All organs, tissues, structures and systems of the human body can be susceptible to inflammatory processes. This even applies to the system of blood vessels, where, it would seem, there is nothing to become inflamed - except the vascular walls. In medicine, there are several general terms to refer to vascular inflammation (vasculitis, angiitis), as well as a number of specific terms indicating the nature or localization of the affected vessels (arteritis, phlebitis, etc.).
The eyeball is “braided” with a network of thin blood vessels that nourish and saturate with oxygen all intraocular elements and media. The ocular vascular system, in its organization, is essentially no different from any other: blood enriched in the lungs enters the arteries, is delivered and distributed in the tissues by the smallest capillaries, then is discharged, along with metabolic products, through the veins. Normally, the vascular network of the eye is practically invisible; if we notice swollen, inflamed or, in common parlance, “burst” eye vessels, this is always a pathology and always a symptom.
The blood supply system of the eye is called the “uveal tract” and consists of the iris (anterior section), ciliary body (middle section, also responsible for accommodation) and choroid (posterior section, which can be called strategic: this is the choroid itself, providing nutrition and oxygenation and regeneration of the photosensitive retinal tissue that covers the inside of the fundus of the eye).
In accordance with the rules of word formation accepted in medicine, inflammation of the vascular system of the eye is designated by the term “uveitis”. It is believed that the original name “uvea” (ancient Greek “grape”) was inspired by the grape-shaped appearance of the ocular choroid, which association becomes especially clear during inflammation.
General information
Uveitis is an inflammatory disease of the choroids of the eye, or more precisely, the uveal tract, consisting of 3 sections: the iris, the ciliary body and the choroid itself.
In most cases, approximately 25%, the pathology causes poor vision and blindness. Most often it is caused by an infection of the blood vessels of the eyes, but there may be other etiological factors. Pathological changes cause pain, severe exudation and lead to the formation of adhesions of the iris and lens, the outpouring of exudate into the vitreous body and atrophy of the eyeball.
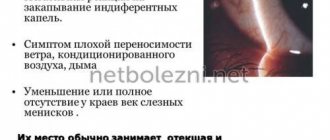
You can suspect that you have ocular uveitis if you often experience a feeling of “fog” before your eyes, spontaneous lacrimation, photophobia, swelling of the eyelids, and your eyes look cloudy and red.
Children's features
Since the disease often occurs against the background of reduced immunity, special attention should be paid to children with chronic pathologies in order to promptly identify uveitis in children.
You can identify a certain risk group in order to be regularly examined by an ophthalmologist. Children with the following diseases should be examined for uveitis:
- diabetes;
- vegetative-vascular dystonia;
- liver or kidney failure;
- obesity;
- impaired metabolism.
Pathogenesis
There are differences between the blood supply to different parts of the human eye; the choroid itself requires normal blood flow from the posterior short ciliary arteries, while the iris and ciliary body are supplied with arterial blood - the long anterior and posterior ciliary vessels. Since the blood supply to these two sections is different, damage to the anterior and posterior sections of the choroid occurs separately as a result of the inflammatory process.
The choroid is characterized by the presence of a small number of T- and B-lymphocytes, as well as mastocytes and fibroblasts. The pathogenesis and development of the inflammatory process is based on the accumulation of plasma cells, monocytes, T- and B-lymphocytes, including their penetration into aqueous tissues. The most important role is played by the soluble S-antigen and photosensitive opsins of the retina.
Congenital aniridia
| A disease in which the iris is absent (see structure of the eye). At the same time, behind the cornea there is a picture of a maximally dilated pupil, that is, blackness. Sometimes a rim is visible - a remnant (rudiment) of the iris root and ciliary processes (see.
|
You can find out more about surgical treatment here
Classification
Against the background of general diseases, primary uveitis develops, while in case of eye pathologies - keratitis , scleritis , retinitis , uveitis is considered secondary. In exogenous forms of the disease, the causes are penetrating wounds of the eyeball, postoperative complications, perforated ulcers of the cornea, and in endogenous forms, toxic-allergic and metastatic phenomena.
Depending on the location of the inflammatory process, it is customary to distinguish:
- Isolated anterior uveitis, or otherwise called iridocyclitis , iritis or cyclitis (since it is almost impossible to separate them clinically due to the common blood supply), which is characterized by damage to the iris and ciliary body, occurs most often - in 80% of cases.
- Peripheral (intermediate) type uveitis, involving in the pathological process a flat area of tissue of the ciliary body and the choroid proper on the periphery (choroid), as well as the vitreous body and retina, which leads to a more significant decrease in visual acuity in the central localization of the pathological process.
- Posterior uveitis, its other name is choroiditis , which means inflammation of the choroid itself; the pathology can affect not only the choroid, but also the retina, as well as the optic nerve - and then we are talking about chorioretinitis .
- Panuveitis ( iridocyclochoroiditis ) is a type of uveitis in which total inflammation of the entire uvea and uveal tract occurs, and the clinical picture combines symptoms of both anterior, intermediate and posterior uveitis.
Considering the nature of the inflammatory process, it is customary to distinguish between serous, purulent, fibrinous, hemorrhagic and mixed uveitis.
If morphological inflammatory changes are taken into account, then uveitis is:
- granulomatous – metastatic hematogenous;
- non-granulomatous – initiated by toxic or toxic-allergic factors.
The difference between the symptoms of chronic and acute granulomatous and non-granulomatous uveitis
Rheumatic uveitis
Against the background of a complex general chronic infectious-allergic disease - rheumatism , rheumatic uveitis develops in 3-8% of cases. The impetus for the manifestation of the disease can be hypothermia and other factors that reduce the body's resistance. At risk are children under 3 years of age. In rheumatic uveitis, the course is acute and violent, with a sharp mixed injection of the eyeball, hemorrhages under the conjunctiva and into the anterior chamber, as well as the development of hyphema, multiple pigmented posterior adhesions on the iris and small gray precipitates on the cornea. The exudate in the anterior chamber is characterized by a gelatinous consistency. The clinical picture develops quickly - within 1.5-2 months and affects both eyes; relapses are possible with rheumatic attacks.
Uveitis in sarcoidosis
Sarcoidosis is a disease that is often accompanied by uveitis. It is characterized by such signs as the presence of granulomas, which are not characterized by caseous necrosis and are drops of lamb fat. In addition, the occurrence of secondary glaucoma , nodules (wax drops) at the edge of the pupil or around the vessels of the iris is possible. In some cases, sarcoidosis manifests itself exclusively as pathology of the eyes, but most often the development of lymphadenitis of the cervical, axillary, and inguinal lymph glands occurs with damage to the mucous membranes of the respiratory tract.
Treatment
Drug treatment
.
Treatment of uveitis directly depends on the cause of the disease.
Due to the fact that it is often not possible to establish it, regimens contain drugs that are symptomatic or prescribed empirically until the etiology of inflammation is established. Specific treatment should be applied after identifying the cause of the disease. The gold standard of treatment is corticosteroids . The main goals of the prescription are: reducing exudation, stabilizing cell membranes, inhibiting the production of inflammatory hormones and the lymphocytic reaction. The choice of a specific drug of this group, as well as the method of administration, is carried out taking into account the activity of the inflammatory process, the tendency to increase IOP, etc. Currently, local and systemic use is possible, as well as installation of an implant into the cavity of the eyeball or under the membranes of the eye that releases the medicinal substance in small doses over a long period of time.
The next most often prescribed for uveitis are drugs with cycloplegic and mydriatic action. Their use is due to the prevention of the formation of synechiae (fusions) of the iris with surrounding structures, reducing pain by reducing spasm of the pupillary and ciliary muscles, stabilizing the blood-ophthalmic barrier and preventing further leakage of protein into the aqueous humor.
Second-line drugs are NSAIDs. They have less anti-inflammatory activity compared to steroids, but can be useful for relieving pain, inflammatory reactions, preventing and treating relapses of the disease, as well as macular edema accompanying it in some cases. When prescribed together with corticosteroids, NSAIDs help reduce the dose of the former required to relieve inflammation during long-term treatment of some forms of chronic uveitis. The drug can be prescribed both in the form of eye drops and in tablet form.
Separate attention should be paid to a relatively new group of drugs - immunomodulators, which are now successfully used in some forms of the disease (for example, caused by Behçet's disease, involving the posterior segment of the eye; Wegener's granulomatosis; necrotizing scleritis). This group includes antimetabolites (methotrexate, azathioprine, mycophenolate mofetil), T-lymphocyte inhibitors (cyclosporine and tacrolimus), alkylating agents (cyclophosphamide, chlorambucil). The goal of this therapy is targeted inhibition of certain mechanisms of the immune inflammatory response that led to damage to the organ of vision (immunosuppression). The drugs can be used both together with corticosteroids and without them, allowing to reduce the negative impact of the latter on the body.
Recently, it has also become possible to use in special forms of the disease (serpinginous choroiditis, shotgun chorioretinitis, sympathetic ophthalmia; caused by Behçet, Vogt-Koyanagi-Harada diseases, juvenile idiopathic arthritis, seronegative spondyloarthropathies) drugs inhibitors of growth factor-α tumors, or so called biological therapy. The most commonly used are adalimumab and infliximab. All biological agents are “second-line” drugs in the treatment of these diseases and are used in cases where previous therapy was unsuccessful.
Surgery
The goals of this type of treatment are visual rehabilitation, diagnostic biopsy to clarify the diagnosis, removal of clouded or altered structures that make it difficult to examine the posterior segment of the eye or contribute to the development of complications (cataracts, vitreous destruction, secondary glaucoma, retinal detachment, epiretinal membrane), administration of drugs directly to the site of inflammation. Also, removal of the affected eye structures can help relieve the inflammatory process. The most commonly used surgical methods include vitrectomy, phacoemulsification, glaucoma filtering surgery, and intravitreal injections.
The success of these interventions directly depends on the timeliness of their implementation, the stage of the disease, and the prevalence of irreversible changes in the eyeball.
Prognosis for the treatment of uveitis
Patients suffering from uveitis should be informed of the importance of following the prescribed treatment and examination regimen. This is the main factor determining a favorable prognosis for the outcome of the disease. Some forms of the disease are capable of recurrence, even despite adequate treatment.
Of course, uveitis itself is not fatal, but if not treated adequately it can cause blindness.
Application
Recommendations on the scope of diagnostic measures for various forms of uveitis. .
Bibliography
1) Saadia Zohra Farooqui, MBBS Senior Resident, Singapore National Eye Centre, Singapore General Hospital, Singapore, Uveitis Classification, 2021. [Medscape] 2) Monalisa N Muchatuta, MD, Iritis and Uveitis Clinical Presentation, 2021. [Medscape] 3) Herbert HM, Viswanathan A, Jackson H, Lightman SL. Risk factors for elevated intraocular pressure in uveitis. J Glaucoma. 2004;13(2):96–9 4) C. Stephen Foster, Albert T. Vitale. Diagnosis and treatment of uveitis. Jaypee-Highligths, 2013. 5) Niaz Islam, Carlos Pavesio, Uveitis (acute anterior), 2009. [Academia] 6) Robert H Janigian, Jr, MD, Uveitis Evaluation and Treatment, 2021. [Medscape] 7) Monalisa N Muchatuta , MD, Iritis and Uveitis Follow-up, 2021. [Medscape] George N. Papaliodis. Uveitis. A practical Guide to the Diagnosis and Treatment of Intraocular Inflammation. Springer, 2021 9) Kanski's Cinical Ophthalmology. A systematic approach. 8th edition. Eisevier, 2021 10) E.A. Egorov. Emergency ophthalmology: Textbook. Pos. M.: GEOTAR-Media, 2005
Risk factors for elevated intraocular pressure in uveitis. J Glaucoma. 2004;13(2):96–9 4) C. Stephen Foster, Albert T. Vitale. Diagnosis and treatment of uveitis. Jaypee-Highligths, 2013. 5) Niaz Islam, Carlos Pavesio, Uveitis (acute anterior), 2009. [Academia] 6) Robert H Janigian, Jr, MD, Uveitis Evaluation and Treatment, 2021. [Medscape] 7) Monalisa N Muchatuta , MD, Iritis and Uveitis Follow-up, 2021. [Medscape] George N. Papaliodis. Uveitis. A practical Guide to the Diagnosis and Treatment of Intraocular Inflammation. Springer, 2021 9) Kanski's Cinical Ophthalmology. A systematic approach. 8th edition. Eisevier, 2021 10) E.A. Egorov. Emergency ophthalmology: Textbook. Pos. M.: GEOTAR-Media, 2005
Author
: Ophthalmologist E. N. Udodov, Minsk, Belarus.
Date
of publication (update): 06/24/2021
Causes
Uveitis can be caused by factors and agents of different origins, which include:
- exogenous and endogenous infections;
- penetrating injuries and burns;
- infectious and allergic agents, immunodeficiencies and the autoimmune nature of the disease.
Main causes of uveitis
Most often, uveitis develops against the background of ankylosing spondylitis and Reiter's syndrome , toxoplasmosis (intrauterine infection), brucellosis , herpes simplex , influenza , meningitis , syphilis (in recent years - less and less), tuberculosis and sarcoidosis, and juvenile rheumatoid arthritis often causes bilateral chronic anterior uveitis, accompanied by the appearance of antinuclear antibodies and Russell bodies ( immunoglobulin in the iris).
In approximately 40% of patients, uveitis develops against the background of systemic diseases, and in 25%, the cause cannot be established, and therefore they speak of the idiopathic nature of the disease.
In recent years, scientists have been able to identify a genetic predisposition to uveitis. It is determined by the HLA genes -B27, -B5, -Bw22, -A29 and -D5. Anterior uveitis, associated with the presence of HLA-B27 in the bloodstream, develops 2.5 times more often in men than in women.
Symptoms of uveitis
Uveitis can be acute, subacute, chronic (if it lasts more than 6 weeks) and often becomes recurrent. The main symptoms usually boil down to the following:
- photophobia (photophobia);
- swelling and redness of the eyes, inflammation and irritation of their surface;
- causeless lacrimation;
- blepharospasm;
- hemorrhages and opacities in the anterior chamber of the eye (more often with serous changes);
- floaters and spots, especially with peripheral uveitis;
- narrowing and fusion of the pupil caused by the adhesion of the pupil to the lens, which subsequently leads to complete fusion of the pupil - disruption of the connection between the anterior and posterior chambers as a result of the accumulation of intraocular fluid in the posterior section and protrusion of the iris anteriorly in the form of a “bombed” iris;
- deterioration of visual acuity and clarity;
- Spontaneously occurring quite severe pain in the eye, which usually intensifies at night, as well as with palpation.
In more severe cases, as in the photo of ocular uveitis, when the retina is involved in the process, patients experience:
- photopsia - flashes and pointless images before the eyes;
- metamorphopsia - distortion of the shape of objects seen;
- scotoma - loss of the central part of the visual fields;
- hemeralopia - deterioration in the acuity of twilight or night vision.
The periodic occurrence of mild pain in the area behind the eyeball is a sign of involvement of the optic nerve in the pathogenesis.
Panuveitis
Generalized uveitis or panuveitis is a serious disease that affects all membranes of the eye. Accompanied by severe impairment of both central and peripheral vision. The disease is dangerous for its complications, the most severe of which are loss of vision and the eye as an organ. Panuveitis is bilateral in nature with varying degrees of severity in the right and left eyes.
The causes of the disease in most cases remain unclear. Pathogenesis is closely related to immune processes. The disease is often detected in sarcoidosis and tuberculosis.
The complaints of patients and the ophthalmoscopic picture are related to which parts of the vascular tract are predominantly affected. Signs of the disease are observed in different combinations and have varying degrees of severity.
Rice. 16. Panuveitis is a serious disease that affects all membranes of the eye.
Rice. 17. Cytomegalovirus infection. Multiple isolated lesions on the retina in the form of “cotton-wool spots”, which arise as a result of occlusion of capillaries and arterioles (retinal infarction).
Rice. 18 and 18.1. Consequences of toxoplasma uveitis. Retinal damage. Retinal scar (photo on the left).
Rice. 19. Behcet's disease (connective tissue disease). Anterior uveitis, hypopyon, retinitis, inflammation of the optic nerve and retinal vasculitis are severe manifestations of the disease.
Tests and diagnostics
Ophthalmic examination, especially in anterior uveitis, often reveals pericorneal or mixed injection, opalescence and optical heterogeneity due to moisture, pigment and blood cells in the anterior chamber, punctate precipitation on the endothelial layer of the cornea, accumulation of fibrin threads and pus (hypopyon), increase, and in severe cases - decrease in intraocular pressure. In this case, the pupil may become more narrowed as a result of fusion or fusion, acquire an irregular scalloped shape due to the occurrence of posterior synechiae, it becomes narrow and sluggishly reacts to changes in lighting intensity. In some cases, exudation into the vitreous body occurs, but in most cases there is swelling of the eye tissue and blurring of the iris pattern. The latter can change color and the patient develops heterochromia, which is associated with a decrease in the number of pigments.
Hypopyon with iridocyclitis
The peripheral process is more characterized by bilateral damage with the formation of exudate and inflammatory cell suspensions in the anterior part of the vitreous.
Thanks to nonspecific laboratory tests and radiation methods, it is possible to detect signs of the underlying or concomitant disease, for example, collagenosis , ankylosing spondylitis , etc.
To determine the location of chronic foci of infection, additional consultation with an infectious disease specialist, otolaryngologist and dentist may be necessary.
Important! In cases of suspected sarcoidosis, a biopsy of the lacrimal glands and affected areas of the eyelids with the conjunctiva, determination of ACE activity and lysozyme . The hilar lymph nodes are examined using chest radiography and gallium scintigraphy.
Coloboma of the iris
| Typically, iris coloboma is located inferiorly at 06.00. clock, resembling a pear or a keyhole (see.
|
You can learn about plastic restoration of the pupil in our video
Install Flash Player to watch the movie.
Diet for uveitis
Diet to boost immunity
- Efficacy: therapeutic effect after 3 weeks
- Terms: 1-3 months or more
- Cost of products: 1600-1800 rubles. in Week
If uveitis is non-traumatic in nature, then the severity of the course and the speed of development of pathogenesis directly depends on the state immunity . Therefore, to prevent uveitis, in addition to eye hygiene and regular examinations by an ophthalmologist, it is important to have a nutritious diet rich in vitamins (especially A and E) and foods that increase the body’s resistance. It is advisable to include in the diet:
- seafood, including cod and oysters;
- chicken eggs;
- nuts and seeds;
- carrots, apricots, citrus fruits and other orange fruits and vegetables;
- sprouted wheat, spinach and microgreens;
- Blueberries, which are also very good for vision, are rich in vitamin A and antioxidants .
Prevention
Carefully following the doctor's recommendations and attending all scheduled appointments with the rheumatologist and ophthalmologist, your child's vision problems should be under control - the main preventive measures.
It is recommended to visit doctors regularly (every 3–6 months) to ensure that there are no changes in the condition of the optical system.
Prevention is as follows:
- proper hygiene;
- minimizing injury;
- strengthening the immune system with drugs and hardening;
- minimizing exposure to toxic substances.
Consequences and complications
Severe trophic disorders, the action of toxins, epithelial lesions, pupillary fusion, congestion and exudation in the retina can lead to such serious consequences and complications as:
- clouding of the lens or in other words - cataract ;
- secondary glaucoma;
- atrophy of the eyeball;
- neuritis;
- exudative retinal detachment;
- band-shaped corneal degeneration.
How is the diagnosis made?
To diagnose the type of uveitis and possible causes, your doctor will obtain your medical history and ask questions about your general health and possible eye conditions that may be associated with uveitis.
At each subsequent visit, he will check your vision and intraocular pressure. The eye will be examined with a slit lamp and drops will be given to dilate the pupils to make fundus examination easier.
Your doctor may also order additional diagnostic testing, such as OCT (optical coherence tomography), visual field test, or retinal angiography, to evaluate possible complications caused by inflammation, such as cataracts, glaucoma, or retinal edema.
In addition, blood tests and x-rays are performed.