Type 2 diabetes is a chronic disease that makes a person dependent on diets and medications for life. At the same time, by detecting the disease in time and being monitored by a good endocrinologist, a diabetic patient can maintain a good quality of life without severe attacks and complications.
Why does type 2 diabetes occur: scientists have discovered the cause of the pathological condition
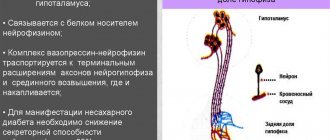
The culprit of the disorder is the hormone adiponectin (GBP-28), produced by adipocytes - cells of adipose tissue of internal organs. The main function of adiponectin is the breakdown of fat deposits into amino acids. It is this process that prevents obesity. In addition, the hormone prevents the formation of atherosclerotic plaques, normalizes cholesterol, and reduces the likelihood of blood clots.
There is a direct relationship between the amount of adiponectin produced and body mass index. The slimmer a person is, the more of this hormone his body produces. And vice versa: high body weight is directly related to a decrease in the amount of GBP-28.
The hormone was discovered only in 1994; until that time, the mechanism of type 2 diabetes was not studied and, accordingly, could not be treated correctly, so the diagnosis of type 2 diabetes was equal to a life sentence. Recent studies have shown that adiponectin directly affects glucose metabolism, influencing the development of diabetes. This discovery provides a new way to treat non-insulin-dependent diabetes.
Adiponectin affects many vital processes, which explains a large number of complications in diabetics who have low levels of the hormone. In particular, GBP-28:
- prevents the formation of fatty deposits in the liver;
- maintains optimal lumen and elasticity of blood vessels;
- prevents visceral fat from depositing on the surface of internal organs;
- helps diagnose atherosclerosis, because hormone cells are deposited in vascular microtraumas;
- increases metabolism and promotes weight loss;
- reduces inflammation of blood vessels and arteries;
- protects the myocardium from necrosis in case of lack of oxygen.
When the level of this hormone decreases, a person becomes ill, and a complex of processes in his body is disrupted.
The relationship between obesity and type 2 diabetes
The culprit of type 2 diabetes in most cases is visceral fat. This is not exactly the fat that is deposited on the sides and waist when you gain excess weight. The reason for the appearance of visceral fat is a discrepancy between the energy entering the body with food and the energy being wasted.
High-calorie, fatty and carbohydrate foods have high energy reserves, so a passion for flour and confectionery products, fried potatoes and pasta with meat gravy is fraught with excess weight. Excess unspent energy goes into the body's fat reserves, namely, into the subcutaneous fat layer and visceral fat.
- Subcutaneous fat has a unique structure. It is distributed on the hips, waist, abdominal wall, and legs in women. Making the figure more rounded, but within reasonable limits, such “replenishment” does not pose a great danger to health. This fat, with normal metabolism and diet, goes away as easily as it comes.
- The visceral (abdominal) type of fat deposits is incredibly dangerous from a medical point of view. The body needs it in small quantities, because... protects internal organs from mechanical damage, and also serves as a reserve depot in case of energy depletion. But its excess is already a disaster for the body.
Abdominal fat accumulates under the serosa, a thin connective membrane that surrounds each organ. In most cases, abdominal fat is located on the surface of the abdominal organs, so a characteristic feature of the problem is a protruding abdomen, disproportionately large compared to other parts of the body. Normally, the amount of such fat should not exceed 15% of the total mass of body fat. If there is much more of it, the excess enters the liver through the bloodstream, being processed into cholesterol. There is a threat of developing atherosclerosis, which leads to stroke or heart attack.
Abdominal fat reduces the amount of adiponectin secreted, and it directly affects the sensitivity of cells to insulin. As a result, a person develops insulin resistance and develops type 2 diabetes.
Yeast infections and gangrene
Diabetes weakens the immune system and a person becomes susceptible to all sorts of fungal diseases. Fungus and other microbes feed on glucose; this is a favorable environment for them to live and reproduce.
High sugar levels not only provoke inflammation in open wounds, but also interfere with rapid healing. Due to poor circulation, it is difficult for blood to reach the affected areas of the body and repair the damage. In addition, diabetes provokes the creation of a bacterial environment and rot, which can result in gangrene. The peripheral parts of the body are affected first, i.e. legs. Gangrene begins first with tingling and numbness in the big toe, and then spreads throughout the leg. The rotting of a living organism is one of the most unpleasant and terrible sensations. A person experiences it in two cases: with gangrene and cancer. In the end, in despair, the patient, exhausted by pain, decides to amputate the limb.
Naturally, maintaining a daily diet is an expensive and burdensome pleasure. In addition to the fact that a person must eat “tasteless” food, he must also carefully select and dose it, and this for the rest of his life. As a result, most people suffering from diabetes have a breakdown within the first year after the diagnosis is announced. Firstly, this is a huge shock for the patient, and secondly, the understanding that this disease is incurable and the medicine must be taken on an ongoing basis can cause denial of the disease itself.
How is type 2 diabetes different from type 1 diabetes?
Despite the similarity of names and some symptoms, type 1 and type 2 diabetes have different natures and forms of progression.
| Type 1 diabetes | Type 2 diabetes |
| Most often diagnosed before the age of 20 | Common among people over 40 years of age |
| Sugar rises sharply | Slow progression of the disease |
| The patient loses weight sharply | The patient is noticeably overweight |
| Appears regardless of the patient’s lifestyle | Lifestyle plays a big role in the development of the disease. |
| The disease manifests itself quickly and violently | There are no symptoms for a long time |
| Insulin is significantly below normal | Insulin is slightly higher than normal |
| Sugar-lowering drugs are ineffective | Sugar substitutes help |
| The disease is incurable | If you follow the diet, there are tendencies to cure |
| Without insulin therapy a person dies | Insulin injections are not needed |
Symptoms of the disease
Unlike type 1 diabetes, T2DM can be asymptomatic for a long time. Patients may present nonspecific complaints of weakness and fatigue. In this regard, the disease can be detected accidentally during examination for:
- fungal skin infections;
- slow healing of skin wounds;
- leg pain;
- erectile dysfunction.
In 20-30% of cases, T2DM is diagnosed in people with myocardial infarction, stroke, decreased vision due to retinal damage and other complications of diabetes. [1]
You can suspect carbohydrate metabolism disorders based on the following symptoms:
- thirst, increasing the amount of fluid consumed to 3-5 liters per day;
- itching of the skin and mucous membranes;
- an increase in the amount of daily urine, including at night;
- causeless loss of body weight. [1]
The absence of these symptoms is not a reason to refuse an annual preventive examination.
Type 2 diabetes in children
Type 2 diabetes is more common in adults, but young children are also susceptible to the disease. These are mainly kids whose parents did not monitor their diet and allowed them to eat chips, candies and other sweets with dyes and a lot of sugar.
However, type 1 diabetes, which has a high hereditary factor, is most common in childhood. But recently, doctors have noted a sharp increase in the incidence of type 2. If in the 80-90s of the 20th century type 2 diabetes occurred in only 2% of children, today it is diagnosed in almost 45% of diabetic children. Moreover, 85% of them are overweight.
The following factors lead to the development of the disease in children:
- viral infections suffered by the mother during pregnancy;
- stress in the baby, which provokes the release of adrenaline into the blood, disrupting carbohydrate processes;
- the child’s passion for foods rich in sugar (waffles, candies, condensed milk, soda);
- lack of movement, physical inactivity;
- birth weight above 4000 grams.
Causes of the disease
The hereditary factor is of primary importance in the development of diabetes mellitus. Predisposition to the disease is transmitted through the maternal line in 5% of cases and through the father in 10% of cases. If both parents have diabetes, the risk of developing pathology reaches 100%.
Also, the main causes of non-insulin-dependent diabetes include:
- inactivity and overeating, leading to obesity - if body weight is 50% higher than normal, then the risk of increased glucose increases to 60%;
- poor nutrition.
The main causes of insulin-dependent diabetes:
- autoimmune diseases (lupus, autoimmune thyroiditis, glomerulonephritis, hepatitis);
- viral infections that destroy pancreatic beta cells responsible for the production of insulin (chickenpox, rubella, hepatitis, mumps).
Does diabetes really come from sweets?
You should not compare the sweets of your childhood with modern sweets. They are much more high in calories and harmful. In their production, trans fats, preservatives, and dyes are used, and this is an additional burden on the pancreas.
Children's passion for computer games leads to physical inactivity and, as a result, an increase in the amount of visceral fat. And it is precisely the main culprit in the development of type 2 diabetes. Therefore, doctors are no longer surprised that children of primary school age suffer from such an “adult” disease.
Risk group for type 2 diabetes mellitus
According to scientists, type 2 diabetes will be 5 times more common by the middle of the 21st century than in the 2000s. This is due to the deterioration of the environment, the popularization of fast food, physical inactivity, and also due to the fact that a generation whose childhood was spent glued to the computer will become adults. In other words, all modern youth who ignore healthy eating and sports are at risk.
The risk group also includes:
People over 40 years of age.
Although each person has his own bodily characteristics, generally the threshold for the development of clear signs of diabetes is 40 years of age.
- Women.
After forty, women preparing for menopause produce less and less sex hormones that support metabolic processes every year. - Men.
At the age of 40, male menopause begins, which for some reason many men have never even heard of. At this age, the male body also reduces hormonal activity.
With the onset of menopause, even those who have remained slim all their lives begin to gain weight. That's why after 40 years you should significantly reduce the number of calories you consume and start watching your weight.
People with a high body mass index (BMI).
This is the indicator recommended by the World Health Organization for calculating the degree of correspondence between height and weight of a person. The criteria are very arbitrary, because they do not take into account the age and occupation of a person. However, they should be followed to understand when to stop and start losing weight.
- On average, the formula is: (height [cm] - 100) ± 10%. Those. with a height of 162 cm, a woman should normally weigh no more than 68 kg in order not to have health problems.
- Waist circumference also matters. For men, the maximum figure is 102 cm, for women - 88 cm. If the waist size is much higher, this indicates an excess of visceral fat, which is deposited on the organs.
Excess weight leads to inhibition of the production of adiponectin, which is responsible for converting insulin into energy and delivering it into the cell;
Hypodynamia - lack of movement
. Sports and exercise increase muscle demand for glucose. Without movement, excess glucose remains in the blood, which leads to decreased sensitivity to insulin. This is how diabetes develops.
Eating disorder - constant consumption of “fast” carbohydrates.
Fast food, candy bars, restaurant food, McDonald's treats, chips and sodas contain high amounts of readily available carbohydrates and starch with little or no fiber. Carbohydrates quickly enter the bloodstream, forcing the production of more insulin. If you do this often, insulin resistance develops.
Frequent stress.
During stress, the body releases a large amount of adrenaline, an insulin antagonist hormone. Accordingly, the more adrenaline in the blood, the higher the glucose level. Blood sugar levels rise, but cells cannot get energy from it. Excess glucose is excreted through the kidneys, which negatively affects their function. This is how type 2 diabetes begins, which a person could have prevented.
Acute complications of diabetes mellitus in the practice of an emergency physician
Acute complications of diabetes mellitus are life-threatening conditions caused by significant changes in blood sugar levels and associated metabolic disorders.
Acute complications of diabetes mellitus:
- hyperglycemic comas - ketoacidotic, hyperosmolar;
- hypoglycemic coma.
Diabetic ketoacidosis and non-ketonic hyperosmolar coma are characterized by varying degrees of insulin deficiency, excess production of counter-insulin hormones and dehydration. In some cases, signs of diabetic ketoacidosis and hyperosmolar coma may develop simultaneously.
Hypoglycemia is caused by an imbalance between the medicine used to treat diabetes (insulin or blood glucose-lowering tablets) and food intake or exercise.
The speed and timeliness of providing care to comatose patients largely determine the prognosis. Therefore, proper management of patients at the prehospital stage is very important.
In the structure of comas at the prehospital stage, hypoglycemic coma ranks third (5.4%), and diabetic coma (3%) ranks fifth (data from the NNPOSMP).
Diabetic ketoacidotic coma (DKA)
DKA is a very serious complication of diabetes mellitus, characterized by metabolic acidosis (pH less than 7.35 or bicarbonate concentration less than 15 mmol/L), increased anion gap, hyperglycemia above 14 mmol/L, and ketonemia. More often develops in type 1 diabetes. DKA accounts for 5 to 20 cases per 1000 patients per year (2/100). The mortality rate is 5-15%, for patients over 60 years old - 20%. More than 16% of patients with type 1 diabetes die from ketoacidotic coma. The cause of the development of DKA is an absolute or pronounced relative deficiency of insulin due to inadequate insulin therapy or an increased need for insulin.
Provoking factors: insufficient dose of insulin or skipping an insulin injection (or taking tableted glucose-lowering drugs), unauthorized cancellation of glucose-lowering therapy, violation of insulin administration technique, addition of other diseases (infections, trauma, surgery, pregnancy, myocardial infarction, stroke, stress, etc.) , dietary disorders (too many carbohydrates), physical activity with high glycemia, alcohol abuse, insufficient self-monitoring of metabolism, taking certain medications (corticosteroids, calcitonin, saluretics, acetazolamide, β-blockers, diltiazem, isoniazid, diphenin, etc. ).
Often the etiology of DKA remains unknown. It should be remembered that in approximately 25% of cases, DKA occurs in patients with newly diagnosed diabetes mellitus.
There are three stages of diabetic ketoacidosis: moderate ketoacidosis, precoma, or decompensated ketoacidosis, coma.
Complications of ketoacidotic coma include deep vein thrombosis, pulmonary embolism, arterial thrombosis (myocardial infarction, cerebral infarction, necrosis), aspiration pneumonia, cerebral edema, pulmonary edema, infections, rarely - gastrointestinal tract and ischemic colitis, erosive gastritis, late hypoglycemia. Severe respiratory failure, oliguria and renal failure are noted. Complications of therapy include cerebral and pulmonary edema, hypoglycemia, hypokalemia, hyponatremia, hypophosphatemia.
Diagnostic criteria for DKA
- The peculiarity of DKA is its gradual development, usually over several days.
- The presence of symptoms of ketoacidosis (the smell of acetone in the exhaled air, Kussmaul breathing, nausea, vomiting, anorexia, abdominal pain).
- The presence of symptoms of dehydration (decreased tissue turgor, tone of the eyeballs, muscle tone, tendon reflexes, body temperature and blood pressure).
When diagnosing DKA at the prehospital stage, it is necessary to find out whether the patient suffers from diabetes mellitus, whether there is a history of DKA, whether the patient is receiving glucose-lowering therapy, and if so, what kind, when was the last drug taken, the time of the last meal, whether excessive physical activity or alcohol intake, what recent diseases preceded the coma, whether there was polyuria, polydipsia and weakness.
Prehospital treatment of DKA (see Table 1) requires special attention to avoid errors.
Possible errors in therapy and diagnosis at the prehospital stage
- Prehospital insulin therapy without glycemic control.
- The emphasis in treatment is on intensive insulin therapy in the absence of effective rehydration.
- Insufficient volume of fluids administered.
- Administration of hypotonic solutions, especially at the beginning of treatment.
- Use of forced diuresis instead of rehydration. The use of diuretics simultaneously with the administration of fluids will only slow down the restoration of water balance, and in hyperosmolar coma, the use of diuretics is strictly contraindicated.
- Initiating therapy with sodium bicarbonate may be fatal. It has been proven that adequate insulin therapy in most cases helps eliminate acidosis. Correction of acidosis with sodium bicarbonate carries an exceptionally high risk of complications. The introduction of alkalis increases hypokalemia and disrupts the dissociation of oxyhemoglobin; carbon dioxide formed when sodium bicarbonate is administered increases intracellular acidosis (although the blood pH may increase); paradoxical acidosis is also observed in the cerebrospinal fluid, which can contribute to cerebral edema; the development of “rebound” alkalosis cannot be ruled out. Rapid administration of sodium bicarbonate (boost) can cause death due to the rapid development of hypokalemia.
- Administration of sodium bicarbonate solution without additional administration of potassium preparations.
- Withholding or not prescribing insulin for DKA in a patient who is unable to eat.
- Intravenous bolus injection of insulin. Only during the first 15-20 minutes is its concentration in the blood maintained at a sufficient level, so this route of administration is ineffective.
- Three to four times of subcutaneous short-acting insulin (RAI). ICD is effective for 4-5 hours, especially in conditions of ketoacidosis, so it should be prescribed at least five to six times a day without an overnight break.
- The use of sympathotonic drugs to combat collapse, which, firstly, are counter-insulin hormones, and, secondly, in diabetic patients their stimulating effect on glucagon secretion is much more pronounced than in healthy individuals.
- Incorrect diagnosis of DKA. With DKA, the so-called “diabetic pseudoperitonitis” often occurs, which simulates the symptoms of an “acute abdomen” - tension and pain in the abdominal wall, a decrease or disappearance of peristaltic noises, and sometimes an increase in serum amylase. Simultaneous detection of leukocytosis can lead to an error in diagnosis, as a result of which the patient ends up in the infectious (“intestinal infection”) or surgical (“acute abdomen”) department. In all cases of “acute abdomen” or dyspeptic symptoms in a patient with diabetes, it is necessary to determine glycemia and ketotonuria.
- Failure to measure glycemia in any patient who is unconscious, which often leads to erroneous diagnoses - “cerebrovascular accident”, “coma of unknown etiology”, while the patient has acute diabetic metabolic decompensation.
Hyperosmolar nonketoacidotic coma
Hyperosmolar non-ketoacidotic coma is characterized by severe dehydration, significant hyperglycemia (often above 33 mmol/l), hyperosmolarity (more than 340 mOsm/l), hypernatremia above 150 mmol/l, absence of ketoacidosis (maximum ketonuria (+)). It develops more often in elderly patients with type 2 diabetes. It is 10 times less common than DKA. Characterized by a higher mortality rate (15-60%). The reasons for the development of hyperosmolar coma are a relative deficiency of insulin and factors that provoke the occurrence of dehydration.
Provoking factors: insufficient dose of insulin or skipping an insulin injection (or taking tableted glucose-lowering drugs), unauthorized cancellation of glucose-lowering therapy, violation of insulin administration technique, addition of other diseases (infections, acute pancreatitis, trauma, surgery, pregnancy, myocardial infarction, stroke, stress and etc.), dietary disorders (too many carbohydrates), taking certain medications (diuretics, corticosteroids, beta blockers, etc.), cooling, inability to quench thirst, burns, vomiting or diarrhea, hemodialysis or peritoneal dialysis.
It should be remembered that a third of patients with hyperosmolar coma do not have a previous diagnosis of diabetes mellitus.
Clinical picture
Severe thirst, polyuria, severe dehydration, arterial hypotension, tachycardia, focal or generalized convulsions increasing over several days or weeks. If, with DKA, disorders of the central nervous system and peripheral nervous system occur according to the type of gradual loss of consciousness and inhibition of tendon reflexes, then hyperosmolar coma is accompanied by a variety of mental and neurological disorders. In addition to the soporous state, which is also often observed in hyperosmolar coma, mental disorders often occur as delirium, acute hallucinatory psychosis, and catotonic syndrome. Neurological disorders are manifested by focal neurological symptoms (aphasia, hemiparesis, tetraparesis, polymorphic sensory disorders, pathological tendon reflexes, etc.).
Diagnostic criteria
- Hyperosmolar non-ketoacidotic coma develops more slowly (within 5-14 days) than DKA. Dehydration is more pronounced (decreased tissue turgor, tone of the eyeballs, muscle tone, tendon reflexes, body temperature and blood pressure) with neurological symptoms, there is no ketoacidosis, ketonuria, anuria and azotemia occur more often in elderly and senile age.
Among possible errors in therapy (see Table 2) and diagnosis, it is customary to highlight the administration of hypotonic solutions at the prehospital stage, long-term administration of hypotonic solutions.
Hypoglycemic coma
Hypoglycemic coma develops due to a sharp decrease in blood glucose levels (below 3-3.5 mmol/l) and severe energy deficiency in the brain.
Provoking factors: overdose of insulin and TCC, skipping or inadequate meals, increased physical activity, excessive alcohol intake, taking medications (β-blockers, salicylates, sulfonamides, etc.).
Clinical picture
Symptoms of hypoglycemia are divided into early (cold sweat, especially on the forehead, pale skin, severe paroxysmal hunger, trembling hands, irritability, weakness, headache, dizziness, numbness of lips), intermediate (inappropriate behavior, aggressiveness, palpitations, poor coordination of movements, double vision, confusion) and late (loss of consciousness, convulsions).
Diagnostic criteria
- Sudden onset of symptoms, usually over a period of several minutes, less often hours.
- The presence of characteristic symptoms of hypoglycemia.
- Glycemia is below 3-3.5 mmol/l.
At the prehospital stage, it is necessary to find out: how long the patient has been suffering from diabetes mellitus, whether the patient receives hypoglycemic therapy, and if so, what kind, when was the last drug taken, whether there have been any dietary violations, whether there have been any episodes of hypoglycemia in the past, whether excessive physical activity and alcohol intoxication were allowed.
Therapy for hypoglycemic coma at the prehospital stage (see Table 3) includes the use of thiamine, prednisolone, glucose, adrenaline solution, magnesium sulfate.
After removing the patient from a hypoglycemic coma, it is recommended to use drugs that improve microcirculation and metabolism in brain cells (glutamic acid, aminolon, stugeron, cavinton) for three to six weeks.
Repeated hypoglycemia can lead to brain damage.
Possible diagnostic and therapeutic errors
- An attempt to introduce carbohydrate-containing products (sugar, etc.) into the oral cavity of an unconscious patient. This often leads to aspiration and asphyxia.
- Use of unsuitable foods (bread, chocolate, etc.) to relieve hypoglycemia. These foods do not have a sufficient sugar-raising effect or raise blood sugar levels too slowly.
- Incorrect diagnosis of hypoglycemia. Some symptoms of hypoglycemia may be mistakenly regarded as an epileptic seizure, stroke, “vegetative crisis,” etc. In a patient receiving hypoglycemic therapy, if there is a reasonable suspicion of hypoglycemia, its relief should begin immediately, even before receiving a response from the laboratory.
- Once a patient has been brought out of severe hypoglycemia, the risk of relapse is often not taken into account.
In patients in a comatose state of unknown origin, it is always necessary to assume the presence of glycemia. If it is reliably known that the patient has diabetes mellitus and at the same time it is difficult to differentiate the hypo- or hyperglycemic genesis of the coma, intravenous jet administration of glucose is recommended in a dose of 20–40–60 ml of 40% solution for the purpose of differential diagnosis and emergency assistance for hypoglycemic coma In the case of hypoglycemia, this significantly reduces the severity of symptoms and thus allows differentiation between the two conditions. In hyperglycemic coma, such an amount of glucose will have virtually no effect on the patient’s condition.
In all cases where it is not possible to measure blood glucose immediately, highly concentrated glucose should be administered empirically. If hypoglycemia is not treated urgently, it can be fatal.
The basic drugs for patients in a coma, in the absence of the possibility of clarifying the diagnosis and immediate hospitalization, are considered to be thiamine 100 mg IV, glucose 40% 60 ml and naloxone 0.4-2 mg IV. The effectiveness and safety of this combination have been repeatedly confirmed in practice.
Kh. M. Torshkhoeva, Candidate of Medical Sciences A. L. Vertkin, Doctor of Medical Sciences, Professor V. V. Gorodetsky, Candidate of Medical Sciences, Associate Professor of NNPO Emergency Medical Care, MGMSU
Symptoms of type 2 diabetes
The signs of this pathology may appear blurred and unexpressed for a long time, which often leads to late detection of the disease. The following symptoms should be warning signs for the patient:
- severe thirst and dry mouth;
- excessive urination, forcing the patient to frequently visit the toilet;
- weight loss;
- visual impairment;
- irritability, increased fatigue, weakness;
- sleep disorders;
- weakening of potency and sexual libido in men;
- digestive disorders - nausea, vomiting, stool disorders.
In the absence of a timely response to symptoms and adequate treatment, the patient lives for a long time with elevated blood sugar levels. This leads to high stress on all internal organs, including the liver, kidneys, heart and blood vessels .
As a result, dangerous consequences such as heart attack, stroke, kidney or liver failure may develop. Due to the fact that tissue healing processes in the body are sharply disrupted, there is a high risk of developing diabetic foot, which can result in limb amputation.
Serious complications.
The development of type 2 diabetes mellitus may be accompanied by the development of chronic and acute complications. The most dangerous complications can lead to death - hyperglycemic coma, hypoglycemic coma, lactic acid coma. Chronic complications develop gradually and include diabetic microangiopathies and macroangiopathies - manifested by thrombosis and vascular atherosclerosis. Disturbances in the functioning of internal organs, joint pain and mental disorders (depression, emotional instability) are often noticeable.
How type 2 diabetes is detected: diagnosis
The difficulty with identifying type 2 diabetes is that the disease may not manifest itself for years. However, the sooner the problem is identified, the more chances the patient has for a full recovery.
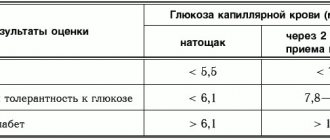
- Blood sugar test.
The simplest test is taking blood for sugar. It is done on an empty stomach, and the patient takes blood from his finger. The normal level is considered to be a glucose concentration of 3.3 to 5.5 mmol/l. Anything higher, even a couple of tenths, is already a cause for concern. However, such an analysis does not give the complete picture. It is quite possible that the patient had gone to a birthday party the day before, and tests showed the consequences of the feast. It is advisable not to indulge in confectionery the day before donating blood. - Glycemic hemoglobin analysis.
A much more telling indicator is glycemic hemoglobin. It detects the disease at the initial stage of development, and also identifies people who are predisposed to diabetes. The analysis is based on the fact that red blood cells, consisting of hemoglobin, “live” in the body for about 120 days, and then break down in the spleen to bilirubin. During this period, they deliver oxygen to the cells and remove carbon dioxide.
Analysis for glycated hemoglobin shows the process of carbohydrate metabolism. If the percentage of glycemic hemoglobin is higher than normal, but the blood glucose test remains normal, this indicates the initial stage of diabetes or prediabetes.
Endocrinologists at the Diana Medical Center urge all patients over 40 years of age to regularly undergo a comprehensive examination of the body and carefully monitor blood glucose levels. This will allow you to detect signs of diabetes in time and avoid serious complications.
Information about the disease.
In fact, “diabetes mellitus” from Greek means loss of sugar. Thus, the term reflects the main symptom of the disease (lack of sugar) - glucose is not retained in the body and is excreted in the urine. Type 2 diabetes mellitus (non-insulin-dependent) develops against the background of tissue insensitivity to the action of insulin, as well as a subsequent decrease in cell function. Diabetes mellitus type 2 (DM2) is different from diabetes mellitus type 1 (DM1). In diabetes 1, the lack of insulin is primary; in diabetes 2, the lack of the hormone is a consequence of a prolonged lack of insulin. Statistics are very diverse and depend on ethnic characteristics and living standards. In Russia, the prevalence is about 7%, and covers 90% of all forms of diabetes. The group most susceptible to the disease is people over 40-45 years of age.
Blood sugar levels: norms and violations
| Analysis | Men | Women | ||
| norm | pathology | norm | pathology | |
| Glycated hemoglobin % (up to 30 years) | 4,5-5,5 | over 5.5 | 4-5 | over 5 |
| Glycated hemoglobin % (from 30 to 50 years) | 5,5-6,5 | over 6.5 | 5-7 | over 7 |
| Blood from a finger on an empty stomach, mmol/l | 3,3–5,5 | over 5.5 | 3,3–5,5 | over 5.5 |
| Analysis after taking 75 grams of glucose, mmol/l | less than 7.8 | over 7.8 | less than 7.8 | over 7.8 |
| Analysis for adiponectin, mg/ml | more than 10 | less than 10 | more than 10 | less than 10 |
How is type 2 diabetes treated?
The first thing a patient is prescribed after diabetes is diagnosed is a strict diet. Daily calorie intake should not exceed 2000. At the same time, such a concept as XE (bread units) is introduced.
1 XE is 25 grams of bread or 12 grams of digested carbohydrates. A person with type 2 diabetes should consume no more than 20 XE per day. With obesity, the norm decreases to 10 XB, and with heavy physical work it increases to 25 XB.
The patient distributes carbohydrate-rich foods evenly throughout the day. Products containing large amounts of XE include honey, dried apricots, white and black bread, cereals, pasta, and sweets. Accordingly, these products should be consumed sparingly.
Fish, meat and eggs do not contain XE at all. There is little XE in vegetables, fruits and herbs. Based on this, the diet of a patient with type 2 diabetes should consist of meat and fish dishes, as well as salads and fruit slices.
If diabetes is at an advanced stage, the patient is prescribed medications.
- glitazones (Roglit, Avandia) accelerate the process of removing glucose from cells;
- biguanides (Langerin, Siofor) increase the sensitivity of cells to glucose;
- sulfonylurea derivatives (Glidiab, Glucobene) stimulate the production of insulin by the pancreas;
- SGLT2 protein inhibitor (Invokana, Jardins) remove excess glucose from the body).
All of these drugs have serious side effects. Their effectiveness also decreases over time. Over time, with progressive diabetes, the patient is prescribed insulin injections, and diabetes from type 2 develops into incurable type 1. That is why it is so important to recognize the disease in time in order to begin treatment and stop the progression of the disease.
Where to get tested for diabetes in St. Petersburg
You can get tested for type 2 diabetes at the Diana Clinic in St. Petersburg. Here you can also undergo an ultrasound of the pancreas using a new expert device. After this, you can consult an experienced endocrinologist.
Endocrinologists at the Diana Clinic take a comprehensive approach to the treatment of non-insulin-dependent diabetes mellitus, combining proper nutrition, giving up bad habits and physical activity with rationally selected medications.
Make an appointment with a gynecologist by calling 8-800-707-1560, request a call back or fill out the appointment form on the page!
Treatment methods
Currently, there is no way to eliminate the cause of the disease and completely cure diabetes mellitus. Therefore, diabetics are prescribed symptomatic treatment aimed at getting rid of unpleasant symptoms, maintaining stable glucose levels, normalizing body weight and preventing complications.
For type 1 diabetes mellitus, insulin therapy is prescribed, and for type 2 diabetes, sugar-lowering drugs are prescribed. Moderate physical activity and proper diet are important for successful treatment.