Thrombosis and various diseases of the heart and blood vessels can cause serious complications and even lead to the death of the patient. The vitamin complex “Angiovit” allows you to reduce the risk and alleviate the course of serious diseases. It normalizes blood composition and protects against thrombosis. It is prescribed for many cardiovascular diseases.
Characteristic
Vitamin complex for the prevention and treatment of cardiovascular diseases associated with increased levels of homocysteine, which is one of the factors of damage to the walls of blood vessels.
Elevated levels of homocysteine in the blood (hyperhomocysteinemia) are found in 60–70% of cardiac patients and are one of the main risk factors for atherosclerosis and arterial thrombosis, incl. for myocardial infarction, ischemic stroke, diabetic vascular damage. The occurrence of hyperhomocysteinemia is promoted by a deficiency of folic acid and vitamins B6 and B12 in the body.
In addition, hyperhomocysteinemia is one of the factors in the formation of chronic (habitual) miscarriage and congenital fetal pathology. A relationship has been established between hyperhomocysteinemia and the occurrence of various types of depressive states, senile dementia (dementia), and Alzheimer's disease.
Composition and release form
"Angiovit" are small white tablets protected by a thin coating. They must be swallowed whole without chewing. Pharmacies sell cardboard boxes of 60 pieces each.
The tablet contains three main active ingredients - B vitamins and their derivatives:
- B6 (pyridoxine hydrochloride) - 4 mg;
- B9 (folic acid) - 5 mg;
- B12 (cyanocobalamin) - 6 mcg.
The medicine is made from forms of several B vitamins. This vitamin complex thins the blood and improves the condition of blood vessels.
Angiovitis. Hyperhomocysteinemia in the practice of an obstetrician-gynecologist
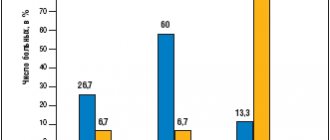
The problem of hyperhomocysteinemia (HHC) has recently attracted the natural interest of doctors of various specialties, including obstetricians and gynecologists. Hyperhomocysteinemia develops due to disorders of homocysteine (HC) metabolism. GC is an intermediate product of methionine metabolism in the body and under normal conditions is found in the body in low concentrations. The main cause of hyperhomocysteinemia is a decrease in the activity of enzymes that ensure the metabolism of HC, as a result of genetic disorders and/or a decrease in the level of cofactor vitamins (folic acid, B6 and B12), which, in turn, may be a consequence of nutritional deficiency, the use of certain medications or the result of a number of diseases. The clinical significance of increased GC levels is determined by a number of reasons. Hyperhomocysteinemia occurs in the population with high frequency, as it can be both hereditary and acquired. HHC is associated with thrombotic complications, neurological symptoms and reproductive dysfunction. Treatment of hyperhomocysteinemia is pathogenetic - the level of GC is normalized when taking folic acid, vitamins B6 and B12 in therapeutic doses. The position about the significant role of HGC in the pathogenesis of reproductive losses is confirmed by analyzing the pathological effects of increased levels of HGC that have been studied to date. It has been proven that hyperhomocysteinemia is one of the causes of anencephaly and spina bifida. Anencephaly is 100% fatal, and spina bifida causes severe neurological problems in the child, including motor paralysis, lifelong disability and premature death. It is known that homocysteine freely passes through the placenta and can have direct teratogenic and fetotoxic effects. It is also possible that excess homocysteine levels may have a toxic effect on the fetal nervous system. Hyperhomocysteinemia is characterized by the development of conditions that can lead to early termination of pregnancy. Childbirth in such cases is accompanied by high infant mortality and a high percentage of neonatal complications. Hyperhomocysteinemia may be one of the reasons for the development of generalized microangiopathy in the second half of pregnancy, manifested in the form of late toxicosis: nephropathy, preeclampsia and eclampsia [1, 2]. In recent years, the role of HHC in recurrent miscarriage has been actively studied. Miscarriage is a serious medical and social problem. From 9 to 13% of women of reproductive age have a history of one undeveloped pregnancy, 5% have two or more. It has been proven that in almost 50% of cases, recurrent miscarriage is a consequence of hereditary and/or acquired thrombophilia [3]. A successful pregnancy outcome depends on the normal development and functioning of the placenta. With thrombophilia, microcirculation is disrupted, vascular thrombosis and placental infarctions develop. The prothrombotic effects of HC can lead to microthrombosis and the development of obstetric complications associated with changes in fetoplacental circulation. There is a hypothesis that thrombophilia can cause the development of thrombosis not only in the mother, but also in the fetus, which can lead to a decrease in its vital functions, and subsequently to death [1]. Features of the physiological adaptation of the hemostatic system to pregnancy, as well as increased folate consumption during fetal development, can lead to the manifestation of thrombophilia caused by HHC, namely fetal loss syndrome in the form of a number of pathological conditions - miscarriages in the first and second trimesters, intrauterine fetal death, placental abruption, severe gestosis. We examined 440 women aged 20 to 45 years, referred from specialized medical institutions in St. Petersburg with a diagnosis of miscarriage (MP) and an age-matched control group (n=120). The GC level was determined using the reference high-precision high-pressure liquid chromatography method [4]. The average level of HC in women with NB significantly exceeded this indicator in the control group (11.8 ± 4.2 µmol versus 6.5 ± 1.4 µmol, p). The results obtained indicate that HC is a significant and fairly common risk factor for miscarriage pregnancy in the population of the North-Western region of Russia. According to the results of our studies, consistent with the data of other authors, the prothrombotic potential of HHC is realized through a toxic effect on the vascular wall; activation of both platelet and coagulation components of hemostasis; increased generation of thrombin, decreased activity of the natural anticoagulant system and fibrinolysis. These pathogenetic mechanisms lead to the development of both arterial and venous thrombosis in HHC [2]. The risk of developing vascular pathology in HHC is dose-dependent and occurs already at HC levels above 10 μmol. The leading pathogenetic link in HHC is endothelial dysfunction, manifested inhibition of its anticoagulant and activation of procoagulant properties. The biochemical basis of this process is oxidative stress initiated by excess GC. Endotheliopathy due to HHC interferes with the normal functioning during pregnancy of a unique, complexly functioning system of three endothelial surfaces - fetoplacental endothelium, uterine vascular endothelium and trophoblast endothelium [1, 2, 4, 5]. Timely diagnosis of HHC is of great clinical importance, since pathogenetic therapy with B vitamins allows normalizing the level of HHC, prolonging pregnancy until timely birth and preventing the development of complications. Thus, a prospective observation of 55 women with recurrent miscarriage we examined earlier showed that normalization of GC levels, the use of antioxidant, antiplatelet and anticoagulant therapy under the control of hemostasis parameters allowed us to achieve a successful pregnancy outcome in 84% of cases. Moreover, in 68% of patients, the dose of folic acid required to maintain HC levels at a normal level for pregnancy was 5 mg per day, and only in 32% of cases the average daily dosage reached 15 mg per day [6]. When caring for a patient with suspected thrombophilia, it must be remembered that the HC level during physiological pregnancy is 50–60% lower than in non-pregnant women of the same age. The concentration of GC, according to data obtained from a study of 155 healthy pregnant women, averages 5.6 µmol in the first trimester, 4.3 µmol/l in the second trimester, and 3.3 µmol in the third [4]. The clinician also needs to know that HHC, especially in combination with such forms of thrombophilia as a mutation in the prothrombin gene and a mutation in factor V Leiden, significantly increases the risk of developing venous thrombosis both during pregnancy and in the postpartum period. According to our data, with a HC level of more than 10 µmol, the relative risk of developing venous thrombosis significantly increases - RR = 1.8 (p = 0.0009), with a HC level of more than 13.4 µmol, the risk increases to 3.1 (p Discussing the problem of thrombotic complications of HHC, which obstetricians-gynecologists may encounter in their clinical practice, one cannot fail to touch upon another extremely important aspect of the problem - an increase in the level of HHC when using combined hormonal contraceptives.Combined oral contraceptives (COCs) are highly effective means of contraception and are used by a huge number of women in all over the world. In addition, the prescription of COCs is a method of treating a number of pathological conditions, including premenstrual syndrome (PMS), which is characteristic of a significant proportion of women of reproductive age. Despite many years of global experience in the use of COCs, issues of the safety of their use continue to remain relevant. COCs increase risk of thrombotic complications.At the same time, not only high-dose COCs of the first generation, but also low-dose COCs of the second and third generations have a prothrombotic effect. If for women of reproductive age the absolute risk of thrombus formation is on average less than 1 per 10,000 per year, then when using II generation COCs it increases to 12 per 10,000 per year, and III generation - to 30 per 10,000 per year [7]. COCs remain the most common cause of thrombotic complications in young women, and minimizing prothrombotic risks with hormonal contraception remains a critical goal. In women with various forms of thrombophilia, hormonal contraception increases the risk of thrombosis by 3–30 times. Despite the fact that HHC is the most common cause of thrombophilia, the effect of COCs on HHC levels has not been sufficiently studied. Foreign authors have previously shown that when taking COCs, the content of vitamins B2, B12 and B6 in the body can significantly (by 30%) decrease and folate metabolism is disrupted [1, 2]. We observed 60 patients with PMS who received therapy with combined hormonal contraceptives for a year. A fairly high incidence of initial HHC was noted in patients with PMS (15% versus 3% in the control group, p Pathogenetic treatment - taking the drug Angiovit (manufactured by the pharmaceutical company), containing 5 mg of folic acid, 4 mg of vitamin B6 and 6 μg of vitamin B12, in therapeutic doses, 1 tablet per day for 1 month - allowed to reduce the HC level to normal in 100% of patients. When using a low-dose COC containing 20 mcg ethinyl estradiol and 150 mcg desogestrel, in women with normal initial HC values there was a steady tendency to increase in the level of GC after 3, 6 and 12 months of taking the drug compared to the initial figures (7.6–8.6–9.6–10.2 µmol).The use of COCs increased the content of GC in the blood plasma by an average of 4 µmol/ l. Taking folic acid, vitamins B6 and B12 effectively eliminated HHC and made it possible to maintain the level of HHC within normal fluctuations during the period of using COCs [8].Taking into account the fairly high frequency of occurrence of hereditary and acquired HHC in the population as a whole, it is impossible to implement determination of the level HC as a screening test before starting hormonal contraception, as well as an increase in HC level when taking third-generation COCs (the most common method of contraception at present), recommendations for the preventive intake of folic acid, vitamins B6 and B12 when using contraceptive steroids are appropriate and justified. Summarizing the above, I would like to emphasize once again that hyperhomocysteinemia is a pathological condition that occurs with high frequency in the population and plays a significant role in the structure of general morbidity and reproductive losses. Particularly significant is the fact that HHC is easily eliminated with the use of accessible, safe and inexpensive vitamin preparations. The domestic drug Angiovit, containing folic acid, vitamins B6 and B12 in therapeutic doses, has proven itself excellent in the treatment of HHC both in patients with thrombosis and in women with a complicated obstetric history.
Can I take it during pregnancy?
Doctors recommend taking Angiovit already at a time when a woman is just about to become a mother. This medicine will help avoid the tragic consequences of a lack of B vitamins for newborns. "Angiovit" is prescribed to avoid the following intrauterine pathologies:
- splitting of the spinal cord (spina bifida);
- heart defects;
- weak immunity;
- anencephaly;
- developmental delay;
- underdevelopment of blood vessels.
The medicine must be taken during all periods of pregnancy, especially at the very beginning, when the child’s nervous system is being formed.
Contraindications and side effects
"Angiovit" should not be taken by patients who have been found to be hypersensitive to the substances that make up the medicine. Side effects manifest themselves in the form of allergic reactions:
- hives;
- headache;
- angioedema;
- dizziness;
- redness and itching of the skin;
- sleep disorders;
- nausea, vomiting;
- abdominal pain.
Most patients tolerate Angiovitis well, especially in spring and autumn, when the lack of vitamins is especially acute.
Overdose symptoms
Medicine does not know of cases of overdose with Angiovit. But if the patient drinks this medicine uncontrollably and in large quantities, he will develop signs of hypervitaminosis. It manifests itself in the form of a number of symptoms:
- numbness of the limbs and other parts of the body;
- tremor of hands and feet;
- impaired coordination of movements;
- prolonged cramps, most often in the calf muscles;
- capillary thrombosis;
- anaphylactic shock.
Particularly severe consequences (thrombosis and shock) are caused by excessive consumption of vitamin B12, so you must take the tablets very carefully.
It is necessary to comply with the dosage and regimen of taking medications.
Interaction with other drugs
"Angiovit" should not be taken together with medications that increase blood clotting. The consequences of such a treatment can be unpredictable: the blood becomes viscous, which causes blood clots to form.
Allergies can occur when Angiovit is combined with thiamine; this effect is created by cyanocobalamin, which is part of the drug. The absorption of vitamin B12 in the stomach is reduced if Angiovit was taken together with antiepileptic drugs, colchicine, aminoglycoside antibiotics, salicylates and potassium-based drugs.
If “Angiovit” was prescribed along with glycosides for the heart, then the myocardium will be well protected from hypoxia. This effect is created by pyridoxine: thanks to its action, contractile proteins of the heart muscle are actively formed. It goes well with Asparkam and glutamic acid.
Pyridoxine weakens the effect of the drug Levodopa for Parkinson's disease, but enhances the effect of thiazide diuretics.
There are drugs that reduce the effect of vitamin B6. These include cycloserine, penicillamine, contraceptives containing estrogen and isonicotine hydrazide.
Vitamin B9 weakens the effects of Phenytoin and Carbamazepine (for epilepsy and arrhythmia), so the dosage has to be increased. Only the attending physician can correct it.
"Angiovit" should not be taken by those patients who are prescribed Methotrexate, Pyrimethamine, Trimethoprim or Triamterene. Also, "Angiovit" is incompatible with sulfonamines, "Kolestyramine" and anti-ulcer antacids based on magnesium and aluminum. Because of this combination, the therapeutic effects of both drugs disappear.