia, irritable bowel syndrome, interstitial cystitis, etc. Changes in the functional and structural state of the central nervous system in patients with chronic back pain are shown using functional MRI and morphometric studies; Cognitive impairment was noted in this category of patients. It has been shown that changes in the activity of spinal cord neurons can occur not only when peripheral sources of pain persist, but also when the functional state of other structures of the central nervous system changes—the cingulate gyrus, amygdala, insula, and medial prefrontal cortex. These plastic changes in the central nervous system may also be associated with the low effectiveness of treatment aimed only at eliminating peripheral sources of chronic back pain. Currently, there is insufficient data to fully understand the pathophysiological changes underlying the development of chronic back pain. Therefore, in addition to identifying the neuropathic, nociceptive and psychogenic components in the formation of back pain, it is necessary to search for clinical and paraclinical markers of the dysfunctional component of chronic pain, on the basis of which therapeutic approaches can be optimized for this relatively therapy-resistant group of patients [56].
Impact of comorbidities
With the development of osteochondrosis, the formation of protrusions and hernias of the spine, concomitant diseases play an important role. This is, first of all, endocrine pathology: diseases of the thyroid and parathyroid glands, adrenal glands, as well as progressive diabetes mellitus. With lumbago, as a particular manifestation of osteochondrosis, it is necessary to check the condition of the kidneys. To do this, you need to perform an ultrasound of the kidneys, do a general blood and urine test.
The syndrome of chronic lumboischialgia is, as a rule, persistent. Constant pain in the lower back significantly limits the ability to work, if not completely deprives it. To prevent this from happening, treatment should begin as early as possible. Moreover, treatment measures must be comprehensive and the entire treatment process must be carried out under the supervision of a doctor.