Ursodesoxycholic acid
Inside. Children and adults weighing less than 34 kg are recommended to use the drug in the form of a suspension.
Dissolution of cholesterol gallstones:
The recommended dose is 10 mg/kg/day, which corresponds to:
| Body weight, kg | Number of capsules, pcs. |
| up to 60 | 2 |
| 61-80 | 3 |
| 81-100 | 4 |
| Over 100 | 5 |
The drug must be taken daily in the evening, before bed (the capsules are not chewed), with a small amount of liquid. Duration of treatment is 6-12 months. To prevent recurrent cholelithiasis, it is recommended to take the drug for several months after the stones have dissolved.
Treatment of biliary reflux gastritis:
1 capsule of the drug daily in the evening, before bed (the capsules are not chewed), with a small amount of water. The course of treatment is from 10-14 days to 6 months, if necessary - up to 2 years.
Symptomatic treatment of primary biliary cirrhosis:
The daily dose depends on body weight and ranges from 3 to 7 capsules (approximately 14±2 mg/kg ursodeoxycholic acid per 1 kg of body weight).
In the first 3 months of treatment, the use of the 250 mg capsule should be divided into several doses throughout the day. After improvement of liver parameters, the daily dose of the drug can be taken 1 time in the evening.
The following mode of application is recommended:
250 mg capsules
| Body weight, kg | Daily dose (capsules, pcs.) | In the morning | During the day | In the evening |
| 47-62 | 3 | 1 | 1 | 1 |
| 63-78 | 4 | 1 | 1 | 1 |
| 79-93 | 5 | 1 | 2 | 2 |
| 94-109 | 6 | 2 | 2 | 2 |
| Over 109 | 7 | 2 | 2 | 3 |
Capsules should be taken regularly, without chewing, with a small amount of liquid.
The use of the drug for the treatment of primary biliary cirrhosis can be continued indefinitely. In patients with primary biliary cirrhosis, in rare cases, clinical symptoms may worsen at the beginning of treatment, for example, itching may become more frequent. In this case, treatment should be continued, taking 1 capsule daily, then the dosage should be gradually increased (increasing the daily dose by 1 capsule weekly) until the recommended dosage regimen is achieved again.
Primary sclerosing cholangitis:
12-15 mg/kg/day (up to 20 mg) for 6-24 months (up to several years).
Cystic fibrosis:
Up to 20-30 mg/kg/day for 6-24 months or more.
Chronic hepatitis of various origins, non-alcoholic steatohepatitis, alcoholic liver disease:
The daily dose is 12-15 mg/kg (2-5 capsules in 2-3 doses, duration of therapy is 6-12 months or more).
Biliary dyskinesia
:
The average daily dose is 10 mg/kg in 2 divided doses for 2 weeks to 2 months.
Children over 3 years old
the drug is prescribed individually, based on the calculation of 20 mg/kg/day.
Deoxycholic acid
Deoxycholic acid
(eng.
deoxycholic acid
, or
deoxycholate
, or
cholanoic acid
, or
3α,12α-dihydroxy-5β-cholan-24-oic acid
) - bile acid, belonging to the so-called
secondary acids
, formed from primary bile acids in the colon under the influence intestinal microflora. The gross formula is C24H40O4. Molecular weight 392.57 g/mol. Deoxycholic acid will dissolve in alcohol and acetic acid. In its pure form it appears as a white or off-white crystalline powder.
Deoxycholic acid in the enterohepatic circulation of bile acids
Deoxycholic acid is formed from a conjugate of the primary bile acid - cholic, which enters the intestines of healthy people from the gallbladder, under the influence of anaerobic bacteria of the colon, where it is deconjugated by microbial choleglycine hydrolase and dehydroxylated with the participation of 7-alpha dehydroxylase.
The resulting deoxycholic acid binds to dietary fiber and is excreted from the body. Acidity in the intestinal lumen is of great importance. When the pH value increases, deoxycholic acid is ionized and well absorbed in the colon, and when it decreases, it is excreted. An increase in pH values in the colon leads to an increase in the activity of enzymes leading to the synthesis of deoxycholic acid, its solubility and absorption and, as a result, an increase in the level of bile acids, cholesterol and triglycerides in the blood. One of the reasons for the increase in pH may be the lack of prebiotic components in the diet, which disrupt the growth of normal microflora, including bifidobacteria and lactobacilli (Lyalyukova E.A., Livzan M.A.). Part of the total volume of deoxycholic acid absorbed in the intestine returns through the portal vein with the blood to the liver (this process is called enterohepatic circulation of bile acids). In hepatocytes, deoxycholic acid is conjugated, binds with glycine or taurine, turning into glycodeoxycholic or taurodeoxycholic acid, and circulates further in the human body along with primary bile acids.
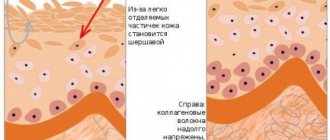
The damaging effect of deoxycholic acid on the mucous membrane
It is assumed that deoxycholic and other bile acids can penetrate the cells of the mucous membrane, being in a non-ionized lipophilic form, thereby causing a damaging effect.
This process is acid-dependent and more pronounced at acidic pH values. When studying the composition of duodenogastroesophageal reflux in patients with erosive esophagitis and Barrett's esophagus, it turned out that with a predominance of cholic, taurocholic and glycocholic acids, there was a significant amount of deoxycholic and taurodeoxycholic acid. In terms of toxicity (and hydrophobic properties), deoxycholic acid is superior to cholic, ursodeoxycholic and chenodeoxycholic acids, but inferior to lithocholic acid.
To reduce the damaging effects of deoxycholic acid on the mucous membrane of the stomach and esophagus, ursodeoxycholic acid preparations are prescribed. Ursodeoxycholic acid is a competitive inhibitor of deoxycholic and other bile acids at all levels of their physiological action: molecular, cellular, tissue and systemic. Due to the significant displacement of hydrophobic deoxycholic and other bile acids from the enterohepatic circulation, ursodeoxycholic acid reduces their potential toxicity to hepatocytes, the epithelium of bile canaliculi, the mucous membrane of the esophagus and stomach, increases the fluidity and reduces the lithogenicity of bile.
Deoxycholic acid as a non-surgical treatment for double chin
At the end of April 2015, the FDA registered the injectable prescription (Rx) drug Kybella, working name ATX-101, developed by Kythera Biopharmaceuticals (USA), the active ingredient of which is synthetic deoxycholic acid. Kybella is approved for use in adult patients to improve the appearance of moderate to severe thickening or enlargement of the submental fat layer. Deoxycholic acid destroys the cell membranes of the fatty tissue under the chin without affecting the surrounding tissue.
| Kybella (deoxycholic acid) injection sites |
During each treatment session, the patient receives several injections of Kybella.
The session is carried out on an outpatient basis. Session duration is 15-20 minutes. The full course of treatment is 2-4, sometimes up to 6 sessions. Sessions are not held more often. than once a month. In 2021, deoxycholic acid, as an international nonproprietary name, is included in ATX, in “Section D. Drugs for the treatment of skin diseases”, in the group “D11A Other drugs for the treatment of skin diseases” and is assigned the code D11AX24.
On the website GastroScan.ru in the “Literature” section there is a subsection “Diseases of the hepatopancreatobiliary system”, containing publications for healthcare professionals on this topic.
general information
Deoxycholic acid is contained as an excipient in the hepatoprotective drug Essentiale N.
Deoxycholic acid has contraindications, side effects and application features; consultation with a specialist is necessary.
Back to section
Indications for use of the drug Ursodeoxycholic acid
Primary biliary cirrhosis of the liver, primary sclerosing cholangitis, chronic active hepatitis, cystic fibrosis, atresia of the intrahepatic bile ducts, cholestasis with parenteral nutrition, alcoholic liver damage, acute hepatitis, prevention of liver damage when using hormonal contraceptives, treatment with cytostatics (during transplantation); cholesterol gallstones in the gallbladder (if it is impossible to remove them surgically or endoscopically), biliary reflux gastritis and reflux esophagitis, bile duct dyskinesia.
Pharmacological properties of the drug Ursodeoxycholic acid
Synthetic stereoisomer of chenoxycholic acid. It has a membrane-stabilizing and hepatoprotective effect, protecting hepatocytes from damaging factors. It has immunomodulatory activity and reduces the severity of immunopathological reactions in the liver. By stimulating exocytosis in hepatocytes during cholestasis by activating Ca2+-dependent α-protein kinase, ursodeoxycholic acid reduces the concentration of bile acids that are toxic to hepatocytes (cholic, lithocholic, deoxycholic, etc.). Inhibits the absorption of lipophilic bile acids in the intestine (apparently due to a competitive mechanism), increases their “fractional turnover” during the hepatic-intestinal circulation; induces choleresis with a high content of bicarbonates, which leads to an increase in the passage of bile and stimulates the excretion of toxic bile acids through the intestines. By replacing non-polar bile acids, it forms non-toxic mixed micelles. By reducing the synthesis of cholesterol in the liver, as well as its absorption in the intestine, ursodeoxycholic acid reduces the lithogenicity of bile, reduces the cholate-cholesterol index, promotes the dissolution of cholesterol stones and prevents the formation of new ones. Ursodeoxycholic acid is absorbed in the small intestine by passive diffusion and in the ileum by active transport. When taken orally at a dose of 0.5 g, the maximum concentration in blood plasma after 30, 60 and 90 minutes is 3.8, 5.5 and 3.7 mmol/l, respectively. When taken systematically, ursodeoxycholic acid becomes the main bile acid in the blood serum, accounting for about 48% of the total pool of bile acids in the blood. Binding to blood plasma proteins is 96–99%. The therapeutic effect depends mainly on the concentration of ursodeoxycholic acid in bile and not in serum. The concentration of ursodeoxycholic acid in bile depends on the dose: as the daily dose increases, the content of ursodeoxycholic acid in bile increases accordingly. The maximum concentration of ursodeoxycholic acid in bile is observed when it is taken at a daily dose of 10–14 mg/kg. With a further increase in dose, the concentration of ursodeoxycholic acid in bile does not increase (plateau phase). About 50–70% of the administered dose is excreted in bile. Ursodeoxycholic acid penetrates the placental barrier.
Special instructions for the use of the drug Ursodeoxycholic acid
Successful conservative treatment of cholelithiasis is possible in the presence of purely cholesterol (X-ray negative) stones with a diameter of no more than 1.5–2 cm, preserved gallbladder function, patency of the cystic and common bile duct; stones should not fill more than half the volume of the gallbladder. To accurately determine the nature of the stones, it is recommended to perform radiography in combination with ultrasound. To prevent recurrence of cholelithiasis, treatment must be continued for several months after stone lysis. During treatment, transaminase levels should be dynamically monitored at least once a month; if their activity is increased, it is recommended to reduce the dose. Treatment should be discontinued if values do not return to normal within 1 month.