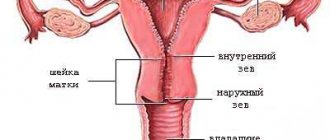
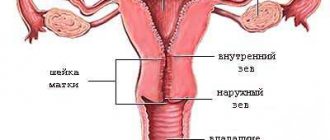
Normally, during childbirth, the cervical part of the uterus opens up to 10-12 cm during contractions. After this, pushing begins and the fetus is pushed out. After childbirth, the cervix gradually returns to its original state.
Cost of services in our clinic
| Appointment with a gynecologist with the highest category | 1000 rub. |
| Consultative appointment with a doctor based on test results and ultrasound results | 500 rub. |
| Extended colposcopy | 1500 rub. |
| Amino test for bacterial vaginosis | 300 rub. |
| Medical abortion (all inclusive) | 4500 |
| Make an appointment by phone: 8-800-707-15-60 (toll-free) |
| *The clinic is licensed to remove tumors |
However, the birth of a child does not always go smoothly: one of the most common complications (6%) is cervical rupture.
If for any reason postpartum tears are not sutured or done incorrectly, after the tissues have fused, the cervix becomes deformed. The pathology requires treatment, as it causes complications - severe inflammation, miscarriages, infertility.
Symptoms
Signs of uterine prolapse consist of dysfunction of those organs that are involved in the pathological process. The displacement of the uterus itself causes:
- feeling of a foreign body in the vagina
- discomfort during sexual activity
- pulling sensations in the lower abdomen.
It is important to remember the fact that the uterus lies at the apex of the vagina, so its prolapse is inevitably accompanied by prolapse of the anterior/posterior wall of the vagina, and therefore the bladder/rectum.
This is why patients with “prolapse of the uterus” complain:
- for urinary disorders (difficulty urinating, a feeling of incomplete emptying of the bladder, frequent urination, loss of urine when straining or against the background of a strong urge, etc.)
- for problems with defecation (difficulty defecating, defecation in portions, the need to reduce prolapse to completely empty the bowel, etc.).
| anonymously to the doctor, through the feedback form, we will try to help you. | Ask a Question |
How does a woman feel when her cervix is deformed?
The inverted mucosa is affected by the acidic environment of the vagina, which causes inflammation, erosion, and the formation of vaginal-cervical fistulas. Isthmic-cervical insufficiency occurs - the tissues become weak and cannot support the fetus during the next pregnancy. With severe deformation, conception is impossible due to the difficulty of sperm penetration into the uterine cavity.
The tissues of the cervical canal, normally covered with protective mucus, remain unprotected: a “gate” for infections is created. Microbes easily penetrate the uterus from the vagina, causing cervicitis and endometritis. Signs of infection are disruptions in the menstrual cycle, pain in the lower abdomen and lumbar region, copious foul-smelling discharge that irritates the genital mucosa.
Deformation, shortening of the cervical part of the uterus, rough sutures cause pain during sexual intercourse. Narrowing of the cervical canal leads to retention of menstrual blood in the uterine cavity and new inflammatory processes.
The doctor determines cicatricial changes in the cervix caused by postpartum tears during a vaginal examination and colposcopy. In gynecological speculums, rough sutures and everted areas of the mucous membrane are visible.
Causes
The causes of uterine prolapse can be described according to the life course model. At the beginning, a person has one or another predisposition to the development of this pathology. Then various aggressive factors begin to act on it, which lead to the onset of the disease. At the first stage, the body copes with the damage that has arisen, but age and the accumulation of damage leads to its manifestation and, in fact, to the complaints that were described above. All pathological factors can be divided into the following:
- Heredity. It has been proven that if close relatives have the disease, the likelihood of occurrence increases several times. Most often, there is a congenital weakness of the connective tissue, which affects other systems of the body, manifesting itself in diseases of the musculoskeletal system, varicose veins, and hemorrhoids. However, heredity is still not a death sentence, and what makes it a reality are the risk factors, which will be discussed below.
- Childbirth and pregnancy. Perhaps the main factor that leads to changes in the qualitative composition of the supporting apparatus of the pelvic floor and its partial damage. Unfortunately, with severe tissue failure, complete prolapse of the uterus can develop immediately after childbirth. On the other hand, for most women in labor, the prolapse completely regresses within the first year.
- Increased loads. And this is not only hard physical labor, but also chronic constipation, lung diseases accompanied by a constant and severe cough, and obesity. All these factors lead to damage to the ligamentous apparatus of the pelvic organs and their prolapse.
- Age. This factor has a complex effect on all supporting structures of the pelvic floor. Firstly, with age, hormonal levels change, and with it the quality of connective tissue (it becomes looser and weaker). In some patients, hormonal changes lead to deformation and changes in the cervix, such as its elongation and hypertrophy. Secondly, muscle tone decreases, including that of the pelvic floor. In this regard, injuries to the ligamentous apparatus once received lose their support and become obvious.
Why do severe postpartum cervical ruptures and deformation occur?
The content of the article
Mild cervical ruptures are normal during childbirth; they heal quickly and therefore do not require treatment. Severe ruptures are the result of incorrect behavior of the woman in labor (early pushing), illiterate or traumatic obstetric care with the use of obstetric forceps or a vacuum extractor, rapid or late labor.
The cervix ruptures for other reasons, for example, if a woman has already had a childbirth with stitches.
When several factors combine, severe cervical ruptures occur that are difficult to stitch. Inexperienced gynecologists apply rough or uneven sutures. And if childbirth occurs suddenly, in unsuitable conditions, the woman is left without medical care at all. As a result, the cervix becomes deformed - it thickens, shortens and bends, and the internal mucous membrane turns outward.
Diagnostics
Diagnosis of uterine prolapse does not raise questions among specialists. To do this, it is necessary to conduct a standard gynecological examination, on the basis of which the stage of prolapse is set and the part of the vagina involved in the pathological process is determined.
Most often, damage occurs to all three sections of the pelvic floor: anterior, posterior and apical.
In total, there are four degrees of uterine prolapse: the first (initial), when the patient is practically not bothered by anything, the fourth degree is accompanied by complete prolapse of the pelvic organs.
The study can be supplemented with a digital rectal examination to exclude rectal prolapse.
As instrumental methods, ultrasound of the pelvic organs and sometimes MRI are performed.
| Most patients receive care for free (without hidden additional payments for “network”, etc.) as part of compulsory health insurance ( under the compulsory medical insurance policy ). | Application for treatment under compulsory medical insurance |
WHAT IS USEFUL FOR THE UTERUS, ITS TREATMENT AND RESTORATION
Women who have undergone acute or chronic endometrial processes, abortion, gynecological surgery, need measures to restore the uterine mucosa, treat and maintain the hormonal function of the ovaries. This justified need may be caused by the following unfavorable factors:
- Functional failure in the production of hormones by the pituitary gland, ovaries and hypothalamus. This usually occurs after ovarian surgery, surgical or mini-abortion, and to a lesser extent after medical abortion.
- Mechanical damage to the endometrium or cervix. Trauma to the mucous membrane in the uterine cavity leads to the formation of intrauterine synechiae and adhesions in the pelvis.
The course of treatment of the uterus to restore its normal functioning after gynecological operations and any abortions includes a set of measures aimed at preventing complications and their long-term consequences. At the following link you can find out what procedures our clinic offers for the rehabilitation of women’s health after peri- and intrauterine interventions that are beneficial for the uterus.
Find out about a good preventative remedy - how to restore the health of the uterus, strengthen and support the female reproductive system as a whole, without taking medications and hormones: “UTERUS AND OVARIES MASSAGE”
Read articles about uterine diseases:
• INFLAMMATION OF THE UTERUS • BEND OF THE UTERUS • CERVICAL EROSION • CAVITY POLYPOSIS • TREATMENT OF ENDOMETRITIS
Treatment
Treatment of uterine prolapse includes surgical and conservative treatment methods.
Conservative methods include:
- Kegel exercises for uterine prolapse are aimed at increasing the tone of the pelvic floor muscles. Due to this, the damaged ligamentous apparatus has a foundation that prevents the pelvic organs from descending excessively. Unfortunately, it is quite difficult to perform these exercises correctly, since it is difficult to train something that you cannot see and do not control. To solve this issue, biofeedback devices (BFB therapy) were developed, which increases the effectiveness of exercises several times. This method will be useful for young patients and women after childbirth.
- Pessaries and bandages are aimed at creating an obstruction in the path of descending organs. When the uterus prolapses, the pessary is placed in the vagina and serves as a kind of spacer. Unfortunately, the presence of a foreign body inside often causes discomfort, chronic inflammation and, most importantly, requires regular visits to the gynecologist to change it. In the case of bandages, they are simply tight underwear that prevents prolapse from leaving the vagina. Sometimes it is combined with a pessary and works like a “plug”. These methods can be used if the operation cannot be performed for some reason. This can be compared to a crutch for a limb injury.
The advantages of my original method of treating genital prolapse:
- preservation of the most natural anatomical and topographic relationships of the pelvic organs;
- minimizing the risk of recurrence of uterine prolapse;
- minimal risk of postoperative complications (erosions of the vaginal mucosa, dyspareunia, damage to neighboring organs, bleeding, infectious complications) - up to 0.1% compared to 30% when using Prolift);
- minimal trauma
- improving the quality of life (the possibility of sexual activity is not limited, unlike the Prolift operation);
- the fastest possible rehabilitation period (the average length of hospitalization after surgery does not exceed 3 days, the possibility of vigorous activity remains);
- no need for long-term hormonal preparation before surgery (unlike classical promontofixation and installation of the Prolift system);
- the possibility of simultaneous correction of other extragenital and gynecological pathologies (pelvic diseases - fibroids, adenomyosis, tubal adhesions, ovarian cysts, etc., each of which seriously affects a woman’s health and ability to bear children).
Diploma
For the best work in the section “Laporoscopic methods in coloproctology”
Formula of invention to the RF patent
Patent holder(s): Konstantin Viktorovich Puchkov
The results of treatment of patients with pelvic prolapse are summarized in three monographs “Laparoscopic operations in gynecology”, “Simultaneous laparoscopic surgical interventions in surgery and gynecology” and “Minimally invasive colon surgery”, as well as in more than 20 scientific publications in various professional peer-reviewed scientific publications in Russia and abroad. As a result of many years of positive attempts to use this technique, we received patent No. 2015126579 of the Russian Federation “Method of laparoscopic promontofixation / K.V. Puchkov, V.V. Korennaya, D.K. Puchkov.- No. 2 2015126579/14; appl. 07/02/2015; publ. 03/09/2017, Bulletin 7.
Operation
The main method of treatment is still surgical, since the supporting apparatus of the pelvis is not restored. Unfortunately, the most popular method, removal of the uterus, often does not help, since not only the uterus, but the pelvic organs (bladder, rectum) prolapse.
For this reason, this approach leads in 30-50% of cases to the development of prolapse of the vaginal stump.
Another problem with hysterectomy is posthysterectomy syndrome, which leads to impaired urination, defecation and decreased sexual function, including due to postoperative shortening of the vagina. Reconstructive operations performed through the vagina seem to be the most optimal and proven. On the one hand, they allow you to achieve a good anatomical result, on the other, a good cosmetic effect. One of the most modern techniques are hybrid operations, which allow the operation to be individualized for each specific patient, while maximizing the use of his own tissues, and, if necessary, supplementing them with a prosthesis only in the busiest places.
Vaginal hysterectomy
Vaginal hysterectomy is surgery to remove the uterus through an incision at the top of the vagina. Also, the ovaries may be removed during the operation. The advantages of the procedure include: small blood loss compared to abdominal hysterectomy, short rehabilitation period, less severe pain. However, despite this, hysterectomy is performed vaginally in only 30% of women, which is associated with indications for this operation: sufficient mobility and small size of the uterus, absence of pathologies of the pelvic organs, normal vaginal dimensions. Possible complications: infection, formation of adhesions, bleeding, there is an increased likelihood of damage to adjacent organs due to the low visibility.
Classification:
There are several main modifications of the operation of vaginal hysterectomy: according to Mayo, Yolkin, Aleksandrov, Persianinov, etc.
Indications for surgery:
Prolapse and loss of internal genital organs, uterine pathology (including complete and incomplete uterine prolapse, small uterine fibroids, uterine endometriosis), which requires its removal.
Contraindications:
History of laparotomy with severe adhesions in the abdominal cavity (relative contraindication); combined pathology (for example, ovarian tumor), which requires a revision of the abdominal cavity. A large uterus is not an absolute contraindication for vaginal hysterectomy.
Conditions for the operation:
In the absence of emergency indications, surgical intervention cannot be performed in the presence of acute inflammatory diseases of any location (including acute respiratory infections, influenza), or the presence of acute inflammatory diseases of the vagina and cervix. In the presence of extragenital pathology, it is necessary to carry out careful preoperative preparation to achieve compensation or remission of the process.
Pain relief methods:
It is preferable to use regional (spinal or epidural) anesthesia, as well as combined anesthesia and endotracheal anesthesia.
Operation technique:
The choice of surgical technique depends on the degree of displacement of the uterus, the presence and degree of elongation of the cervix, the presence or absence of adhesions in the abdominal cavity, pathology of the uterus and appendages.
Technique for vaginal hysterectomy according to Mayo:
A circular incision is made in the vaginal wall, 5–6 cm away from the external pharynx (or along the last transverse fold of the vagina). Using closed Cooper scissors, inserted under the fascia, the bladder is peeled off from the fascia covering it, moving the scissors to the upper corner of the wound (the ends of the scissors should be visible through the fascia so as not to injure the bladder). A midline incision is used to cut through the fascia to the upper corner of the wound. The bladder is additionally separated from the fascia to its lateral sections, then from the cervix and peritoneum upward, dissecting the prevesical tissue. As a result, the peritoneum of the anterior fornix is exposed, which is opened (anterior colpotomy). The cervix is pulled as far upward as possible, towards the womb. Using a Mikulicz clamp, the posterior wall of the vaginal vault is grasped and cut with scissors (posterior colpotomy). The incision is brought to the origin of the uterosacral ligaments. Three separate ligatures are placed on the posterior wall of the vagina, capturing the opened peritoneum, and the threads are taken onto holders. Bullet forceps are applied to the anterior wall of the uterus and “dislocate” it into the anterior colpotome opening of the wound. Clamps are applied and the uterosacral, cardinal ligaments and bundles of uterine vessels are transected on both sides in stages. Strong clamps are applied to the upper parts of the broad ligaments, including the round ligaments of the uterus and the stumps of the uterine appendages (uterine ends of the tubes and proper ovarian ligaments), and the uterus is cut off. Tissues taken in clamps (ligaments, vessels, stumps of appendages) are sewn with a counter furrier's seam, trying not to puncture the vessels. The suture begins from the top, gradually removing the clamps. The furrier suture is strong, tightens well, there is no need for separate ligation of blood vessels, which significantly reduces the operation time. However, this manipulation is possible only with sufficient experience, confidence of the surgeon and efficient work of the operating team. Untimely removal of the clamps - too early or, conversely, too late, can lead to the escape of blood vessels and bleeding or the formation of a hematoma. In this regard, in the absence of sufficient experience, it is possible to separately stitch and bandage all the crossed formations (sacrouterine, cardinal ligaments, stumps of the uterine vessels and uterine appendages). After this, sew them together (sacral ligaments with uterosacral ligaments, cardinal ligaments with cardinal ligaments, etc.) with separate vicryl sutures. To create a strong support for the bladder, the ligaments of the uterus are fixed to the walls of the vagina. For this purpose, a needle is inserted immediately at the upper corner of the wound through the vaginal mucosa, fascia and peritoneum of the bladder, the upper segment of the connected uterine ligaments behind the mattress suture and punctured through the described layers in the opposite direction of the opposite edge of the wound. A second suture is made with the same thread, capturing the edges of only the vaginal mucosa. Several such sutures are placed at a distance of 1.5–2 cm downwards from the first one. With these sutures, the vaginal wall is fixed to the interconnected ligaments of the uterus. The last suture strengthens the vaginal wall in the area of the stump of the uterosacral ligaments. With this suture, the ligament stumps are located extraperitoneally. The posterior vaginal vault is closed with interrupted sutures, applying them in the transverse direction. Colpoperineolevatoroplasty is performed.
Surgical technique in the absence of significant prolapse of the uterus and vaginal walls:
The cervix is grabbed with a two-pronged clamp so that the anterior and posterior lips are immediately captured (reliable fixation of the uterus with low mobility is one of the conditions for the successful performance of this operation), and it is reduced as much as possible. After fixing the uterus, use a short mirror and, if necessary, side lifts (to improve visibility, you can fix the labia minora to the skin). A circular incision is made in the vagina at the border of its transition to the cervix (along the last transverse fold) and peeled upward using a blunt and sharp method. Clamps are applied to the cardinal ligaments, they are crossed and ligated with vicryl with stitching, and the ligatures are placed on holders. By pulling the uterus down, the bladder is peeled off to the vesicouterine fold. One of the techniques that greatly facilitates the operation in conditions of low mobility of the uterus is the opening of the posterior vaginal vault, as this allows one to be well oriented in the anatomical relationships. After the posterior vaginal fornix is opened, the uterosacral ligaments are crossed and ligated with stitching, and the uterus becomes increasingly mobile. The vesicouterine fold is opened and sutured to the vaginal mucosa (many surgeons, immediately after sufficient mobilization of the bladder, open the vesicouterine fold and then open the posterior vaginal fornix - all this depends on the personal preferences of the surgeon and his skills and does not have a significant impact on the course of the operation). The fundus of the uterus is grabbed with bullet forceps and dislocated into the wound, after which the ribs of the uterus become accessible: the round ligaments of the uterus, the proper ovarian ligaments and the fallopian tubes. Clamps are applied to them, they are cut and ligated with vicryl and stitching. When the uterus is pulled toward itself and downward, clamps are applied to the uterine vessels. The vessels are divided and ligated. The uterus is removed. After removal of the uterus, the wound is sutured so that the ligament stumps remain outside the peritoneum. To do this, the first suture is placed on the left so that the needle passes through the vaginal wall, peritoneum, ligament stumps and vascular bundle, peritoneum of the rectal uterine cavity and the posterior wall of the vagina. Then only the vaginal walls are captured with the same suture. The thread should not be tied to make it easier to apply the suture on the other side. On the right, the suture is applied in such a way that it first grasps the posterior wall of the vagina, the peritoneum of the rectouterine cavity, the stumps of vascular bundles and ligaments, and then the vesicouterine fold of the peritoneum and the anterior wall of the vagina. After the threads are pulled through on both sides, knots should be tied. When the sutures are applied correctly, the vaginal walls are connected. The stumps of the ligaments remain between the layers of the peritoneum and the vaginal wall, i.e. reliably peritonized. If necessary, an additional suture can be placed on the vaginal wall. It is not necessary to achieve complete tightness of the abdominal cavity, since if there is wound discharge, it is discharged out.
The surgical technique as modified by V.I. Krasnopolsky et al.:
The cervix is securely fixed by both lips and brought down as much as possible; a triangular flap is cut out from the mucous membrane of the anterior vaginal wall with a scalpel (the top is 1.5–2 cm below the external opening of the urethra, the base is facing the cervix). The incision continues into a circular one around the cervix (at the level of the last transverse fold or along the length of the vagina being formed). The width of the flap is always individual and depends on the presence and degree of cystocele. The vaginal mucosa is peeled off from the prevesical fascia. The flap to be peeled off must be thin and consist only of the mucous membrane, not contain elements of the prevesical fascia; for this it must be fixed with Kocher clamps and, when peeled off, placed on the “cushions” of 2-3 fingers of the surgeon’s left hand, all the time maintaining the tension of the flap with the fingers and controlling it thickness. Many surgeons do not use hydraulic tissue preparation, i.e. do not inject an anesthetic solution (procaine) or an isotonic sodium chloride solution under the mucous membrane, since it is believed that the introduction of the solution, especially uneven and excessive, distorts the anatomical relationships and makes orientation difficult. Then it is advisable to slightly (approximately 1 cm) peel the edges of the mucous membrane from the fascia to the sides for their optimal comparison in the future. To mobilize the bladder, when the cervix is pulled downwards, the connective tissue fibers between the bladder and the cervix and the fibers of the vesicovaginal septum are crossed, the bladder is shifted upward using a sharp and blunt method. Usually the boundaries of the bladder are clearly visible; if there are difficulties, its boundaries are determined using a metal catheter. For better visualization of the vesicouterine fold, the bladder is pulled upward using a lift, while the peritoneum is exposed in the upper corner of the wound - it is whitish in color and slightly “overhangs”. If the peritoneum of the anterior fornix is clearly visible, it is opened in the transverse direction, the peritoneal incision is continued to the sides (within visibility, i.e. transparency) and sutured to the vaginal mucosa. With significant elongation of the cervix before the opening stage, the cardinal ligaments are crossed and ligated with vicryl stitching (sometimes in several stages), the threads are taken onto a holder. If it is difficult to find the peritoneum of the anterior fornix, for example, in the presence of adhesions (after a cesarean section, as a result of PID), to prevent injury to the bladder and abdominal organs, it is advisable to first perform a posterior colpotomy. Then, under visual control, the plica vesicouterina is cut in a safe place on the finger inserted into the anterior fornix. To open the peritoneum of the posterior fornix, the uterus is pulled as far upward as possible, towards the womb. The peritoneum of the posterior vaginal vault is opened (posterior colpotomy). The posterior wall of the vagina is sutured to the peritoneum of the posterior fornix with separate vicryl ligatures (3–4 sutures), the threads are taken onto a holder. The uterosacral ligaments on both sides are divided and ligated with vicryl sutures. At this stage, reliable fixation (suturing) of the uterosacral ligaments to the vaginal wall is especially important. The threads are also taken onto holders. When the uterus is pulled in the opposite direction, the uterine vessels are crossed and ligated with stitching, the threads are taken onto holders. Bullet forceps are applied to the anterior wall of the uterus and the uterus is “dislocated” into the opening of the wound of the anterior fornix. Payra clamps or any other strong clamps are placed along the ribs of the uterus to prevent tissue from slipping out after removal of the uterus. The uterus is cut off. The tissues taken into the clamps (peritoneal layers, round ligaments, uterine ends of the tubes and the ovarian ligaments) are stitched with a shaped suture and securely tied with a turn. In the presence of massive stumps (the danger of the ligature slipping or loosening after reducing the swelling of the stump), additional (safety) sutures are applied. The abdominal cavity is drained with a tupper, the stumps of all ligaments and uterine vessels are pulled into the wound and once again examined for the reliability of hemostasis. If necessary, additional hemostatic sutures are applied. If it is necessary to remove the appendages after removing the uterus, long mirrors are inserted into the abdominal cavity. In this case, the infundibulopelvic ligaments become accessible, on which clamps are applied. The ligaments are cut and ligated. Ligatures are held on clamps. Starting from the upper corner of the wound, peritonization is carried out with a purse-string vicryl suture on a built-in needle so that the stumps of all ligaments and the vascular bundle are located extraperitoneally. With the correct surgical technique and peritonization, all large blood vessels that can cause significant bleeding in the postoperative period will be located extraperitoneally, the bleeding will be external (into the extraperitoneal space and then into the vaginal dome), where it is more accessible for diagnosis and assistance than intra-abdominal bleeding. Additionally, the stumps of the uterine appendages, uterine vessels, cardinal and uterosacral ligaments are gradually sutured together. Separate vicryl sutures are placed on the mucous membrane of the anterior vaginal wall. The posterior vaginal vault is formed with separate vicryl sutures, applying them in the transverse direction. The mandatory final stage of the operation is colpoperineolevatoplasty.
Complications:
- injury to the bladder during its mobilization or opening of the anterior fornix;
- injury to the rectum or adjacent intestine when opening the posterior fornix;
- injury to the ureter is a rare complication; to prevent it, clamps during the operation must be applied directly along the cervix, then along the ribs of the uterus;
- escape of blood vessels, formation of hematomas during surgery.
What to do in advanced cases
In this case, the walls of the vagina descend so much that the pelvic organs and even the abdominal cavity are displaced into the genital tract. Prolapse of the cervix and its body is often observed. Grade 3-4 prolapse requires only surgical treatment.
With advanced prolapse of the vaginal walls, the following may occur:
- Cystocele is prolapse of the bladder. Occurs when the anterior wall subsides.
- Rectocele is prolapse of the rectum. Occurs when the posterior wall subsides.
- Enterocele is prolapse of loops of the small intestine. Occurs when the upper-posterior part of the vaginal wall prolapses.
Cystocele, rectocele, enterocele
To eliminate this condition, colporrhaphy is performed, which can be:
- Anterior – correction of sagging anterior vaginal wall and bladder prolapse.
- Posterior – treatment of prolapse of the posterior wall with the return of intestinal elements to their place.
- Combined or complete. In this case, both walls of the vagina are tightened, and all displaced organs return to their correct position.