The term “Coronary heart disease” includes a group of diseases:
- myocardial infarction
- atherosclerotic cardiosclerosis
- angina pectoris.
Angina pectoris (synonymous with angina pectoris) is characterized by attacks of sharp chest pain and discomfort in the chest due to lack of blood supply to a certain area of the heart. The severity of the attacks varies, and in rare cases it ends in death. The main cause of the disease is atherosclerosis of the coronary arteries of the heart.
To make an accurate diagnosis, a number of other diseases that may manifest as pain in the heart area should be excluded: spinal osteochondrosis, herpes zoster, diseases of the esophagus and stomach, lung diseases, cardioneurosis, pericarditis.
Types of angina
There are the following types of disease, which depend on the clinical picture:
Angina pectoris
One of the main manifestations of IHD. As a result of a discrepancy between the myocardial need for oxygen and its delivery through arteries narrowed due to atherosclerosis, myocardial ischemia occurs, which is manifested by chest pain or shortness of breath and severe fatigue during exercise.
Stable exertional angina is divided into four functional classes. Functional classes of angina are designed for accurate diagnosis and include a wide variety of clinical information (eg, easy walking on level ground and brisk climbing of stairs).
Variant (spontaneous) angina
Characterized by unpredictable appearance, i.e. pain may also occur at rest. It does not occur as a response of the heart to emotional and physical stress and differs from angina pectoris in that it is usually based on spasm of the coronary arteries of the heart, and not just atherosclerotic damage.
Unstable angina
Requires immediate hospitalization, there is a high probability of developing myocardial infarction.
Reasons for the development of pathology
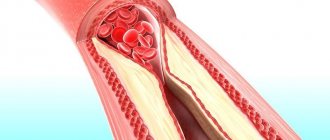
Symptoms of unstable angina develop against the background of a gradual narrowing of the lumen of the coronary arteries. This phenomenon causes necrosis of cardiomyocytes. Lipid deposits on the coronary vessels lead to the formation of atherosclerotic plaques. The patient suffers from decreased blood flow in the coronary arteries.
A significant amount of lipid deposits can cause blood clots. Damaged vessels become overly susceptible to substances released by platelets. This phenomenon provokes further narrowing of the arterial lumen.
Symptoms
Main symptoms include:
- acute chest pain radiating from the left (or right) side to the lower jaw, arm, shoulder blade
- shortness of breath
- feeling of suffocation and lack of air
- feeling of fear, anxiety
- increased pain in the left chest area when trying to take a deep breath
- increased sweating
- tachycardia
- deviation of blood pressure from normal (low or high).
The main factors in the development of the disease that cause symptoms of angina pectoris include
- age (usually after 40 years)
- gender (men develop CHD on average 10 years earlier than women)
- hereditary factor.
An important role in the formation of the disease is played by excess body weight, a history of diseases such as diabetes, arterial hypertension, increased blood clotting, metabolic syndrome, emotional lability, lack of physical activity, smoking and alcoholism.
Angiotensin-converting enzyme inhibitors (ACEIs)
Angiotensin-converting enzyme inhibitors (ACEIs)
–
for angina pectoris,
they are prescribed to prevent the development of heart failure.
Therefore, drug doses are usually lower than for the treatment of hypertension. If after a MI you develop symptoms of heart failure or doctors identify impaired LV function, adding an ACE inhibitor to your therapy will significantly reduce the risk of death and the likelihood of a recurrent MI. The effect of drugs such as ramipril, trandolapril, zofenopril, enalapril has been proven. If these drugs are poorly tolerated, it is possible to replace them with angiotensin receptor antagonists. ACE inhibitors can be prescribed for angina pectoris without a history of heart attack
- their ability to slow the progression of atherosclerosis has been proven. The effect of the drugs ramipril and perindopril has been proven.
Diagnostics
In diagnosing angina, a balanced and competent approach is necessary, because with unstable angina, the patient's condition may worsen until the development of myocardial infarction. Each study must be substantiated.
- ECG
- 24-hour ECG monitoring
- bicycle ergometry or treadmill (stress test with simultaneous ECG recording)
- EchoCG
- stress echocardiography
- coronary angiography
- myocardial scintigraphy
At the EXPERT Clinic, cardiologists are also functional diagnostics doctors. They will weigh all the risks before conducting the examination.
What can the disease be confused with?
As for diseases not related to the cardiovascular system, based on the symptoms and signs, angina pectoris can be mistaken for:
- osteochondrosis of the cervical or thoracic spine;
- vegetative-vascular dystonia;
- gastrointestinal diseases (diaphragmatic hiatal hernia);
- pleurisy, pulmonary embolism;
- pinched nerves.
Usually this disease is confused with the onset of myocardial infarction. The signs are really very similar. The main difference is that an attack of angina is relieved by taking nitroglycerin. In case of a heart attack, the medicine does not work or relieves pain only slightly and temporarily.
Treatment
The goals of treatment are to improve the prognosis (prevent heart attack) and eliminate symptoms of the disease. Non-medicinal (sports, diet), medicinal (tablets and drip infusions) and surgical treatment methods are used.
At the EXPERT Clinic, patients have the opportunity to receive a full consultation with a cardiologist on lifestyle changes and modification of risk factors. If necessary, treatment in a day hospital under the supervision of experienced medical personnel is possible.
Therapeutic measures
Conservative treatment involves prescribing several groups of drugs to the patient. Antianginal drugs relieve symptoms of angina pectoris. In acute attacks accompanied by intense pain, intravenous infusion of painkillers is performed.
Thrombolytics reduce the likelihood of blood clots. A similar goal is pursued when prescribing direct anticoagulants to a patient.
Lipid-lowering drugs remain an integral component in the drug treatment of unstable angina. They help normalize cholesterol levels in the patient’s blood. Constant use of such drugs reduces the likelihood of complications and recurrent attacks.
If conservative treatment is ineffective, the patient is prescribed surgery. The type of surgical intervention is determined by a cardiologist based on coronary angiography data. Imaging will allow us to understand the extent of damage to the coronary arteries. The most common methods of surgical treatment of angina remain coronary bypass surgery and coronary angioplasty.
Recommendations
To prevent angina attacks you must:
- quit smoking
- control cholesterol levels, if necessary, eat a low-fat diet
- perform a dosed and doctor-selected set of physical exercises
- avoid stress
- lead a healthy lifestyle
A balanced diet, dosed physical activity and regular monitoring by a qualified doctor can save a patient with angina pectoris from heart surgery.
Cytoprotectors
Cytoprotectors
– protects against the death of heart muscle cells during episodes of acute and chronic oxygen deprivation (ischemia), allowing the cells to produce energy to pump the heart using less oxygen.
There is an evidence base for the drug trimetazidine (Preductal MV). The drug has no contraindications (except for individual intolerance) and side effects. Partnership between doctor and patient is the key to successful treatment of angina pectoris.
Still have questions? Make an appointment! Using materials from the article by N.S. Veselkova
FAQ
How to avoid angina pectoris?
To avoid angina pectoris, it is necessary to prevent the development of atherosclerosis if possible, because in the vast majority of cases it is the cause of angina. As is known, many factors directly influence the formation of atherosclerotic plaques. Gender, age, heredity are predisposing factors that cannot be changed, but other factors can be controlled and even prevented:
- high blood pressure
- smoking
- high cholesterol
- overweight
- diabetes
- low physical activity
- stress
Changing these factors is in your hands!
Is it possible to completely recover from angina?
Angina pectoris, as a rule, occurs as a result of damage to the coronary arteries supplying blood to the myocardium by atherosclerosis, and this is a chronic incurable process. However, with a properly selected treatment regimen, it is possible to ensure that long-term remission occurs and angina attacks will not bother you. Also, at present, if necessary, it is possible to install a stent into the narrowed lumen of the vessel to restore blood circulation, or MCS/CABG surgery is a surgical intervention that restores the blood flow of the heart below the site of the narrowing of the vessel. In this surgical procedure, another path for blood flow is created around the narrowing site to the part of the heart that is not supplied with blood.
Where does it hurt during an angina attack?
Characteristic of angina is paroxysmal pain behind the sternum, in the center of the chest. The pain is of a compressive, pressing nature, more often associated with physical or psycho-emotional stress and goes away when it stops. The pain may radiate to the left arm, shoulder blade, lower jaw and collarbone. If nitrates are used, the effect on angina is not delayed, it develops immediately, within 1-2 minutes.
Are there ways to cope with an angina attack without medications?
Since many people experience angina attacks during physical activity, sometimes simply stopping the activity (walking, etc.) and resting can lead to the cessation of pain. However, people suffering from angina pectoris should always have nitroglycerin or nitrospray with them in order to relieve an attack of pain within one to two minutes. You should not delay the time before taking nitroglycerin, since pain is a manifestation of myocardial ischemia (insufficient blood supply), and if it persists, then foci of necrosis may occur in the myocardium (myocardial cells may die). If angina attacks become more frequent, you should urgently consult a cardiologist.
What medications will help with an attack of angina?
An attack of angina must be stopped as soon as possible from the moment of its occurrence, because prolonged ischemia will lead to the development of necrosis, i.e. myocardial infarction. If an attack occurs for the first time in your life, call an ambulance. You can take a nitroglycerin tablet on your own or use a nitro spray under the tongue. The effect will occur within 1-2 minutes and does not last long, 10-15 minutes. It is better to take the drug while sitting or lying down, as a short-term decrease in blood pressure, dizziness, headache, tinnitus may occur - these symptoms are safe and are a consequence of the action of nitroglycerin. If pain returns, you can take nitroglycerin again, because it does not accumulate in the body; multiple doses of the drug are possible during the day (up to 6 tablets per day). If your blood pressure is high, you need to lower it to normal levels.
All patients who have suffered an attack of angina pectoris need to have an ECG performed and a decision by a cardiologist on hospitalization.
Why is it necessary to quit smoking? How does smoking worsen angina?
If you smoke and have angina, the best thing you can do to help your heart is to quit smoking!
Studies have shown that the mortality rate in those patients with angina who quit smoking decreased by 2 times compared to those who continued to smoke. Why? Angina is based on a lack of oxygen in the heart muscle, and smoking increases the level of carbon dioxide in the blood, and it displaces oxygen in the blood. This leads to oxygen starvation of the heart muscle. Smoking also increases blood viscosity. Smoking increases the frequency and aggravation of angina attacks and greatly increases the risk of myocardial infarction. Quitting smoking eliminates the adverse effects of nicotine on the coronary arteries, and angina attacks disappear or become less frequent.
Important: replacing cigarettes with cigars and pipe tobacco, switching to cigarettes with less tar and nicotine do not reduce cardiovascular risk!
Contrary to popular belief, abruptly quitting smoking is not harmful; overcoming this bad habit has an undeniable positive effect, regardless of smoking experience.
You need to be prepared for the fact that sometimes depression and irritability occur when quitting smoking, in which case you can seek help from a psychotherapist.
I suffer from angina pectoris, but I dream of losing excess weight. What physical activities are acceptable for people with such problems?
For people suffering from angina, 30–45 minutes of physical activity per day is recommended. The best choice is walking (preferably at a brisk pace) or Nordic walking with ski poles, cycling, swimming. It is important that the exercises do not cause pain, palpitations, or shortness of breath. When practicing swimming or water aerobics, you should remember that cold water can provoke angina attacks, so the water temperature in the pool should be comfortable for you. It is better to do water aerobics under the supervision of a trainer and according to a program specially adapted for people with cardiac problems. In this case, the loads should increase very gradually. However, to lose weight, you need not only physical activity, but also proper nutrition; a nutritionist will help you choose the right menu during your consultation.
Can you have angina if there is no pain?
Unfortunately yes. For example, with diabetes mellitus, diabetic polyneuropathy develops, and the patient may not feel pain, this is the so-called silent ischemia. This condition is dangerous because the patient does not take action in time, and myocardial infarction will develop. In some cases, shortness of breath during exercise can be considered equivalent to pain, so you can suspect the presence of angina pectoris and come for examination to a cardiologist.
How does the disease develop?
It is at such moments that common signs of angina pectoris appear in women and men: you feel a lack of air, arrhythmia. At this time, chemical changes occur in the myocardium associated with metabolic disorders, a decrease in the synthesis of substances, and the accumulation of acids. The functions of the myocardium are gradually disrupted, and its metabolism changes.
What causes this disease? There are certain factors:
- high cholesterol levels;
- obesity when consuming excessive amounts of fats and carbohydrates;
- physical inactivity disrupts lipid volume;
- smoking causes oxygen starvation of cells and arterial spasm;
- arterial hypertension causes myocardial tension;
- anemia, intoxication contribute to oxygen starvation;
- diabetes mellitus increases the risk of ischemia;
- increased blood viscosity is a direct risk of blood clots;
- psycho-emotional stress (especially in women) worsens myocardial nutrition.
Treatment history
Case No. 1
Kirill, 57 years old. Experienced smoker, hypertensive (“working” pressure 150/95 mmHg). Five years ago, according to the patient, he had problems with his heart and blood pressure, was examined, took prescribed medications for six months, then stopped taking them on his own. During the visit to the clinic, attacks of chest pain appeared during physical activity, which went away when the exercise stopped. At the doctor’s appointment, blood pressure is 170/100 mmHg, rapid pulse is 90 beats per minute. The patient was examined - an increase in the level of “bad” cholesterol was detected, ECG and ultrasound of the heart without signs of ischemia, and ischemia was recorded on the 24-hour ECG monitor at the time of significant physical activity, i.e. there is angina pectoris. The patient was given a treatment regimen for angina pectoris, which resulted in normalization of blood pressure and cholesterol levels within 3 months, and a significant increase in exercise tolerance. With the help of a psychotherapist, the patient decided to quit smoking and took up Nordic walking with a gradual increase in loads under the supervision of a cardiologist. Over the past year, angina attacks have not bothered me. It is recommended to continue taking medications and undergo regular preventive examinations.
Thanks to cooperation with doctors and the desire to feel better, the patient was able to change his lifestyle, prevent complications of the disease and prolong his life for many years.
Calcium agonists
Calcium agonists - are able to dilate the blood vessels of the heart, increasing the flow of blood to the heart muscle (myocardium), thereby reducing the number of angina attacks
.
They are divided into three main groups with characteristic features. Drugs from the group of dihydropyridine calcium antagonists
(nifedipine) can be prescribed together with beta blockers, or instead of beta blockers (if intolerance or contraindications to the latter).
The first generations (nifedipine) increase the heart rate, so short-acting tablets (nifedipine 10 mg) are prohibited for angina pectoris. There are special prolonged forms (osmo-adalat, corinfar-retard, nifecard) containing from 20 to 60 mg of nifedipine. The third generation of drugs (amlodipine, felodipine) practically does not increase the pulse rate and is taken once a day. Drugs from the verapamil and diltiazem group
reduce the heart rate; combined use with beta blockers is contraindicated due to the risk of bradycardia and other complications. It has been proven that regular use of calcium antagonists can reduce the incidence of strokes.