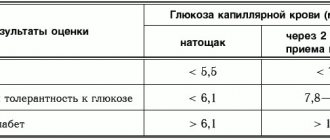
Symptoms of high blood sugar can appear at any age. You need to know them in order to go to the hospital in time so that the doctor can prescribe treatment. The normal blood sugar level depends on the age of the person: in infants up to one year old it varies from 2.8 to 4.4 mmol/l, in people older than this age it ranges from 3.3 to 5.5 mmol/l.
When they are higher than these values, they speak of hyperglycemia. It can be caused by various pathological processes in the body; as a rule, elevated blood sugar levels are associated with a disorder of carbohydrate metabolism.
Therefore, it is important to replace the signs of hyperglycemia in time in order to consult a doctor in a timely manner. You also need to know the reasons that can trigger an increase in blood glucose in order to eliminate them if possible.
Diabetes mellitus in women: main signs and symptoms
In most cases, the causes of diabetes in women are the same as in men, but its occurrence and manifestation have a number of differences due to the physiological characteristics of the female body. The disease occurs due to disruptions in the functioning of the endocrine system, which becomes more vulnerable during periods of childbirth, menopause and the postmenopausal stage of life 1.
Plus, the female body is more prone to obesity, which predisposes to metabolic problems and hormonal disorders that affect blood glucose levels. There are two types of diabetes mellitus – the first (DM1) and the second (DM2)1.
Symptoms
The characteristic symptoms of hyperglycemia do not appear immediately. Due to the blurred clinical picture, it is not always possible to suspect a pathology and begin therapy on time. You should go to the hospital to get tested if the following signs appear:
- Intense thirst. This is one of the main symptoms of high blood sugar. Glucose draws water from peripheral tissues and the person feels thirsty all the time. When sugar reaches 10 mmol, it begins to be excreted in the urine, and with it water, which causes frequent emptying of the bladder and dehydration.
- Dry mouth.
- Headaches caused by water-salt imbalance and dehydration.
- Skin itching.
- Weakened vision.
- Numbness and tingling of the fingers of the upper and lower extremities.
- Pain when walking.
- Hands and feet are cold to the touch. This is due to the fact that peripheral blood circulation is impaired.
- Nephropathy.
- Weight gain or loss that is associated with insulin dysfunction.
- Disturbances in the functioning of the digestive tract, which causes stool retention or indigestion.
- Decreased appetite.
- Smell of acetone from the mouth.
- Poor skin regeneration; with hyperglycemia, even small wounds take a long time to heal.
- Heart rhythm disturbances;
- Heavy, restless breathing;
- Fast fatiguability;
- Weakening of the immune system, which causes a person to often get sick.
With severe hyperglycemia, severe dehydration and ketoacidosis develop, and consciousness is impaired. It can cause coma.
The symptoms of high blood sugar in men and women are largely similar, but the latter are more likely to experience:
Pathology of diabetes mellitus type 1 and 2
In T1DM, the body stops producing or significantly reduces the production of the insulin gene due to the death of pancreatic beta cells. This happens because the immune system malfunctions and, instead of foreign microbes and bacteria, mistakenly begins to destroy the cells and structures of its own body.
This is called an autoimmune pathological process, the trigger for which can be:
- genetic predisposition;
- viral infections;
- some chemicals1.
In T2DM, insulin-dependent tissues of the body - fat, muscle and liver - cease to provide an adequate metabolic response to the insulin gene. The receptors interact poorly with insulin, making it difficult for it to penetrate tissues. To overcome the obstacle, the pancreas begins to produce more insulin 1.
This entails the depletion of beta cells responsible for gene production. Over time, there is not enough insulin to maintain blood glucose at normal levels. The insensitivity of insulin-dependent tissues to insulin is called insulin resistance. The main cause of diabetes in women is obesity. Others include genetics, family history, age 1.
Signs in women over 40
After 40 years of age, there is a danger of developing both type 1 and type 2 disorders. The main reasons for developing this pathology are a sedentary lifestyle and overeating. The autoimmune system begins to attack the pancreas, where insulin is produced. It's not known why, but thin women have a higher risk of developing diabetes without actively developing symptoms.
Insulin injections are rarely required. The main focus of treatment is on a low carbohydrate diet. A healthy lifestyle will help support the body in the fight against the problem. The main thing is not to get caught up in unhealthy sweets and other temptations. Otherwise, all previous treatment will go to waste.
Symptoms of type 1 diabetes in women
Type 1 diabetes mellitus is characterized by an early age of onset, although in a small percentage of cases (5%) it also occurs in older generations. It mainly affects girls, young women and young women under 25 years of age. In 50% of cases, the disease is diagnosed in children under 10 years of age 1.
Symptoms appear unexpectedly and quickly, which are easy to recognize:
- copious amounts of urine with frequent urination;
- an irresistible feeling of hunger and thirst (due to loss of fluid in the urine);
- sudden loss of body weight even with increased appetite;
- lethargy, apathy, drowsiness (due to the lack of insulin, the body lacks energy);
- temporary vision problems;
- pungent odor of acetone from the mouth;
- vomiting and nausea 1.
University
→ Home → University → University in the media → Modern classification and diagnosis of diabetes mellitus
The photo is for illustrative purposes only. From open sources
The relevance of changing approaches to the classification of diabetes mellitus (DM) is due to the variety of clinical manifestations and the need for a differentiated choice of treatment tactics. Work on this publication coincided with the final stage of preparation by the working group of national protocols for the diagnosis and treatment of diabetes, a working version of which is available on the website of the Republican Center for Medical Rehabilitation and Balneotherapy, which was used to indicate diagnostic criteria.
Approach navigator
Understanding diabetes as a syndrome of chronic hyperglycemia determines its diagnostic criteria, given in Table. 1.
The diagnosis of diabetes is established based on a combination of two laboratory indicators that meet the diagnostic criteria for diabetes:
- fasting blood glucose (two tests performed on different days);
- fasting blood glucose and HbA1c;
- blood glucose on an empty stomach and 2 hours after a load of 75 g of glucose or
- blood glucose in a random analysis in the presence of classic symptoms of hyperglycemia or dehydration and catabolism.
In case of newly diagnosed hyperglycemia against the background of a critical condition, to establish a diagnosis, it is necessary to evaluate HbA1c: an HbA1c level of >6.5% indicates in favor of diabetes.
Reasons for the need to use new classification approaches include:
- decreasing differences in the phenotypes of type 1 and type 2 diabetes as the prevalence of obesity in childhood and young adulthood increases;
- detection of type 1 diabetes in adulthood, including in association with autoimmune diseases;
- developments in the field of molecular genetics that make it possible to identify monogenic forms of diabetes.
In 1980, WHO proposed a well-known etiological classification of diabetes, which changes periodically. In recent years, there have been calls to update the classification system for diabetes because many patients did not fit into either type.
The accumulation of new data led to the fact that in 2021 the WHO updated the classification of diabetes, which is based on the etiopathogenetic principle. The proposed classification is based on the potential for use in real-life clinical practice, since many laboratory tests that can improve the differentiation of types of diabetes and improve the effectiveness of treatment are not available in most clinical settings worldwide. The classification of diabetes for 2021 is given in table. 2.
Diabetes mellitus type 1
Although type 1 diabetes has been called “childhood” or “adolescent” for many years, global trends indicate that 42% of type 1 diabetes occurs in people over 30 years of age.
Diagnostic criteria for type 1 diabetes:
- acute onset;
- presence and progression of clinical symptoms;
- ketonuria;
- young age;
- the presence of first-degree relatives with type 1 diabetes and/or autoimmune pathology in the patient.
If differential diagnosis is necessary, the diagnosis is confirmed by a reduced level of C-peptide and the detection of increased levels of diabetes-associated antibodies. Confirmation of type 1 diabetes determines the need for insulin replacement therapy (IT).
Diabetes mellitus type 2
It accounts for 90–95% of all types of diabetes, is most common in adults, but given the prevalence of overweight and obesity in children, there is an increase in the number of children with this disease.
Common characteristics include the combination of β-cell dysfunction with relative insulin deficiency and insulin resistance (IR) in the setting of overweight or obesity (predominantly visceral). The pathophysiological mechanisms of development of type 2 diabetes reflect different mechanisms, so it is likely that its subtypes will be defined in the future.
Type 2 diabetes often remains undiagnosed for many years due to oligosymptoms, but chronic hyperglycemia, which does not lead to noticeable symptoms of diabetes, determines an increased risk of cardiovascular pathology and microvascular complications.
Risk factors for developing type 2 diabetes:
- overweight or obesity;
- age over 45 years;
- family history (DM in first-degree relatives);
- arterial hypertension;
- presence of other cardiovascular diseases;
- hypercholesterolemia, hypertriglyceridemia;
- habitually low physical activity;
- birth of a child weighing >4 kg or evidence of a history of gestational diabetes;
- polycystic ovary syndrome.
The risk of type 2 diabetes is considered high if you are overweight or obese and have one (or more) other risk factors.
Clinical diagnostic criteria for type 2 diabetes:
- age 40 years and older;
- overweight or abdominal obesity;
- absence of ketonuria;
- family history of type 2 diabetes.
Due to oligosymptoms, diagnosis requires obtaining pathological laboratory data twice.
HbA1c is not recommended for anemia, hemoglobinopathy, hemodialysis, recent blood loss or after blood transfusion, treatment with erythropoietin.
An oral glucose tolerance test with a 75 g glucose load (OGTT) is performed when questionable glycemic values are obtained. OGTT is not performed:
- against the background of acute diseases;
- against the background of short-term use of medications that increase glycemic levels;
- with diagnosed diabetes or identified fasting glycemia of more than 7.0 mmol/l or random hyperglycemia of more than 11.1 mmol/l.
For most people with type 2 diabetes, insulin treatment is not necessary but may be necessary to reduce hyperglycemia and prevent chronic complications. As a rule, patients receive treatment with oral glucose-lowering drugs, the action of which is aimed at various parts of the pathogenesis.
Hybrid forms of diabetes
The identification of this type (isolated for the first time) is a consequence of the difficulties in differentiating type 1 and type 2 diabetes. Based on the characteristics of clinical manifestations, hybrid forms of diabetes include:
- slowly developing immune-mediated diabetes;
- Type 2 diabetes, prone to ketosis.
A slowly developing form of autoimmune diabetes in adults was described as diabetes manifesting similarly to type 2 diabetes, but with proven signs of autoaggression (increased antibodies to glutamic acid decarboxylase (GAD), tyrosine phosphatase (IA-2), insulin or transporter 8 zinc (ZnT8)). This form of diabetes is called latent autoimmune diabetes in adults (LADA - Latent Autoimmune Diabetes of Adult), which is subject to critical reflection. It is important that the need for IT when making a diagnosis is not obligatory and it is possible to control the disease with lifestyle changes and oral medications.
In 2021, a consensus statement of experts on LADA was published, defining diagnostic criteria for the pathology:
- age over 30 years;
- history of the presence of autoimmune pathology;
- the rarity of identifying components of the metabolic syndrome and the absence of cardiovascular diseases;
- the decrease in C-peptide levels is slower than in diabetes;
- positive GAD antibodies (the most sensitive marker) and other diabetes-associated antibodies;
- does not require IT when manifesting diabetes (Management of Latent Autoimmune Diabetes in Adults: A Consensus Statement From an International Expert Panel. Buzzetti R., Tuomi T. et al. Diabetes 2020, 69 (10) 2037-2047).
Confirmation of the diagnosis of LADA is carried out on the basis of the given algorithm and is based on determining the level of C-peptide in patients with positive GAD antibodies.
Shown in Fig. Algorithm 1 identifies patients with C-peptide levels between 0.3 and 0.7 nmol/L as patients with LADA.
Rice. 1
When C-peptide levels are 0.3–0.7 nmol/L, it is recommended to start treatment with dipeptidyl peptidase 4 inhibitors, sodium cotransporter 2 inhibitors, glucagon-like peptide 1 receptor agonists, or thiazolidinediones (non-sulfonylureas) (see Fig. 2). If target glycemic levels are not achieved, combination therapy can be used, and only when all possibilities have been exhausted is IT initiated.
Rice. 2
Discussions on the issue of slowly developing immune-mediated diabetes continue. The question of whether this condition is a separate disease or a stage of the process leading to type 1 diabetes remains open.
Type 2 diabetes prone to ketosis
An unusual form of ketosis-prone nonimmune diabetes was first described in young African Americans and later in other populations. The characteristic signs of the pathology are a combination of ketosis and signs of severe insulin deficiency with the development of remission and the absence of the need for IT for a fairly long time (up to 10 years), which resembles the course of type 2 diabetes. More often, this type of diabetes is detected in men and is not related to body weight. The main pathogenetic features of this disease are unclear.
Ketosis-prone type 2 diabetes can be differentiated from type 1 diabetes and classic type 2 diabetes. Glucotoxicity is considered to be a factor causing acute and recurrent β-cell failure. Restoring normoglycemia after initiation of IT leads to optimization of the secretory function of β-cells and eliminates the need for IT.
Other specific types of diabetes
Specific diabetes is a group of heterogeneous diseases characterized by a syndrome of chronic hyperglycemia caused by absolute or relative deficiency of insulin with dysfunction of vital organs and systems, with the exception of other types of diabetes included in this classification (see Table 3).
Monogenic forms of diabetes are based on the identification of a pathological mutated gene, which leads to the development of clinical manifestations. The diagnosis can only be reliably established based on the results of genetic testing. The listed variants of monogenic forms of diabetes include familial forms (MODY - maturity onset diabetes of the young) with early onset (before the age of 25 years), which is insulin-independent and occurs as a result of β-cell dysfunction. The most common genetic subtypes are associated with mutations in the glucokinase gene (GCK MODY) and the hepatonuclear factor gene (HNF1α MODY and HNF4α MODY).
Phenotypic manifestations and responses to treatment in different forms of monogenic diabetes vary. For example, with GCK MODY, lifelong mild fasting hyperglycemia persists with rare complications and does not require pharmacotherapy. The most common form, HNF1α MODY, on the contrary, leads to progressive and severe hyperglycemia with a high risk of vascular complications, but patients with this pathology remain highly sensitive to sulfonylurea derivatives.
Clinical manifestations are determined by the degree of decompensation of carbohydrate metabolism and the underlying disease. The most commonly recorded specific diabetes is caused by a pancreatogenic factor. Potential clinical manifestations include deafness, visual impairment with retinal atrophy, manifestations of encephalopathy, changes in appearance (growth disorders, elf-like face, pterygoid folds of the neck, large ears, micrognathia, lack of subcutaneous fat, impaired sexual development, acanthosis nigricans, etc. ). An assessment of family and drug history is obligatory. The form of specific diabetes is determined by anamnesis and examination confirming the presence of pathology that can cause diabetes. Treatment tactics are determined individually.
Unclassified diabetes
Conducting a full diagnostic search when identifying a disease aimed at clarifying the type of diabetes is becoming increasingly complex and is not always available in full, which has led to the inclusion of the category “unclassified diabetes.” Establishing this diagnosis is valid before establishing the cause of the pathology using anamnesis, examination and modern examination methods (presence or absence of ketosis or ketoacidosis, diabetes-associated AT, secretion of C-peptide, etc.).
Hyperglycemia first identified during pregnancy
It should be classified as diabetes diagnosed during pregnancy or as gestational diabetes (GDM), which is borrowed from the WHO publication “Criteria for the diagnosis and classification of hyperglycemia first identified during pregnancy” (2013).
The diagnosis of diabetes during pregnancy should be made if one or more criteria are present:
- fasting plasma glucose ≥7.0 mmol/L;
- plasma glucose level 1 hour after ingestion of glucose at a dose of 75 g ≥11.1 mmol/l;
- plasma glucose level ≥11.1 mmol/L at any time in the presence of symptoms of diabetes;
- HbA1c more than 6.5% in early pregnancy.
The diagnostic criteria for GDM are given in Table. 4.
The diagnosis of GDM can be established when one of the indicators increases after a load of 75 g of glucose.
In case of GDM and DM and pregnancy, only lifestyle correction and IT can be used as treatment options; all tableted antihyperglycemic drugs are contraindicated.
Conclusion
Obviously, the modern classification of diabetes is based on the potential assessment of new data on the characteristics of the development and treatment of diabetes and will be useful in real clinical practice. Tatyana Mokhort, Head of the Department of Endocrinology, BSMU, Doctor of Medicine. sciences, professor; Natalia Karlovich, chief physician of the Republican Center for Medical Rehabilitation and Balneotherapy, chief freelance endocrinologist of the Ministry of Health, candidate of medical sciences. Sciences Medical Bulletin, December 10, 2020
Share
Symptoms of type 2 diabetes in women
Type 2 diabetes mellitus is typical for people aged 40 to 60 years who are overweight 2. Insulin resistance develops in them due to the consumption of large amounts of carbohydrate foods. This type includes 80-90% of all cases of disease, and it is inherited in 90-95% of cases. 1. The symptoms of type 2 disease do not differ from the symptoms of type 1 diabetes, since they have the same cause - high blood glucose levels.
Other signs may include:
- skin itching;
- weakness;
- infectious skin lesions (boils, carbuncles, small ulcers);
Additional symptoms of diabetes in women with untimely identified type 2 disease manifest themselves in the form of cataracts, joint pain, and angina pectoris 1.
Features of the course in girls
Statistics show that women are much more likely to suffer from the manifestations of pathology.
This especially applies to the second type of disease. This is due to the fact that the weaker sex has more adipose tissue, and, on the contrary, less muscle mass than men. The fact is that adipose tissue does not absorb insulin and does not utilize glucose well. Girls are also more susceptible to stress, which provokes the release of steroid hormones and increased glucose levels. A particular danger in the development of pathology is the love of sweets. Frequently eating cakes and pastries leads to an increase in fat. This leads to activation of the disease in women. Girls also develop another type of pathology - gestational. But we'll talk about it later.
Features of the manifestation of the disease in women
The specific characteristics of the female body influence the manifestations of the disease. Since a woman is more dependent on fat metabolism in the body than a man, diabetes, regardless of age, can manifest itself as:
- rapid gain of excess weight, turning into obesity;
- sudden weight loss;
- excessive appetite 1.
Signs of type 2 disease are often itching and burning of the skin, dryness of the mucous membrane of the external genitalia 1. Unpleasant sensations in the genital area are the result of many reasons, including hormonal changes, which, for example, occur during menopause, pregnancy, and menstruation. Therefore, due to the uncertainty of their origin, a woman does not always consult a doctor in a timely manner.
Primary manifestations of diabetes mellitus in women also include:
- tingling and temporary loss of sensitivity in the skin of the hands, feet, and genital area;
- menstrual irregularities;
- vaginal and oral candidiasis;
- polycystic ovary syndrome, expressed in darkening of the skin on the elbows, neck, and armpits (with a predominance of male hormones over female ones)1
How to fix
If you notice symptoms of high blood sugar, you should immediately go to the hospital to identify the cause of hyperglycemia. Depending on the provoking factor, the necessary therapy is prescribed.
Otherwise, hyperglycemia in the human body will lead to irreversible processes and provoke the development of vascular and skin diseases, indolent infections, depression, and sleep problems.
Depending on the cause and severity of hyperglycemia, your doctor may prescribe medications. To reduce high blood sugar levels, it is important to learn how to properly cope with stressful situations and regularly devote time to physical activity.
It is also important to pay special attention to your diet and choose foods with a low glycemic index.
You can include in your diet:
- seafood and lean fish, including lobster, crab and lobster;
- mushrooms;
- cereals;
- vegetables and greens such as cabbage, broccoli, zucchini, radishes, pumpkin, spinach, carrots, tomatoes, cucumbers, bell peppers, celery, asparagus, horseradish, onions, Jerusalem artichoke;
- soy and soy cheeses, including tofu;
- flaxseed, butter and rapeseed oil;
- berries and fruits such as cherries, raspberries, avocados, apples, kiwis, grapefruits and lemons;
- spices such as mustard, cinnamon and ginger;
- legumes, including lentils;
- walnuts, almonds, cashews;
- milk and dairy products, such as low-fat cottage cheese and kefir;
- lean meats;
- eggs, but not more than 1 piece per day.
It is recommended to steam, stew, bake, and boil dishes. Food should be taken in small portions, at the same time, to reduce the risk of a sharp jump in sugar.
Diabetes mellitus during menopause
A woman is at maximum risk of the disease at the age of 50 years and older, while a man on average gets sick earlier - at 35-40 years 1. This is due to the onset of menopause. In the female body, the production of estrogens sharply decreases, which stimulate the secretion of the hormone insulin by the endocrine apparatus of the pancreas, thereby affecting blood sugar levels. During menopause, metabolism and fat distribution are disrupted, which in turn prevents the effective participation of insulin in maintaining glycemia at a stable level 2. Thus, menopause has a direct impact on the risk of the onset and development of the disease.
Diabetes and pregnancy
If signs of diabetes mellitus in women are detected during pregnancy, it receives the technical name “gestational”, indicating the period of time from conception (the day of the last menstruation) until the birth of the child 1. This type of disease is associated with the restructuring of the female body and changes in the volume of hormones produced. Some of them interfere with the action of insulin. The first signs of the disease appear, as a rule, at the 24th week of fetal development; it occurs as type 2 diabetes 1.
Risk factors for the disease during pregnancy include:
- family inheritance;
- obesity;
- age (from 25-30 years);
- previously observed elevated blood glucose levels;
- arterial hypertension;
- glucosuria;
- weight gain during pregnancy;
- undiagnosed prediabetes 1
It must be emphasized that with proper treatment, pregnant women give birth to completely normal children. The lack of competent treatment and supervision by medical staff, on the contrary, is dangerous for women’s health and the fetus.
If the diagnosis is not confirmed
If the examination did not confirm the presence of diabetes, but identified factors for its development, then you need to be attentive to your health and not neglect prevention. Don't forget that prevention is always better than cure. Patients at risk are advised to follow a diet, lead an active lifestyle and have their blood glucose tested once a year.
If prediabetes is detected
Proper diet and lifestyle can help delay or prevent the onset of diabetes. Prediabetes indicates an early disorder of carbohydrate metabolism. Signs of prediabetes include impaired fasting blood glucose and impaired glucose tolerance. Patients are advised to consume less easily digestible carbohydrates and increase physical activity. In addition, it is recommended to be examined by a therapist at least once a year and have your blood glucose tested.
If you have been diagnosed with type 2 diabetes mellitus
Once the diagnosis of diabetes has been confirmed, treatment should not be delayed. First, you need to go to an appointment with an endocrinologist to clarify the concomitant pathology and select individual treatment. A referral to an endocrinologist will be given by a therapist or general practitioner if, as a result of the examination, it turns out that the level of blood glucose in venous plasma exceeds 7.0 mmol/l, and glycated hemoglobin is higher than 6.5%. The endocrinologist determines the individual target level of glycated hemoglobin (HbA1c) for the patient and develops glucose-lowering therapy based on the examination results and the presence of concomitant diseases.
Additional examinations
An endocrinologist may prescribe additional examinations for the patient. This is necessary to anticipate possible complications of T2DM. As an additional examination, the endocrinologist may refer the patient to an ophthalmologist to check the condition of the fundus and evaluate visual acuity at the time of diagnosis of type 2 diabetes.
There are a number of mandatory examinations that a patient with T2DM must undergo every year. These include ECG and chest x-ray. If indicated, the patient may be referred for additional examinations:
- See a cardiologist for arterial hypertension and dyslipidemia;
- See a nephrologist or urologist for kidney pathology;
- See a neurologist if you complain of loss of sensation in the limbs and poor wound healing.
Selection of treatment and free medications
The treatment program for the patient is drawn up by an endocrinologist. There is no standard program, since treatment is selected taking into account the patient’s lifestyle, the presence of concomitant diseases and a tendency to hypoglycemia. While the selection and correction of insulin therapy is underway, the patient should regularly visit an endocrinologist.
It is useful to know that patients with diabetes can receive preferential drug coverage; benefits apply to:
- hypoglycemic drugs and other medications prescribed by your doctor;
- means for administering insulin;
- means for self-monitoring of glycemia;
- consumables for insulin pump.
Medicines can be obtained with a prescription from a doctor. They are issued at the pharmacy of the clinic to which the patient is assigned. Prescriptions are issued for a period of no more than 90 days. If the drug is not available, the prescription is registered in a special journal in the prescribed form, and the drug is delivered to the point within 10 days.
Diagnosis of the disease
At the initial stage, diagnosis consists of laboratory tests. First of all, a general analysis of urine and blood is performed. A biochemical blood test is also performed, which determines the quantitative content of glucose, urea nitrogen, metabolic products - creatinine and electrolytes, gas composition is determined, etc. 3.
The composition of urine is tested for the presence of ketone bodies. If any are detected, their presence in the blood serum is determined.
Additional examination methods can be used to diagnose the disease:
- electrocardiography of cardiac muscle activity;
- chest x-ray;
- analysis of biological material of body fluids.
T2DM
Type 2 diabetes mellitus (T2DM) most often affects people over 40 years of age. This form of diabetes is characterized by relative insulin deficiency. For a long time, the disease may not manifest itself at all; symptoms appear gradually, so people often seek help late. Over time, the patient may need insulin therapy. Type 2 diabetes mellitus is treated mainly on an outpatient basis.
The risk of developing T2DM is higher in the following groups of people:
- age over 45 years;
- overweight (body mass index more than 25 kg/m²);
- high blood pressure (arterial hypertension, above 140/90 mm Hg);
- genetic predisposition (close relatives suffer from T2DM);
- low physical activity;
- elevated blood triglyceride levels (≥ 2.82 mmol/L) and decreased HDL cholesterol levels ≤0.9 mmol/L.
For people who are at risk, doctors recommend doing a blood test at least once a year and monitoring their glucose levels.
Symptoms of T2DM
Type 2 diabetes mellitus does not have specific symptoms that can clearly identify the disease, but the appearance of several symptoms of the disease at the same time may be a sign of the development of T2DM. Check if you have three or more symptoms from the list below, this is a reason to see a doctor:
- you feel dry in your mouth and constantly thirsty;
- you have excessive urination, including at night;
- your skin and mucous membranes are itchy;
- you quickly get tired and feel weak;
- your wounds and skin damage are healing slowly;
- pustules appear on the skin;
- you have lost a lot of weight and suddenly for no apparent reason.
What to do if you suspect you have T2DM?
If you feel unwell and experience symptoms of diabetes, the first thing you should do is consult a doctor. An examination performed by a therapist or general practitioner will help identify T2DM. To register at the clinic, you will need a passport and compulsory medical insurance policy. The doctor will decide on the need for further examination based on the results of the examination.
The following tests help identify T2DM:
- general blood analysis;
- general urine analysis;
- biochemical blood test with blood glucose testing;
- biochemical blood test to assess lipid metabolism disorders;
- determination of the level of glycated hemoglobin in the blood;
- oral glucose tolerance test.
All of the above tests can be done at the clinic at the site of attachment. The results will be ready 1-2 days after submission. The diagnosis may be as follows:
- diabetes mellitus has not been confirmed, but there are factors for its development;
- prediabetes was detected;
- type 2 diabetes mellitus was diagnosed.
Diabetes treatment
After confirming the diagnosis of type 1 diabetes, treatment with insulin is prescribed, which compensates for the lack of production of the gene by the body’s own 3. The most important element in the treatment of type 2 disease is diet.
In the first case, a diet is also necessary, and the patient must carefully monitor the diet, evaluate and take into account the amount of carbohydrates in dishes and sugar in order to correctly calculate the dose of insulin.
In the second case, the main goal is to combat obesity. It is carried out not only with the help of diet, but also with physical activity, by giving up bad habits, etc. In case of morbid obesity, bariatric surgery is indicated - surgical reduction of the size of the stomach 1.
A mandatory condition for the treatment of diabetes mellitus in women is constant monitoring of blood sugar levels. For this purpose, special devices are used - glucometers, which can work with blood from a finger and other parts of the body.
Increased thirst and urination.
This is the most common sign of diabetes. Since insulin is not produced by the body, or is produced in insufficient quantities, sugar is in free flight. Once in the kidneys, sugar is excreted along with urine, simultaneously collecting fluid from other tissues, thus loading the kidneys and dehydrating the body. As a result, a person begins to drink more water, trips to the toilet increase, forming a kind of vicious circle. A person becomes constantly tired and irritable (who enjoys spending days involuntarily engaged in the “water cycle in nature”!), in addition to the kidneys, the heart is also in a stressed state, because Sugar safely “removes” fluid from the circulatory system, the blood becomes viscous and thick, and the heart has to push it to the peripheries with redoubled force, raising blood pressure.
Drug treatment
The current concept of treatment for type 1 diabetes involves injections of insulin, which is produced by the pharmaceutical industry in the form of pen syringes.
The injection regimen consists of two parts:
- injection of a long-acting hormone under the skin for 12–24 hours (administered 1–2 times a day), which covers the body’s need for insulin at night and between meals;
- introduction of “ultra-short” insulin or, as it is also called, insulin “for food”. It is used after meals or when signs of unwellness to reduce excessive glucose increases1
In the treatment of type 2 disease, insulin is rarely used, only if other approaches are ineffective. In both cases, patients take additional glucose-lowering drugs, as well as medications that prevent the development of possible complications 3.
Evaluation of treatment effectiveness
The effectiveness of the prescribed treatment must be monitored and, if necessary, the treatment program adjusted. In addition, it is important to identify emerging complications at an early stage. To do this, patients are recommended to check glycated hemoglobin every three months, microalbuminuria (MAU) every six months, and undergo a clinical examination once a year.
Patients with diabetes mellitus of the first group are registered with an endocrinologist, and patients with T2DM, after selecting appropriate therapy in the absence of severe cardiovascular diseases, are observed by a therapist or general practitioner. If the patient's condition worsens, the therapist can re-refer him to an endocrinologist to adjust the therapy. If the complications that arise lead to a person’s loss of ability to work, he is assigned a disability, but this is done on the basis of the conclusion of a medical and social examination.
Diet
The diabetes diet is aimed at reducing body weight mainly in diabetics with type 2 disease. It involves avoiding foods rich in carbohydrates. The main essence of the diet is to organize timely nutrition with high-quality products and maintain target blood glucose values.
The choice of food products, as well as the mode of their consumption, is determined by a qualified nutritionist or endocrinologist. When compiling a diet, the type of disease must be taken into account, i.e. whether insulin is produced by the body on its own or requires injection in a certain dose.
Disease prevention
The best methods for preventing diabetes in women are regular physical activity, proper nutrition and an overall healthy lifestyle. Physical activity in the form of walking and jogging, swimming, cycling, fitness accelerates metabolism, stabilizes hormone levels, smoothes out hormonal fluctuations, helps 4:
- to burn calories;
- control body weight;
- minimize the level of “bad” cholesterol;
- absorption of oxygen by the body;
- prevent the development of heart disease;
- improve sleep.
Healthy and proper nutrition does not necessarily require giving up traditional or national cuisine. The main thing in it is the balance of proteins, fats and, first of all, carbohydrates, for which it is enough to adhere to the general rules for eating foods.