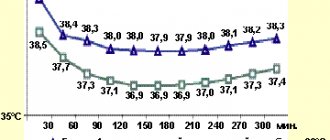
For the body to function normally, blood circulation must occur continuously. The blood supply to organs and systems is ensured by the pumping function of the heart muscle, which pushes out 70 - 80 ml of blood (cardiac output) with each systole. In a minute, in an adult with a heart rate of 70 beats, the heart pumps about 5 liters of blood (and in a day - more than 7 tons!).
- Anatomical and functional features of the cardiovascular system
- Acute cardiovascular failure
- Urgent measures
- Drug therapy
- Shock
- Collapse
Collapse as an indicator of pathological conditions in the body
Vascular collapse usually occurs as a result of a combination of exposure to various factors (pathogenic microorganisms, extremely low or high temperature, etc.) and the initial state of health. In other words, blood stops circulating normally, mainly in the presence of a serious pathology, a long-term chronic disease. The sudden development of collapse against the background of apparent complete well-being is a good reason to undergo a thorough further examination.
In the dictionary Dictionary of foreign words
{not: collapse}, a, m.
1. honey. Sudden onset of vascular insufficiency, accompanied by a drop in arterial and venous blood pressure, hypoxia, which causes a serious condition of the patient.||Cf. COMA" title='COMA, COMA is, what is COMA, COMA interpretation'>COMA I, SHOCK.
2. trans. A severe crisis in the economy and social life of the country, accompanied by a drop in production, the destruction of economic ties, and a decrease in the standard of living of the majority of the population. The country is in a state of collapse.
Share the meaning of the word:
Changes in the body that occur during collapse
When the body is exposed to pathological factors, a pathogenetic chain of adverse events develops:
- decreased vascular tone leads to their expansion and an increase in the volume of the vascular bed;
- normal or reduced (due to blood loss, burns, dehydration, etc.) volume of circulating blood as a result of decreased vascular resistance cannot provide all organs and systems with adequate blood supply, and subsequently blood redistribution occurs;
- blood is redistributed unevenly: deposited in the vessels of the abdominal cavity and lungs, it enters the skin, muscle tissue, brain and kidneys in a significantly reduced mass;
- the return of blood to the heart is significantly reduced, so the heart begins to work at a faster pace to provide the body with blood flow;
- slowing down of blood flow in the vessels as a result of deposition and insufficiently efficient work of the heart lead to blood stagnation, the formation of blood clots and even greater circulatory disorders;
- inhibition of blood supply to individual organs leads to the formation of multiple organ failure (cardiovascular, cerebral, respiratory, renal) and the appearance of clinical manifestations of collapse.
Anatomical and functional features of the cardiovascular system
From the left ventricle, blood enters the arterial system of the systemic circulation. Arteries contain 15% of the total circulating blood volume. These vessels carry blood to the tissues. The terminal sections of the arteries end in arterioles (resistance vessels). They perform the function of distributing blood in tissues. Thus, an increase in the tone of the arterioles (their spasm) prevents the flow of blood into the capillary pool. Tissue ischemia occurs, and blood flows into the venous system through arteriovenous anastomoses. A decrease in arteriolar tone, on the contrary, increases their lumen and enhances blood supply to tissues.
Natural vasoconstrictors (vasoconstrictors) are:
- adrenalin,
- norepinephrine,
- serotonin,
- angiotensin-2.
Under stress, the concentration of catecholamines (adrenaline, norepinephrine) in the blood increases sharply. They cause spasm of arterioles; a phenomenon of centralization of blood circulation occurs with a decrease in peripheral blood flow. The vasodilating effect is exerted by “acidic” metabolites (lactates, pyruvate, adenylic and inosinic acids), bradykinin, histamine, acetylcholine, a number of medications (neuroleptics, alpha-adrenolytics, peripheral vasodilators, ganglion blockers, etc.), some exogenous poisons, etc. Their action causes the phenomenon of decentralization of blood circulation (opening of the lumen of arterioles and redistribution of blood from the central vessels to the periphery, into the capillary bed).
Capillaries are an extensive network of the smallest vessels in the body, with a total length of 90,100,000 kilometers. About 20-25% of the capillaries function simultaneously, in which the transition of oxygen and nutrients from the blood to the tissues and the removal of “waste” metabolic products from them occurs. Periodically, with an interval of several tens of seconds, other capillaries open, where the blood is redistributed (vasomotion effect). Capillaries contain 12% of all circulating blood. However, in some pathological conditions this volume can increase several times.
The waste blood flows from the capillaries into the venous system. Veins play the role of a blood reservoir, since they contain the bulk of it (70%). They, unlike arteries, are able to change their volume, affecting the flow of blood to the heart.
The most important hemodynamic indicator of the venous system is central venous pressure (CVP). This is the pressure that blood exerts on the walls of the vena cava and the right atrium. It is an integral indicator of circulating blood volume, vascular tone and pumping function of the heart. CVP is measured with a phlebotonometer. Normally it is 60-120 mm of water column.
Central venous pressure decreases when:
- blood loss;
- excessive loss of water (hypohydration);
- decreased tone of arterioles and veins.
This reduces the volume of blood flowing to the heart and, accordingly, reduces cardiac output. With negative CVP values, there is a danger of circulatory arrest. Venous pressure increases when:
• heart failure (left and right ventricular);
• excessive infusion of blood and other fluids;
• obstruction of blood flow from the right ventricle of the heart (pulmonary embolism).
When the CVP is more than 150-160 mm Hg. against the background of left ventricular failure, patients may develop pulmonary edema. An integral indicator of the hemodynamics of the arterial part of the vascular system is blood pressure (systolic, diastolic, pulse and average). Systolic and diastolic blood pressure are measured with a tonometer using the Korotkoff method. Pulse blood pressure is the difference between systolic and diastolic.
The value of blood pressure is influenced by the volume of cardiac output and the resistance of peripheral vessels (arterioles). This dependence is directly proportional. Therefore, you can increase a patient’s blood pressure in the following ways:
- introduce vasoconstrictor agents (adrenaline solution, mezaton, etc.);
- increase the volume of circulating blood (by transfusion of polyglucin, refortan, etc.);
- improve the functional ability of the myocardium (by introducing cardiac glycosides, etc.).
The total blood volume in humans is about 7% of body weight: in men 70 ml/kg, in women - 65 ml/kg. The circulating blood volume (CBV) is somewhat smaller, since part of the blood does not participate in the circulation, being in the vascular depot. BCC can be measured by injecting a known concentration of a substance into the bloodstream, for example, Evans blue or polyglucin, and determining the degree of its dilution. So, measurements of central venous pressure, blood pressure, cardiac output and blood volume in patients make it possible to identify the characteristics of circulatory disorders and carry out adequate corrective therapy.
Reasons leading to the development of a collaptoid state
To date, the etiology of collapse has been well studied, which allows us to identify the main causes of its occurrence as a result of exposure to the body:
- infectious agents (causative agents of dysentery, botulism, meningoencephalitis, typhoid fever, influenza, and so on);
- massive blood loss (for example, as a result of injury, bleeding from a gastric or duodenal ulcer, from esophageal varices);
- severe burns;
- severe dehydration;
- toxins, poisons (especially cyanide, carbon monoxide, organophosphorus compounds);
- medications (most often antihypertensive, antiarrhythmic, b-blockers, as well as local anesthetics when released into the general bloodstream);
- various physical factors (too high or too low temperature, electric current, radioactive radiation):
- allergens (in case of development of an anaphylactic reaction);
- a decrease in venous tone, which leads to the development of orthostatic collapse (occurs after prolonged bed rest, a long-term serious illness, certain diseases of the endocrine system, and sometimes occurs in the postoperative period).
Almost everyone has encountered a condition (if not personally, then seen something similar in a film or read in literature) when a person who stood up quickly suddenly falls, “settles,” and becomes weaker. This is the so-called orthostatic collapse, which develops as a result of redistribution of blood flow, an increase in the vascular venous bed (due to decreased tone of the vein walls) and a significant decrease in the return of blood back to the heart.
Photo: https://pixabay.com/photos/medications-money-cure-tablets-257336/
In addition to the listed pathological factors, various acute diseases or chronic diseases in the deteriorating stage play an important role:
- cardiovascular - acute myocardial infarction, pulmonary embolism, severe heart rhythm disturbances (including pacemaker dysfunction), dissecting aortic aneurysm, artificial heart valve dysfunction, acute myocarditis, pericarditis and others;
- severe pneumonia;
- acute pancreatitis and so on.
Other factors
There is compelling evidence supporting attenuation of the baroreflex response as a mechanism responsible for ON and FCI. It is noted that heat stress may promote this response. However, several other factors have been studied that could also aggravate the reaction.
A weakening of the sensitivity of the baroreflex during hypoglycemia was found. This is important because serum glucose levels decrease with increasing exercise duration, which may increase the susceptibility of endurance and ultra-endurance athletes to CPT (36). Striving for a target time or a high pace is also associated with CF (30). When trying to achieve a final or temporary goal, the breathing rate increases, as a result, the athletes' carbon dioxide concentration decreases. Studies show a protective effect of hypercapnia (37) and the resulting hypocapnia further impairs the baroreflex (38).
Taking medications may influence the response to LBCI: taking antidepressants is a possible factor in CFN because it significantly impairs the reflex cardiovascular response to exercise by altering neurochemical reactions (39). In addition, in two independent randomized controlled clinical trials, H1 and H2 receptor antagonists blunted post-exercise hypotension, suggesting that histamine may also play a role in CEF (40, 41) (Table 4).
Table 4. Other factors
| Source | Author/journal | Year | Type of study | Patients | results | UD |
| 36 | Adler et al Diabetes | 2009 | Clinical trial | 20 men | Previous hypoglycemia impairs baroreflex sensitivity and hypotensive stress response | 2 |
| 37 | Howden et al Exp Physiol | 2004 | Case-control | 9 subjects | Increased arterial CO2 is associated with increased cerebral blood flow | 3 |
| 38 | Lucas et al J Appl Physiol | 2008 | Cross | 9 men | Postural hypotension and hypocapnia exacerbate cerebral hypoperfusion during prolonged exercise | 3 |
| 39 | Middleton et al Eur J Clin Pharmacol | 1987 | Case-control | 7 women and 7 control group | Significant impairment of the cardiovascular reflex response when taking antidepressants | 3 |
| 40 | Lockwood et al J Physiol | 2005 | Randomized controlled trial | 14 healthy men and women | H1 receptor antagonists reduce post-exercise vasodilation and blunt post-exercise hypotension | 1 |
| 41 | McCord et al J Appl Physiol | 2006 | Randomized controlled trial | 10 healthy men and women | H2 receptor antagonists reduce post-exercise vasodilation and blunt post-exercise hypotension | 1 |
| LE - level of evidence | ||||||
Classification
Conventionally, the following types of collapse can be distinguished:
- cardiogenic - develops as a result of a decrease in cardiac output (blood volume from the ventricles of the heart), which is observed, for example, with extensive myocardial infarction, heart rhythm disturbances;
- vasodilation – formed with a sharp decrease in vascular tone (vascular resistance), most often as a result of overheating of the body, an overdose of certain medications, or the course of severe infectious processes;
- hypovolemic – occurs when the volume of circulating blood decreases as a result of massive bleeding, repeated vomiting and diarrhea, deep and extensive burns;
- orthostatic.
The main reasons for the progression of the disease under study
If collapse occurs, emergency care is indicated in the following situations:
- acute bleeding, resulting in the loss of a large amount of blood,
- serious burns,
- viral diseases,
- intoxication with certain medications,
- stressful situations; depressive mood
- acute cardiovascular failure,
- diseases in the nervous system,
- endocrine pathology.
Symptoms of collapse
Collapse develops mainly suddenly and is characterized by the occurrence of typical clinical manifestations that accompany a sharp deterioration in a person’s condition. Among them, the most commonly observed are:
- severe general weakness;
- apathy, indifference to what is happening around, lethargy;
- dizziness, flashing “spots”, the appearance of a “veil” before the eyes;
- sweating, chills;
- thirst;
- significant reduction or cessation of urine output;
- rapid breathing and heartbeat, sometimes – interruptions in heart function;
- trembling of fingers, convulsions may occur.
During collapse, a sudden loss of consciousness may occur - fainting (syncope), which usually indicates suppression of blood supply to the brain.
Photo: https://pixabay.com/photos/forest-trees-sky-nature-green-1366345/
There are signs that can be used to predict an unfavorable outcome of collapse in the absence of timely assistance:
- severe headache that occurs suddenly;
- a burning sensation, heaviness behind the sternum, often spreading to the neck and lower jaw on the left, less often to the left arm;
- sharp “dagger” pain in the abdomen;
- a pronounced increase in breathing, while the person experiences suffocation;
- increased heart rate over 160 or decreased to less than 40 beats per minute;
- maintaining a significant decrease in blood pressure even after placing the patient in a horizontal position;
- the presence of known serious diseases in the victim (for example, life-threatening cardiac arrhythmias, aneurysm of the aorta or cerebral artery, chronic ischemic and non-ischemic diseases of the cardiovascular system, peptic ulcer, and so on);
- elderly age.
Symptoms
The disease occurs completely unexpectedly. Initially, weakness and dizziness occur, and the patient is thirsty. The skin becomes lighter than its normal state, profuse cold sweating appears on it, characterized by chills. The pulse becomes slower, the pressure decreases significantly, and shortness of breath is also observed. Among other things, you may notice deterioration in vision, the appearance of extraneous sounds in the ears, and the person may be worried about something. As the disease progresses, a person's thoughts become confused, his pupils dilate, and his heart beats much faster.
symptoms of collapse
First aid for collapse: a reminder for those nearby
Act quickly and confidently, without wasting time in panic; your help can save the life of the victim.
First aid for collapse includes several simple but very important points.
- It is necessary to place the person on a hard horizontal surface, while raising the lower limbs (so that the legs and the surface are about 45 degrees).
- Try to stop bleeding if it exists, as well as stop exposure to other unfavorable factors, such as high fever.
- Open the windows to provide fresh air into the room.
- Unfasten belts, buttons, fasteners while keeping clothes tightly attached to the chest and stomach.
- Let the vapor of ammonia soaked in cotton wool or gauze be inhaled through your nose (hold it near your nose for no more than a second).
- If you have a chill, cover with a warm blanket or blanket (this especially applies to the lower extremities).
- Check the patency of the upper respiratory tract: examine the oral cavity for the presence of dentures, foreign objects, food (in order to avoid suffocation due to their entry into the larynx, trachea and bronchi).
- If a person is unconscious or vomiting, experts advise turning the victim on his side, securing this position with a roll of clothing or a blanket.
- If you have a tonometer, measure your blood pressure and count your pulse per minute.
- Call an ambulance, telling in detail about the person’s condition, describing the circumstances of the development of collapse (sudden deterioration in condition, symptoms that preceded it, previously taken medications, the presence of any diseases or pathological conditions, if known).
The appearance of the patient during collapse is of great importance (when seeking medical help, he should be presented in detail to the ambulance dispatcher): pallor of the skin, sometimes with bluish lips and fingers and toes, while the skin is cold, wet and sticky to the touch, dilation of the pupils is often observed, blood pressure is reduced or not determined, the pulse is often accelerated or very rare, weak (thread-like), and frequent shallow breathing is observed.
- Prepare medications taken by the patient, as well as the patient’s epicrisis from the outpatient card/medical history, electrocardiogram, prescriptions, and so on (this way, medical workers will have a better understanding of the patient’s medical history, which will allow them to quickly determine the cause of the collapse).
- Stay with the injured person until the ambulance arrives.
You should not administer any medications or perform medical procedures on your own without the necessary education! However, this statement does not apply to a situation where there is no breathing or heartbeat: any person must have the skills of cardiopulmonary resuscitation and provide it if necessary.
Photo: https://pixabay.com/photos/ambulance-medicine-hospital-1005433/
conclusions
FCI is a common phenomenon in endurance activities, which is characterized by collapse after completion of competition without neurological, biochemical or thermal abnormalities. CFN is perhaps the most common etiology for medical providers serving competitions in the field. But the doctor needs to remember that KFN is diagnosed after excluding other etiologies that cause collapse. There is no scientific evidence to support previous assumptions that dehydration or heat stress is the cause of CFI. However, these factors, along with medications, hypocapnia and hypoglycemia, contribute to CFI. According to the modern point of view, the cause of postural hypotension is blood retention in the lower extremities due to a decrease in peripheral resistance in conditions of a weakened baroreflex response, which causes CFP. In women, KFN is predominantly not due to a violation of the baroreflex, but due to a decrease in cardiac filling. Treatment of CFP is usually symptomatic and includes oral fluid intake and the Trendelenburg position. General body cooling, intravenous hydration, or advanced treatments are not usually needed.
Rice. 1. Algorithm for collapse of physical activity.
T, temp. - temperature; SBP – systolic blood pressure; HR – heart rate, fr – saline solution.
Original
:
Diagnosis of the causes of collapse
In order to choose the right tactics for eliminating the collaptoid state, it is necessary to find out the cause of the development of the pathological condition.
For this we use:
- a thorough examination of the patient (presence of injuries, burns, active bleeding, condition of the skin, measurement of blood pressure, counting pulse and respiratory rate, assessment of heart rhythm, and so on);
- during a general examination, complaints are clarified, as well as an anamnesis of life and illness, the circumstances under which the condition worsened;
- general blood test (signs of bleeding, dehydration, infectious process, etc.);
- biochemical blood test (sugar level, kidney, liver, etc.);
- coagulogram (signs of activation or inhibition of the blood coagulation system);
- registration of an electrocardiogram (pay attention to the presence of blockades, serious heart rhythm disturbances, ischemic changes, as well as specific changes characteristic of other pathological conditions, for example, pulmonary embolism);
- according to indications, it is possible to conduct a more in-depth study: ECHO-CG, HM-ECG, EEG, FGDS, FCS, CT, MRI, X-ray and so on.
Doctors of various specialties are often invited to consultations, for example, a neurologist, cardiologist, arrhythmologist and others, if necessary.
Treatment
According to scientific data, blood retention in the lower extremities with a weakening of the baroreflex response are the main mechanisms of CFN. Therefore, the choice of treatment options is primarily aimed at correcting these disorders. Because there is insufficient evidence for hyperthermia and dehydration as the primary etiology of CFN, general body cooling and intravenous fluid administration are not considered as the initial treatment of CFN.
A randomized controlled trial demonstrated restoration of normal hemodynamics by the Trendelenburg position (42, 43). Oral fluid intake has also been shown to protect against CFP and has been used as an effective treatment for CFP (43, 44). A randomized controlled trial and two small studies found a redirection of peripheral blood flow to the center and a reduction in cardiovascular tension from superficial skin cooling, suggesting that cooling may treat CFI (45 – 47). Finally, according to a study of compression stockings in runners, if runners are prone to ON, they may benefit from wearing compression stockings while running (48). People prone to FCI also appear to benefit from taking medications that block the H1 and H2 receptors, cooling the skin surface, and ensuring adequate glucose intake during exercise (Table 5).
Table 5. Treatment
| Source | Author/magazine | Year | Type of research | Patients | Result | UD |
| 42 | Journeay et al Aviat Space Environ Med | 2004 | Randomized controlled trial | 6 subjects | Positive pressure in the lower body helps restore hemodynamics | 1 |
| 43 | Anley et al Br J Sports Med | 2010 | Randomized controlled trial | 28 athletes | PHFN is effectively treated with Trendelenburg position and oral hydration | 1 |
| 44 | Davis and Fortney Int J Sports Med | 1997 | Controlled test | 5 men | Fluid intake is an effective treatment for ON | 2 |
| 45 | Durand et al Am J Physiol Regul Integr Comp Physiol | 2004 | Randomized controlled trial | 8 subjects | Superficial cooling of the skin – improves OH in people with normal temperature | 1 |
| 46 | Wilson et al J Appl Physiol | 2002 | Clinical trial | 9 subjects | Superficial cooling of the skin protects people under heat stress from OH | 3 |
| 47 | Cui et al Am J Physiol Heart Circ Physiol | 2005 | Controlled test | 9 subjects | Superficial cooling of the skin increases central venous pressure | 2 |
| 48 | Privett et al Clin J Sport Med | 2010 | Controlled test | 6 subjects | Runners who are prone to OH after exercise can reduce their risk by wearing compression stockings while running. | 1 |
| PPHH – postural exercise hypotension; OH – orthostatic intolerance. | ||||||
Therapeutic measures
The reason for the development of collapse is determined by the algorithm for providing assistance:
- when exposed to poisons, toxins, drugs - remove substances from the body as quickly and completely as possible, use specific antidotes;
- stopping bleeding, replenishing blood loss with blood components or blood substitutes;
- stopping the use of the drug that caused anaphylactic shock, anti-shock measures (infusion therapy, antihistamines, adrenergic agonists, glucocorticosteroids, etc.);
- the use of antiarrhythmic drugs, electrical pulse therapy, temporary or implantable pacemakers for cardiac arrhythmias;
- the use of cardiotropic treatment for acute myocardial infarction, myocarditis, pericarditis, cardiomyopathies and other diseases of the cardiovascular system;
- the use of antiviral and/or antibacterial drugs in the presence of an infectious process, and so on (depending on the etiological factor).
Photo: https://pixabay.com/photos/medicine-pills-blood-pressure-2994788/
Emergency care for collapse of almost any etiology includes the use of:
- inhalation of humidified oxygen;
- infusion therapy;
- glucocorticosteroids;
- vasopressor drugs.
These measures are used after performing the first aid described above. The patient is usually hospitalized in the intensive care unit (or in a specialized hospital), where treatment and monitoring of hemodynamic parameters continue.
The danger of a collapsed state
When collapse develops, it is important to remember that the further prognosis depends on how quickly the correct emergency care is provided. You need to understand that minutes of delay can cost the victim his life. In the absence of adequate medical care, collapse quickly leads to multiple organ failure and disruption of the normal functioning of internal organs.
The greatest danger is the developing disruption of the blood supply to the brain, which can lead to ischemia and massive death of nerve cells.