Classification of ventricular extrasystoles
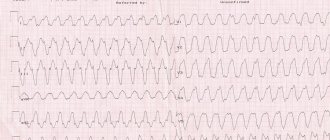
Under certain circumstances, ventricular extrasystole causes a severe form of arrhythmia - ventricular tachycardia, which turns into fibrillation. And this condition is the most common cause of sudden coronary death.
Lown classification
The classification of PVCs has changed several times following diagnostic and prognostic needs. Extrasystoles in them were distributed according to quantitative values, location and frequency of occurrence. For about 15 years in cardiology they used the classification of ventricular extrasystoles according to Lown and Wolf (B. Lown and M. Wolf). They proposed it for the gradation of gastric extrasystoles in post-infarction patients. A few years later, it was adapted for patients without a history of heart attack.
This classification reflects the quantitative and morphological signs of PVCs (based on the results of a 24-hour ECG):
| Class | Characteristics of ventricular extrasystole |
| Extraordinary layoffs are not recorded | |
| 1 | Less than 30 single extrasystoles in any 60 minutes during the day |
| 2 | More than 30 single extrasystoles during any hour of monitoring |
| 3 | There are (polymorphic) extraordinary contractions occurring in different foci of excitation |
| 4A | There are two extrasystoles in a row emanating from one focus of excitation (monomorphic) |
| 4B | There are paired polymorphic extrasystoles |
| 5 | There are polymorphic PVCs passing in one gulp of 3–5, registration of paroxysmal ventricular tachycardia is possible |
According to Lown's classification, class 1 is a benign condition, rather considered as a functional disorder without circulatory impairment and clinical signs. Starting from class 2, ventricular extrasystole has a poor prognosis, being associated with an increased risk of developing fibrillation and cardiac arrest.
Gradation of extrasystoles by location, time and frequency of occurrence
There is a classification of ventricular extrasystole according to the place of origin of impulses and the number of foci of excitation:
- extrasystoles emanating from one focus are called monotopic;
- PVCs that originate in several foci are polytopic;
- right ventricular extrasystole;
- left ventricular extrasystole.
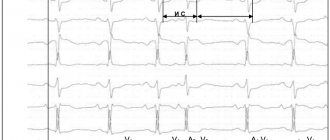
According to the time of occurrence, ventricular extrasystoles are divided into early (recorded at the beginning of diastole), interpolated, appearing in the middle between two beats, and late, occurring at the very end of diastole. Early extraordinary contractions according to the ECG sign are called “R on T” (layering of two teeth on top of each other). They are caused by organic changes in the myocardium. According to Lown, this type of ventricular extrasystole is classified as class 5.
In cardiology, there is a concept of a statistical daily “norm” of VES if they are well tolerated. There is no such norm for early extrasystole - it should not exist at all. Average or interpolated is the majority of the VES (up to 80%). Its average normal indicator is considered to be up to 200 extraordinary contractions per day. Late extrasystoles almost overlap the subsequent normal contraction. Their permissible daily quantity is up to 700. Today, the medical community uses the RJ Myerburg classification, which reflects the shape and frequency of ventricular extrasystoles:
| By frequency | According to morphology | ||
| 1 | less than 1 in 60 minutes - rare; | A | Single from one source |
| 2 | 1–9 per hour - infrequent; | B | Single from different foci |
| 3 | 10–30 per hour – moderately frequent; | C | Doubles |
| 4 | 31–60 per hour - frequent; | D | Unsustained ventricular tachycardia |
| 5 | more than 60 per hour - very frequent. | E | Sustained ventricular tachycardia |
Prevention of heart rhythm disturbances
The basic rules of prevention are:
- Therapy of concomitant pathologies of the cardiovascular, circulatory, endocrine and nervous systems.
- Do not self-medicate and do not take strong tranquilizers, hormones, or sedatives.
- Conduct control diagnostics in a timely manner.
The disease of extrasystole is characterized by relapses, therefore, after completing the course of therapy, you should regularly undergo control diagnostics of the heart rhythm.
This article is posted for educational purposes only and does not constitute scientific material or professional medical advice.
Examples of diagnosis formulation:
WPW syndrome, frequent paroxysms of supraventricular tachycardia (up to 2-3 times a month).
DCM, complete block of the left bundle branch, frequent polytopic ventricular extrasystoles, CHF II B, FC III. Cardiac asthma.
- Single polymorphic ventricular extrasystole
3. IHD: exertional angina, FC III. Post-infarction cardiosclerosis (with Q wave, infarction, date, localization). SSSU corrected with a pacemaker (date). CHF II A, cardiac asthma.
Background: Stage III hypertension, stage 2 hypertension, risk 4.
4. IHD: progressive angina. PIX (date, location), aneurysm of the anterior wall of the left ventricle. Incomplete AV block II degree (Mobitz II), CHF III, FC IV.
General information
The factors that caused the development of the disease can be of physiological and pathological origin. An increase in the tone of the sympathetic-adrenal system leads to an increase in the occurrence of extrasystoles. Physiological factors influencing this tone include the consumption of coffee, tea, alcohol, stress and nicotine addiction. There are a number of diseases that lead to the formation of extrasystole:
- cardiac ischemia;
- myocarditis;
- cardiomyopathy;
- heart failure;
- pericarditis;
- hypertonic disease;
- osteochondrosis of the cervical spine;
- prolapse of the mitral valve leaflets;
- cardiopsychoneurosis.
There is a certain connection between the patient’s age, time of day and the frequency of extrasystoles. Thus, more often the ventricular type is present in people over 45 years of age. Dependence on circadian biorhythms is manifested in the registration of extraordinary heart contractions, more in the morning hours.
Ventricular extrasystole threatens the patient’s life. Its formation increases the risk of sudden cardiac arrest or ventricular fibrillation.
Diagnosis of extrasystole
A preliminary diagnosis of “extrasystole” is made by a specialist based on an initial examination and collection of an anamnesis of the disease: genetic predispositions, already diagnosed pathologies and patient complaints.
To confirm the diagnosis and select a therapeutic regimen, the patient is prescribed:
- ECG
. - Bicycle ergometry
. - Load test.
- ECG-Holter (24-hour monitoring)
. - Ultrasound of the heart
(if necessary). - MRI (if necessary).
Based on the diagnostics performed, the cardiologist clearly sees the foci of occurrence and the type of extrasystoles (atrioventricular, ventricular or atrial).
Reasons for development
Irregularities and heart diseases are the main reasons why PVCs develop. Also, ventricular arrhythmia can be triggered by heavy physical work, chronic stress and other negative effects on the body.
From cardiac pathologies:
| Heart failure | Negative changes in the muscle tissue of the heart muscle, leading to disruption of the inflow and outflow of blood. This is fraught with insufficient blood supply to organs and tissues, which subsequently causes oxygen starvation, acidosis and other metabolic changes. |
| Coronary heart disease (CHD) | This is damage to the heart muscle due to impaired coronary circulation. IHD can be acute (myocardial infarction) or chronic (with periodic attacks of angina). |
| Cardiomyopathy | Primary myocardial damage, leading to heart failure, atypical beats and heart enlargement. |
| Heart disease | Defect in the structure of the heart and/or major outflow vessels. Heart disease can be congenital or acquired. |
| Myocarditis | An inflammatory process in the heart muscle that disrupts impulse conduction, excitability and contractility of the myocardium. |
Taking certain medications (incorrect dosage, self-medication) can also affect the functioning of the heart:
- Ventricular extrasystole
| Diuretics | Medicines in this group increase the rate of urine production and excretion. This can provoke excessive excretion of the “heart” element - potassium, which is involved in the formation of the impulse. |
| Cardiac glycosides | The drugs are widely used in cardiology (they lead to a decrease in heart rate and an increase in the force of myocardial contraction), but in some cases they cause side effects in the form of arrhythmia, tachycardia, atrial fibrillation and ventricular fibrillation. |
| Drugs used for heart blocks (M-anticholinergics, sympathomimetics) | The side effects of the drugs manifest themselves in the form of stimulation of the central nervous system, increased blood pressure, which directly affects heart rhythm. |
Also, the development of PVCs can be affected by other pathologies not associated with disruption of the cardiovascular system:
- Diabetes mellitus type 2 . One of the serious complications of the disease associated with carbohydrate imbalance is diabetic autonomic neuropathy, which affects nerve fibers. In the future, this leads to a change in the functioning of the heart, which “automatically” causes arrhythmia.
- Hyperfunction of the thyroid gland (moderate and severe thyrotoxicosis). In medicine, there is such a concept as “thyrotoxic heart,” which is characterized as a complex of cardiac disorders - hyperfunction, cardiosclerosis, heart failure, extrasystole.
- In diseases of the adrenal glands, there is an increased production of aldosterone, which in turn leads to hypertension and metabolic disorders, which is interconnected with the work of the myocardium.
Ventricular extrasystole is not of an organic nature (when there are no concomitant cardiac diseases), caused by a provoking factor, often has a functional form. If you remove the negative aspect, then in many cases the rhythm returns to normal.
Functional factors of ventricular extrasystole:
- Electrolyte imbalance (reduction or excess of potassium, calcium and sodium in the blood). The main reasons for the development of the condition are changes in urination (rapid production or vice versa, urinary retention), malnutrition, post-traumatic and postoperative conditions, liver damage, and surgery on the small intestine.
- Substance abuse (smoking, alcohol and drug addiction). This leads to tachycardia, changes in material metabolism and disruption of myocardial nutrition.
- Disorders of the autonomic nervous system due to somatotrophic changes (neuroses, psychoses, panic attacks) and damage to subcortical structures (occurs with brain injuries and pathologies of the central nervous system). This directly affects the functioning of the heart and also provokes surges in blood pressure.
Ventricular extrasystoles disrupt the entire heart rhythm. Pathological impulses over time have a negative effect on the myocardium and the body as a whole.
Why do extrasystoles occur during VSD?
Cardiac “dancing” in vegetative-vascular dystonia can occur when both parts of the autonomic nervous system are disrupted.
If the sympathetic department fails, extrasystoles appear after physical exertion. They are poorly controlled by sedatives, and may even intensify after taking them.
If the functioning of the parasympathetic system is disrupted, in addition to cardiac symptoms, digestive disorders are of concern: epigastric pain, diarrhea, bloating. A cup of coffee or sweet tea or a brisk walk will help relieve such an attack.
If the cause is psychological, treatment measures are directed in the other direction.
Most often, dystonics are bothered by two types of extrasystole:
- Ventricular. Usually makes itself felt in the first half of the day. It is caused by disturbances in mental balance, for example, great joy or grief. It also appears when the weather changes or when drinking strong drinks. Other provoking factors include magnesium and calcium deficiency, osteochondrosis. It all starts with an intense beat in the heart area, followed by a pause. The patient becomes covered in cold, sticky sweat and develops a feeling of fear. Despair sets in, he cannot choose a comfortable position for himself, becomes numb or begins to fuss. The violence of his heart leads him into an uncontrollable state, causing him a lot of suffering.
- Supraventricular. The most common type of arrhythmia in VSD. The causes of this condition coincide with those of the ventricular form. In addition, dystonics who are addicted to antiarrhythmic and diuretic drugs are at risk. Patients claim that the condition worsens when lying down. It is this sign that indicates that the cardiac failure is functional in nature.