Norms for TSH
It is important to remember that TSH fluctuations are especially individual for each person at different ages.
Therefore, an accurate interpretation of TSH tests (resolving the issue of whether TSH is low or increased) should only be carried out by a medical specialist. On average, the norm for TSH levels in adults is 0.23-4.90 mIU/l. For children aged 7-12 years, the TSH norm, on average, is in the range of 0.61-5.20 mU/l. For children under 6 years of age, the TSH norm ranges from 0.45-3.6 mU/l.
The average value and norm of TSH during pregnancy is 0.2-3.5 mU/l. In pregnant women, during some periods, it is considered normal when the TSH level is elevated to 5.6 mU/L.
Diagnostics
An increase in TSH is detected by a blood test. Along with this parameter, it is advisable to immediately determine the level of free T3 and T4. This will help you make the correct diagnosis and choose treatment.
A pituitary adenoma is detected on an MRI of the brain. This study is referred if laboratory data did not help to identify the cause of the condition.
A high TSH level in the analysis is not always an indicator of the presence of pathology. It rises after heavy physical activity, so it should be avoided for at least a day before the test. After removal of the gallbladder and hemodialysis, the results may also be distorted. If the attending physician knows about this, he will take all the circumstances into account when deciphering the test results.
The level of TSH in the blood fluctuates depending on the time of day. The maximum level is observed from 2 to 4 am, and the minimum - at 17-18 hours.
Read also: Hypothyroidism: causes, symptoms, treatment
Why is TSH low?
A decrease in TSH concentration in the blood may indicate:
• Deterioration of the pituitary gland function – after brain injuries, with hereditary diseases, infections, after severe bleeding;
• Hypothyroidism is a deterioration in the normal functioning and function of the thyroid gland, which may be associated with a tumor, iodine deficiency, protein deficiency, heredity, exposure to radiation and other reasons;
• Psychological stress;
• Abuse of thyroid hormones;
• Sheehan syndrome – partial death of cells in the pituitary gland in women after childbirth.
Causes
TSH is not produced by the thyroid gland, as the name suggests, but by the pituitary gland. This is a gland located in the brain. When high TSH is detected in women, there can be only two reasons: the pituitary gland produces it on its own or in response to a deficiency in the blood of thyroid hormones - thyroxine (T4) and triiodothyronine (T3).
Most often, excess TSH occurs in response to a lack of T4 and T3. But in some cases, the pituitary gland produces it in large quantities due to the growth of the gland itself. The more cells there are, the more TSH is synthesized.
When is a TSH test needed?
An analysis to determine TSH norms is needed in the following cases:
• Suspicion of hypofunction of the thyroid gland - lethargy, drowsiness, dry skin, constipation, chilliness, etc. An examination can help understand the cause of decreased function (to distinguish pathology of the thyroid gland from pathology of the pituitary gland);
• Suspicion of hyperfunction of the thyroid gland – a feeling of arrhythmia and tachycardia, diarrhea, nervousness, insomnia, menstrual irregularities, feeling of heat, weight loss, protrusion of the eyeballs from the orbits, etc.;
• Monitoring the results of treatment after removal of the thyroid gland (partial or complete);
• Monitoring the results of hormone replacement therapy for glandular diseases;
• Autoimmune diseases of the thyroid gland and control of their treatment;
• Diagnosis of suspected congenital hypothyroidism in a newborn.
Treatment
Therapy depends on the type of disease. Hypothyroidism is treated with replacement therapy with synthetic analogues of T3 and T4. The dosage is selected individually for each patient based on test results.
Pituitary adenoma is treated in three ways: first, the doctor prescribes hormone replacement therapy. If it is ineffective and the tumor progresses, radiation therapy is performed. If there is no positive dynamics, the tumor is removed surgically.
If high TSH in women is not corrected, the consequences will depend on the cause that caused the condition. Due to hypothyroidism, myxedematous coma can develop, which can lead to death. Against the background of hyperthyroidism, a hyperthyroid crisis may occur. It is also deadly to humans.
Even small fluctuations in TSH can lead to dangerous consequences for a woman. Impaired thyroid function leads to disruption of the menstrual cycle, which can cause infertility.
If pregnancy occurs in a woman with thyroid pathologies who are not treated, the child may develop cretinism. This can be successfully prevented by taking hormone replacement therapy or hormone-correcting medications.
Dear patients! Remember that only a qualified doctor can make an accurate diagnosis, determine the causes and nature of the disease, and prescribe effective treatment. You can make an appointment with our specialists or call a doctor at home by calling 8-(4822)-33-00-33
Be healthy and happy!
How often do you need to get tested for TSH, who and where?
TSH analysis is especially important for children and women when planning pregnancy, as well as during it. Any suspicion of hormonal disorders associated with the thyroid gland requires testing using hormone tests, including TSH.
It is imperative to monitor TSH for those who have already had problems with the thyroid gland before. According to the recommendation of the American College of Physicians, TSH testing should be done regularly for all women over 50 years of age, since this is a risk group for hormonal disorders due to the onset of hormonal changes in the body (entry into menopause).
You can get tested for TSH in almost any clinic or laboratory. However, only at LAB4U the affordable price of a TSH blood test is combined with high quality and accurate results.
Possible diseases
The growth of pituitary tissue is possible due to a tumor - adenoma. This is one of the rarest causes of elevated TSH levels in the blood.
The most common causes of elevated TSH:
- hypothyroidism - a lack of thyroid hormones, in response to which the pituitary gland produces more TSH;
- thyroiditis is an inflammation of the thyroid gland, including autoimmune inflammation, to which the pituitary gland reacts.
Diagnosis requires a large-scale examination, since without finding out the cause it is impossible to select a treatment.
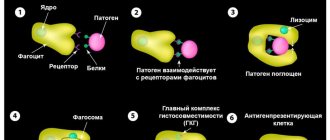
Functions of thyroid-stimulating hormone in the female body
The first thing that elevated TSH means is a low concentration of triiodothyronine and thyroxine in the bloodstream. The role of thyroid-stimulating hormone is to ensure an increase in the production of T4 by the gland, which is achieved through its effect on receptors that are located on the membrane of the follicular cells of the thyroid gland. The result of this effect is an increase in iodine consumption by thyrocytes (thyroid cells), which trigger the process of synthesis and secretion of the most important regulators of differentiation of tissues, organs and systems - the hormone T4 (about 80%) and the more powerful T3 (about 20%). The effect appears within 1-2 minutes. Regulation of the biosynthesis of thyroid hormones is the main, but not the only task of thyroid-stimulating hormone.
In a woman’s body, it is also responsible for:
- quantitative change in phospholipids, nucleic acids;
- lipolytic effect (lipolysis) – enhances the breakdown of fat molecules into glycerol and fatty acids;
- production of proteins, support of energy balance;
- maintaining the normal structure of the thyroid gland (when TSH is increased, the size of the woman’s thyroid gland also changes - tissue growth, an increase in volume and a change in the contours of the thyroid gland are observed, which can be identified visually or determined by touch);
- an increase in the number and size of hormone-producing cells;
- sensitivity of hormonal receptors - prepares tissues for the action of triiodothyronine and thyroxine.
Why is an increase in TSH dangerous?
An increase in thyrotropin secretion is observed relatively rarely; it manifests itself as hypothyroidism or thyrotoxicosis. Symptoms usually progress quickly. High concentrations of thyrotropin in women often cause infertility, difficulties with conception, spontaneous abortion in the early stages, severe toxicosis, bleeding, fetal hypoxia, developmental delay and even fetal death. The consequence of high TSH can also be problems with the heart, vision, mucous edema, thyrotoxic crisis, atherosclerosis, and disruptions in the functioning of the central nervous system. Without medical care, a woman's quality of life can seriously deteriorate.
With timely, competent treatment and strict adherence to all medical recommendations, the prognosis is generally favorable.
Causes of increased thyroid-stimulating hormone
Changes in the direction of increasing TSH levels may be associated with:
- with a benign neoplasm in the pituitary gland – thyrotropinoma;
- adenoma in the anterior pituitary gland;
- syndrome of resistance to hormonal elements of the thyroid gland;
- irregular production of thyrotropin;
- juvenile hypothyroidism, other formations in the pituitary gland;
- subacute thyroiditis;
- chronic pathologies, including mental illnesses;
- removal of the gallbladder, lead intoxication;
- excessive physical activity, hemodialysis procedures;
- preeclampsia.
The element may increase during therapy with certain medications:
- anticonvulsant action - during treatment with Benserazide, Phenytoin;
- beta blockers - Atenolol, Metaprolol;
- Morphine, Prednisone, Rimphapicin.
A similar deviation occurs during therapeutic procedures using iodides and Calcitonin.
Donating blood for TSH hormone
This is a laboratory test. Conducted in standard mode. It involves examining biomaterial taken from the patient using specialized equipment. Each medical laboratory has its own methodology, equipment, reagents, rating scales, which causes some discrepancies in measurement results. This is important to consider when visiting different clinics.
Repeated annual checks are recommended to be done in the same institution and at the same time, because daily and seasonal fluctuations in thyrotropin levels are possible. Its concentration in the blood can be determined as part of a separate study or as part of a set of tests. In laboratory diagnostics, chemiluminescent immunoassay is used to determine TSH.
Material for research
The biomaterial is blood serum. Hemolysis and lipemia may affect the test result. A woman's blood sample is obtained from a vein (forearm, cubital fossa). When drawing blood, the patient sits or lies. Venous blood collection is the simplest invasive procedure. The laboratory technician treats the injection site with a disinfectant. A tourniquet is applied to restrict blood circulation.
How do you prepare for the procedure?
It is advisable to collect blood in the morning.
Preparatory activities include:
- Exception on the eve of the examination of physical procedures and other methods of examination - X-ray, X-ray fluorography, ultrasound.
- Refusal to use hormone-containing drugs (7 days before) and medications containing iodine (3 days before). The exact timing of abstinence and the names of medications must be agreed upon with your doctor in advance.
- Avoiding alcohol consumption, stressful situations, overheating, hypothermia, minimizing emotional stress, physical activity (1 day).
- Limiting fatty foods, fried foods, not exercising (1 day).
- Elimination of any food before the session, pure non-carbonated water is allowed (the procedure is carried out on an empty stomach).
- Abstinence from smoking, keeping calm (1 hour).
Period of execution
The urgency of the analysis depends on the specific laboratory and its capabilities. After collecting the material, the study can be carried out independently or samples can be sent for analysis to another institution. In most cases, the result in the form of a special table on a laboratory form (indicating reference values) can be obtained on the same or the next day. By agreement with the contractor, the result can be sent by email.
How to decrypt
Specialists from a medical institution help to correctly interpret the final result, but for a more accurate interpretation, you will need to consult with the attending physician, who has all the necessary information about the internal picture of the disease, the woman’s health status, her physiological characteristics, and the presence of concomitant diseases.
Thyrotoxicosis (hyperthyroidism) - symptoms and treatment
In the treatment of thyrotoxicosis, the following basic methods are usually used:
- conservative drug treatment with thyreostatic drugs;
- radioactive iodine therapy (I 131);
- surgery;
- non-drug treatment (limiting physical activity, healthy sleep, quitting smoking, preventing stress).[5][11][12]
The fight against the syndrome involves eliminating the clinical manifestations of thyrotoxicosis with normalization of T3, T4 and TSH values and achieving stable remission of the disease.
Conservative therapy
In the conservative treatment of diffuse toxic goiter in patients with a moderately enlarged thyroid gland (up to 40 ml), propylthiouracil (PTU) or thiamazole (Tirozol or Mercazolil) is prescribed. This helps to achieve normal functioning of the affected organ. In case of diagnosed cases of diffuse toxic goiter in the first trimester of pregnancy and the occurrence of side effects while taking thiamazole, PTU is prescribed. As a result of treatment, after 4-6 weeks there is an improvement - the level of free T4 is normalized. Additionally, beta-blockers are prescribed according to indications (for example, 2.5-5 mg of Concor per day).
In severe cases, it is recommended to take glucocorticoids - up to 10-15 mg of prednisolone per day. Then, over 2-3 weeks, the dose of the thyreostatic agent is reduced to a maintenance dose (no more than 10 mg per day). In parallel, the patient is usually prescribed 50 mcg of levothyroxine per day. This treatment regimen is called “Block and Replace.”[3][6][7][10][12] Stable maintenance of normal levels of free T4 and TSH will indicate the adequacy of the prescribed therapy.
If there are persistent side effects of the prescribed treatment, thyreostatic drugs are canceled, radioactive iodine therapy or surgery is prescribed. In case of relapse of thyrotoxicosis, the question arises about the need for radioiodine therapy or thyroidectomy - complete or partial removal of the thyroid gland.[5][12]
Treatment with radioactive iodine
Radioiodine therapy for diffuse toxic goiter is carried out in case of persistent relapse of thyrotoxicosis after the end of properly administered conservative therapy (for 12-18 months) and difficulties in taking thyreostatic drugs (decrease in the number of leukocytes in the blood or the occurrence of allergic reactions).
Treatment with radioactive iodine is carried out in specialized centers with radiation and environmental safety for people and nature. The only contraindications for this therapy are pregnancy and breastfeeding.
The goal of radioiodine therapy in destroying hyperfunctioning thyroid tissue is to achieve a stable hypothyroid state.[3][6][7][10][12]
Surgical treatment
Surgical intervention for diffuse toxic goiter is necessary if the goiter is located behind the sternum, with diffuse and nodular forms of goiter with compression and the patient refuses other methods of therapy. Total and subtotal thyroidectomy are the treatment of choice. If there is a nodular formation in the thyroid gland, it is necessary to perform a puncture biopsy and diagnostic cytological examination.[4][5][12]
After the operation, levothyroxine preparations (Euthyrox, L-thyroxine) are prescribed at the rate of 1.7 mcg per kg of the patient’s weight. TSH determination is carried out 6-8 weeks after surgical treatment and over time.
Treatment of diffuse toxic goiter with concomitant endocrine ophthalmopathy is preferably carried out using the “Block and Replace” scheme.[5][10][12]
In the case of thyrotoxicosis with a TSH-secreting pituitary tumor (thyrotropinoma), the TSH level is diagnosed taking into account the levels of free T3 and T4, as well as MRI (as a result, a pituitary adenoma is usually detected). Such patients require surgical intervention.[3][6][7][10][12]
What is TSH in a blood test?
TSH, in its chemical structure, is a representative of the family of glycoprotein hormones and belongs to the group of protein-peptide compounds. For its role in the body it is called regulating. Synthesized by the pituitary gland. Its full name is thyroid-stimulating hormone. Synonyms thyrotropin, thyrotropin are also used. Stimulates the thyroid gland. Determines the content of the main thyroid hormones in the blood: thyroxine (T4), converted into a more active form - triiodothyronine (T3).
In the functioning of the pituitary gland, there is a phenomenon of interaction between TSH, T4, T3, and the feedback principle operates. It is expressed as follows: if the level of T4 decreases even slightly, the pituitary gland immediately reacts to this with a multiple increase in TSH in the blood. It, in turn, activates the thyroid gland, causing it to increase the production of vital thyroxine.
If the thyroid gland releases a lot of thyroxine, and its concentration exceeds the norm, then the excess is suppressed by inhibiting the release of TSH. Suppression of synthesis is carried out by the action of the isolated thyrotropin on the anterior lobe of the pituitary gland.
Based on this interconnected production mechanism, based on the level of thyroid-stimulating hormone in a blood test, diagnosticians and endocrinology specialists:
- judge the functional activity of the thyroid gland;
- study the production of hormones, the body’s needs for thyroxine;
- assess the quality of compensation for the condition caused by persistent hormone deficiency (primary hypothyroidism);
- determine the hormonal background of a woman - without TSH, a diagnostic examination for hormones will not be complete;
- develop diagnostic and treatment tactics;
- monitor the effectiveness of treatment