It is not news that diseases of the cervix can result in the development of cervical cancer, and this pathology is increasingly found among young women who have given birth and middle-aged women who do not present any complaints. The need for early diagnosis is important because the process of cancer formation is staged and includes background and precancerous diseases, cancer in situ (cancer “in situ”) and advanced cervical cancer. In this regard, the study of both benign and precancerous diseases is of great preventive importance.
Risk factors for the development of cervical diseases include bacterial and viral infections, especially human papillomavirus (HPV) and herpes simplex virus (HSV). The role of HPV in the occurrence of cervical cancer has been proven. Risk factors also include: early onset of sexual activity and early first pregnancy (before 16 years of age), multiple sexual partners, unprotected sexual intercourse, cervical injuries during childbirth and abortion, smoking, menstrual irregularities, immunodeficiency.
I. Exo- and endocervicitis
This is an inflammation of the mucous membrane of the exocervix and endocervix, which can be caused by both opportunistic microflora (streptococci, staphylococci, E. coli) and urogenital infection (myco-, ureaplasmosis, trichomoniasis, chlamydia, viral infections).
There are no specific clinical symptoms of inflammation; most often the disease is manifested by the appearance of more abundant discharge from the genital tract (leucorrhoea), very rarely dull pain in the lower abdomen, associated mainly with concomitant diseases (urethritis, cystitis).
Diagnostics
A gynecological examination reveals hyperemia around the external pharynx, mucous or purulent discharge.
Colposcopy helps not only to diagnose cervicitis, but sometimes to clarify its etiology.
So, according to the colposcopic picture, it is possible to differentiate inflammation of chlamydial, viral, candidiasis and trichomonas etiology.
With trichomanasic cervicitis, the so-called “strawberry cervix” symptom is observed, when small petechial hemorrhages are visualized on the cervix during colposcopy.
Trichomonas diffuse cervicitis
Candidal cervicitis is accompanied by an alternation of “rough” zones with a “varnished” surface, as well as the appearance of typical cheesy discharge on the cervix and vaginal walls.
Candidiasis cervicitis
A typical symptom of viral cervicitis is the symptom of “large erosion,” when the entire surface of the cervix is bright red with ulcers.
Chlamydial cervicitis is accompanied by swelling of the ectopic columnar epithelium, foci of necrosis and ulceration, and mucopurulent discharge.
To clarify the etiology of inflammation, it is also necessary to take a smear for flora, a culture tank and sensitivity to antibiotics from the cervical canal, a scraping for urogenital infection using the PCR method and a PAP test to exclude background and precancerous diseases.
Treatment depends on the pathogen that caused the inflammation and its sensitivity to antibiotics.
Considering that most often the cause is several pathogens, local drugs with anti-inflammatory, antibacterial and antifungal effects are used in treatment (Polygynax, Terzhinan, Klion-D, Betadine).
For gonorrheal, trichomonas, herpetic etiology of cervicitis, oral antibacterial or antiviral drugs are used in combination.
Rehabilitation period
The rehabilitation period depends on the type and stage of the disease, as well as on the method of its treatment. For example, with laser therapy for erosion it lasts 5-7 days. During this time, tissue rejection and wound healing on the surface occurs. The woman should stay at home, but visit a gynecologist to monitor the healing process.
During the rehabilitation period, minor pain in the lower abdomen and streaks of blood in the discharge may occur 7-10 days after the erosion has been removed. Complete tissue restoration occurs after one to one and a half months.
Contact us to sign up for an examination using the contacts listed on the website.
II. True cervical erosion
Quite often, doctors use the term “cervical erosion,” thereby denoting deviations from the norm when examined with the naked eye. Basically, these “deviations” turn out to be ordinary ectopia or pseudo-erosion.
True erosion is a violation of the integrity of the epithelium (ulcer) and is rare during the reproductive period.
In this case, degeneration and desquamation of the stratified squamous epithelium occurs with exposure of the subepithelial stroma.
Causes of true cervical erosion.
1. Inflammatory process. Long-term discharge in colpitis and cervicitis of various etiologies leads to pathological changes in the cervical mucosa, increased epithelial permeability to microorganisms, its degeneration and desquamation.
2. Cervical injuries. Mechanical damage to the cervix during childbirth and a pathological reaction to the suture material used for reconstruction of ruptures, trauma to the cervix with mirrors during examination may be one of the reasons for the appearance of true erosion of the cervix.
3. Burns of the cervix. After treating the cervix with various methods (chemo-, electro-, cryodestruction), as a rule, the scab is rejected, resulting in the formation of an erosive surface that gradually epithelializes.
4. Trophic disturbances. The risk group for the occurrence of this disease is patients with uterine prolapse, when tissues are traumatized by underwear, as well as patients after radiation therapy.
5. Hormonal imbalance. A deficiency of female sex hormones in postmenopause plays a significant role in the appearance of true erosion. Lack of estrogens leads to thinning of the mucous membrane, decreased secretion of glands, dryness and, as a result, tissues become more vulnerable.
6. Other reasons. Immunity disorders, allergic reactions, vitamin deficiencies and lack of minerals can also contribute to the appearance of erosion.
During colposcopy, true erosion looks like an epithelial defect with clear edges and an uneven, tuberous bottom.
Normally, if you exclude the inflammatory process that supports erosion, after 1-2 weeks it begins to epithelialize.
Therefore, the main method of treatment for true erosion is to eliminate the inflammatory component. When treating true cervical erosion in postmenopause, combined treatment is used, including exclusion of the traumatic factor, anti-inflammatory and hormonal therapy.
Do not forget about a cytological examination of the cervix before treatment to exclude more serious pathologies.
More information about cervical erosion: causes, symptoms, diagnosis, treatment.
I. BACKGROUND PROCESSES
- Hyperplastic processes associated with hormonal disorders:
- a) endocervicosis (simple, proliferating);
- b) polyp (simple, proliferating, epidermal);
- c) papillomas;
- d) leukoplakia (without atypia);
- d) endometriosis.
- Inflammation:
- a) true erosion;
- b) cervicitis.
- Post-traumatic processes:
- a) ruptures;
- b) ectropion;
- c) scar changes;
- d) cervicovaginal fistulas.
III. Leukoplakia of the cervix
This is a lesion of the mucous membrane of the exocervix, consisting in thickening of the mucosa and disruption of its keratinization processes, while white films or plaques, flat or rising above the surface, form on the surface of the cervix.
Kinds
During colposcopy, three forms of cervical leukoplakia are distinguished:
- flat leukoplakia - whitish areas are on the same level with normal stratified squamous epithelium;
- warty leukoplakia - the surface of the cervix looks lumpy due to the layering of the affected areas on top of each other and their elevation above the surface;
- erosive leukoplakia - during colposcopy, in addition to leukoplakia, erosive areas or cracks are determined on the cervix in the affected area.
According to the histological conclusion, simple leukoplakia of the cervix (or without atypia) and leukoplakia with atypia are distinguished.
Simple leukoplakia is characterized by thickening of the basal and granular layer of stratified squamous epithelium and the phenomena of parakeratosis.
The reason for this process is not fully understood, but possible causes include disruption of the woman’s hormonal levels, cervical injuries, infectious and chemical factors.
Leukoplakia with atypia refers to precancerous diseases and consists of the appearance of basal cell hyperactivity and atypical cells. In 15-75% of cases it can develop into preinvasive squamous cell carcinoma.
Colposcopy in this case does not allow accurately differentiating the disease.
The only diagnostic method is cytological, or better yet, histological examination.
To do this, a PAP test or a biopsy of the leukoplakia area is performed.
If simple leukoplakia is confirmed at the histological level, no treatment is required other than observation and a PAP test once a year.
If atypical cells are detected during histological examination, the treatment method is radio wave “cauterization” of leukoplakia on the cervix on the 5-7th day of the menstrual cycle; in advanced cases, conization of the cervix is used.
The use of tampons with sea buckthorn oil, aloe and rosehip is not permissible, because provokes rapid growth of malignant cells!
Pathogenesis
The pathogenesis of cancerous, precancerous and background diseases is different and depends on what type of epithelium was damaged and what cells were involved in the process.
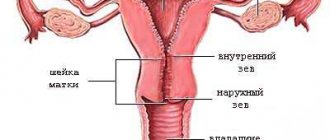
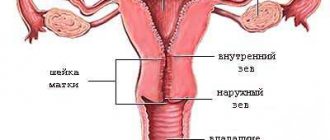
To better understand the symptoms and characteristics of your disease, as well as the principles and direction of treatment, you should learn more about the structure of the cervix. The cervix is covered with 2 types of epithelium:
- multilayer flat – vaginal part;
- single-core cylindrical - cervical canal.
In addition to the epithelium, the structure includes the stroma (the tissue of the cervix itself) and the basement membrane, which separates the epithelial cells from the stroma and consists of collagen, reticulin, argyrophilic fibers and neutral mucopolysaccharides.
Multilayer epithelium contains several types of cells, different in shape, nucleus, functionality and other parameters. They are folded in several layers:
- basal;
- parabasal;
- intermediate;
- surface.
The structure of stratified squamous epithelium and glycogen storage activity change with age because they depend on estrogen production. A greater number of layers and a maximum amount of glycogen are observed during reproductive age, the lowest in girls in the neutral period and in postmenopausal women. In postmenopause, only the basal and parabasal layers are preserved, and this is a normal variant.
The columnar epithelium that lines the cervical canal consists of only one row of columnar cells. These cells produce mucopolysaccharides, which are involved in the formation of a mucus plug in the cervical canal.
The cause of this or that deviation is a displacement of the epithelial border to the vaginal portion of the cervix, eversion of the mucous membrane of the cervical canal to the vaginal side, keratinization of multilayered squamous epithelium, its atrophy and reduction in the number of layers, the appearance of outgrowths from connective tissue, impaired cell differentiation and other processes.
The epithelial boundary in this case plays a key role - 90% of all pathologies of the cervix occur precisely there. The unspoken name for this border is the “zone of storms.” Its displacement, as indicated above, indicates the presence of pathologies. During the diagnostic process, the woman’s age should be taken into account, since as she grows older, the “storm zone” changes its location:
- in girls and adolescents - around the external os on the vaginal portion of the cervix;
- in adult women - in the area of the external pharynx;
- in postmenopause - in the cervical canal at different levels.
IV. Cervical endometriosis
According to the literature, in almost 20% of cases, cervical endometriosis is the result of diathermocoagulation. Also, some researchers include plastic surgery, abortion and childbirth as the causes of the development of cervical endometriosis. It is assumed that the endometrium penetrates into the damaged mucous membrane of the cervix, forming foci of heterotopia.
When endometriosis is localized only on the vaginal part of the cervix, the disease may be asymptomatic or accompanied by the appearance of spotting dark brown discharge before and after menstruation.
When endometriotic lesions penetrate into the mucous membrane of the cervical canal, a pain syndrome occurs, changing its intensity depending on the phase of the cycle.
During colposcopy, foci of endometriosis look like reddish cysts, up to 5 mm in size, and on the days of menstruation they increase in size and become purple-bluish.
Also, before treatment, it is necessary to conduct a biopsy of the lesions with a histological conclusion to exclude malignant processes.
The radical method of treating cervical endometriosis, as well as other forms of this disease, is surgical. On days 6-7 of the cycle, laser or radio wave destruction of the lesions is performed.
Relapse of the disease after this is extremely rare.
Diagnosis of diseases
Differential diagnosis and the correct selection of studies to identify certain diseases in the early stages is the main task of gynecology in terms of cervical diseases. You can examine the cervix in several ways, which are described above. Let’s summarize the diagnostic information into one list (you can sign up for any of these studies at the NEARMEDIC clinic):
- gynecological examination;
- Schiller's test - staining with iodine-containing preparations that reveal pathological areas without glycogen;
- colposcopy – examination of the cervix with multiple magnification using a colposcope (survey or with additional tests);
- microcolposcopy - allows you to examine the cervix with a magnification of hundreds of times to assess cell morphology;
- cervicoscopy – examination of the cervical canal using a hysteroscope (most often curettage is added);
- cytology - examination of smears (reliability 60-70%);
- morphological methods - used in extreme cases;
- PCR – detection of viruses and infections, HPV serotyping;
- Ultrasound – evaluates the structure of the mucous membrane of the cervical canal, detects polyps;
- MRI, CT, angio- and lymphography are used to clarify the diagnosis of cancer.
The listed diseases constitute a far from complete list of pathologies that can affect the cervix. As you can see, not all of them are expressed by vivid symptoms, especially in the early stages. Regular examinations, treatment of HPV and underlying diseases in the cervix allow you to maintain health and eliminate the occurrence of precancerous and cancerous processes.
V. Precancerous diseases of the cervix
According to the literature, cervical cancer ranks third among malignant diseases of the reproductive system in women. Every year, up to 500,000 new cases of cervical cancer are registered worldwide.
But cancer does not appear at lightning speed; decades pass before precancer turns into a malignant process. It can be prevented if precancerous changes are diagnosed and treated in time.
The difficulty in diagnosis lies in the fact that even a pronounced process is asymptomatic, which is why it is so important to be examined by a gynecologist at least once a year.
Many studies prove that the formation of precancerous processes begins with infection with the human papillomavirus, which subsequently disrupts the structural structure of cells, most affecting the cell nuclei.
Condylomas
According to the Bethesda system classification, they are classified as LSIL (low-grade squamous intraepithelial lesions).
Condylomas arise as a result of papillomavirus infection and are growths of connective tissue covered with stratified squamous epithelium.
There are genital and flat condylomas.
In 10% of cases, flat condylomas can become malignant within 2 years; they are invisible to the naked eye and are diagnosed during extended colposcopy.
Treatment of condylomas consists of laser surgery of the affected lesions with further antiviral and immunomodulatory therapy.
Mild dysplasia (CIN I)
Changes in cell structure affect only the lower layers of stratified squamous epithelium.
As a rule, these changes arise as a result of the inflammatory process and either disappear after anti-inflammatory therapy or regress on their own.
In 10-15% of cases they can develop into moderate dysplasia.
Moderate dysplasia (CIN II) Characterized by the fact that changes in cells affect higher layers.
In 20% of cases it progresses to CIN III, and in 5% it can develop into cervical cancer.
Severe dysplasia (CIN III) and cancer in situ In CIN III, changes in cells are characterized by the appearance of large nuclei or several nuclei in all layers of the mucosa. Only in the most superficial layers can signs of maturation and differentiation of normal cells be detected.
In case of cancer in situ, the cells do not differ in structure from cancer cells, but these changes have not yet spread beyond the mucous membrane.
Considering that different degrees of dysplasia can be combined, to clarify the stage and before treatment, it is necessary to carry out a targeted biopsy of suspicious areas followed by histological examination.
Treatment
For CIN I-II, treatment begins with anti-inflammatory drugs, followed by repeated cytological examination after 2 weeks.
Also, if a human papillomavirus infection is detected, antiviral and immunomodulatory therapy can be used in combination.
If the changes persist during repeated examination, laser coagulation of the cervix is performed as the most effective method of treatment.
This is an outpatient procedure performed on days 4-7 of the cycle. Complete epithelization of the coagulated surface occurs 4-6 weeks after the procedure.
Subsequently, dynamic observation with cytological examination is necessary every 6 months.
In case of CIN III and cancer in situ, wait-and-see tactics are unacceptable; it is necessary to immediately carry out conization of the cervix - amputation of the cervix followed by histological examination of the material.
The procedure is performed in a hospital under general anesthesia. In this case, you can use various techniques: radio wave, laser, electrosurgical or simply surgical.
The disadvantage of the laser technique is that the edges of the material become charred, which complicates further diagnosis, but the risk of bleeding is much lower than after using the surgical method.
In recent years, the radio wave or argon plasma method has been widely used using a special loop, which eliminates both of these disadvantages.
After the manipulation, clinical observation is also necessary once every 3 months.
More information about cervical dysplasia: classification, causes, symptoms, diagnosis and treatment.
Methods and methods of treatment
Modern medicine offers various methods of treating diseases of the reproductive system. First, it is necessary to identify the cause of the disease and, if possible, eliminate it. For this purpose, treatment of inflammatory processes and hormonal imbalances is carried out, and, if necessary, treatment against viruses and immunological disorders. But sometimes such measures are not enough to eliminate the disease.
MC "Diagnostics" provides the following methods of treating an organ such as the cervix:
- Chemical removal - used for superficial tissue damage and the formation of condylomas.
- Diathermocoagulation is contraindicated in nulliparous women, as it causes scarring.
- Cryotherapy (treatment with liquid nitrogen) - used for superficial tissue damage and the formation of condylomas. Does not leave scars and is painless.
- Laser therapy – removes tissue and stops bleeding. It has increased efficiency, does not leave scars, and is painless.
- Radio wave surgery – cuts off the damaged area, is safe and painless, removes tissue and stops bleeding.
- Excision of the cervix is performed for malignant tumors.
Types of pathologies
Background diseases of the cervix are a whole group of pathologies that are characterized by an altered state of the epithelial layer, although its individual cells still divide, mature and differentiate normally. This means that natural cellular processes remain intact. In contrast, precancerous conditions are characterized by dysplastic changes, in which the normal functioning of cells is disrupted. As a result, they first turn into atypical and then into malignant.
Background pathologies include:
- endometriosis;
- erosion and pseudo-erosion;
- cervicitis;
- polyps, etc.
Precancerous conditions of the cervix include:
- Dysplasia.
Characterized by uncontrolled division of cervical epithelial cells. It can occur in mild, moderate and severe forms. In approximately 60% of cases, dysplasia leads to the formation of malignant carcinomas, and in another 15% - to the appearance of microcarcinomas. - Leukoplakia.
It involves keratinization of the superficial and proliferation of the basal layers of the epithelium. Also, leukoplakia can be accompanied by severe cell atypia, which in 75% of cases gives rise to cervical cancer. - Erythroplakia.
It is diagnosed by atrophic changes within the epithelium and pathological growth of its basal layer. - Adenomatosis.
This is hyperplasia of the mucous membrane of the cervical canal, which often develops into glandular forms of cancer.
These pathologies develop on the basis of underlying diseases if they are not detected and treated in time.
Symptoms - when to seek help
There are no clinical manifestations of first-degree cervical dysplasia; it can only be detected during examination. However, in most cases, the disease occurs against the background of other ailments that have certain symptoms. Associated inflammatory processes can manifest as burning or itching, discharge of varying consistency, and contact microbleeding after sexual intercourse. Frequent accompaniments of dysplasia may be gonorrhea or chlamydia, which have specific symptoms.
Statistics show that in most cases, dysplasia is accompanied by the presence of uterine erosion, so an experienced specialist will definitely refer you for a special PAP analysis in such cases. If cervical erosion is detected during pregnancy, the diagnosis of dysplasia can be carried out using conventional methods. The first and second stages are not an obstacle to normal childbirth; in the third stage, the doctor may recommend a cesarean section.
How does an appointment with a gynecologist go?
When a patient comes to see a gynecologist, the doctor first collects anamnesis to find out how old the patient is, when the pain and irregularities in the menstrual cycle began, whether the patient is sexually active, and how menstruation occurs. This will help form a complete clinical picture before examination and testing.
How to properly prepare for the procedure. In fact, there is nothing complicated about this: you just need to wash yourself in advance and put on clean underwear. During the examination, you need to relax as much as possible and listen to the doctor’s instructions. At the initial appointment, an examination, colposcopy and smears are taken. At the follow-up appointment, the patient is given a diagnosis and a treatment regimen is prescribed.
In our center, the procedure for examining and treating cervical erosion with laser, as well as any other pathology of the cervix, is carried out as delicately as possible so that the patient feels comfortable and does not feel pain during all procedures.
Symptoms
Precancerous diseases in women are very often asymptomatic. But you should definitely consult a doctor immediately if:
- Watery discharge that appears constantly or periodically;
- Blood during or after sexual intercourse;
- Menstrual irregularities;
- Itching and burning of the genitals.
Pain is not typical for precancerous diseases. However, they can be accompanied by inflammatory processes, which leads to painful sensations in the lower abdomen.
Prevention
There are primary and secondary prevention of cervical cancer.
Primary prevention consists of preventing sexually transmitted diseases, abstaining from early sexual activity, quitting smoking, and using mechanical barrier means for contraception.
Secondary prevention of the disease consists of identifying and eliminating precancerous diseases through a systematic examination of women using additional research methods discussed above.