Sore throat, dryness, burning sensation, discomfort and sharp pain when swallowing - each of us has probably encountered these symptoms, regardless of gender and age.
It’s especially disappointing when a sudden sore throat disrupts pre-planned plans and prevents you from leading your usual lifestyle. And then there may be a desire to deal with the disease by starting treatment with antibiotics. But such therapy is indicated only if it is recommended by a doctor; self-medication can be harmful. Let's find out why.
How do antibiotics work?
With the discovery of antibiotics, humanity in the 20th century began to hope, if not for eternal life, then at least for complete relief from all diseases. But that did not happen. After all, antibiotics can only fight bacterial diseases. But they are powerless against viruses.2
This means that for acute respiratory viral infections, influenza, tonsillitis, pharyngitis, laryngitis and other diseases that cause a sore throat, antibiotics may be needed only in a small percentage of cases, and the need to take them can only be determined by a doctor.
Is it true that antibiotics do not cure everything?
- Wait! - you say. – If antibiotics are useless, why are they so often prescribed by doctors for sore throats?
No doctor, without special tests, can determine in 100% of cases whether a sore throat is caused by bacteria or viruses. Therefore, today there is a growing trend of overprescription of antibiotics throughout the world. According to statistics, 80-90% of cases of acute inflammation of the pharynx in adults are caused by a viral infection, and only 10-20% are caused by bacteria.1 The problem is that bacteria have launched a counter-offensive. By mutating, some of them have learned to become resistant to drugs. That is, when a population is exposed to an antibiotic, real natural selection occurs according to the Darwinian model. You can say: “What doesn’t kill bacteria makes them stronger.”
In this way, resistance can develop - the immunity of bacteria to antibiotics. What could this lead to?
Why is antibiotic resistance dangerous?
According to WHO experts, antibiotic resistance is one of the most serious threats to human health, food security and development today.1
And this problem can only be dealt with by refusing to take antibiotics “just in case,” for prevention, or hoping to quickly get rid of unpleasant symptoms. Taking antibiotics for a sore throat in the absence of bacterial diseases, you will not help yourself, but on the contrary, you can harm. Remember: in many cases, symptomatic treatment can help with a sore throat.
Rating of the best moisturizing sprays
Preparations with sea water and vegetable oils eliminate dry mucous membranes, which prevents the proliferation of pathogens.
The best sprays with a moisturizing effect:
- Aqualor. A popular remedy for the quick and safe treatment of oropharyngeal diseases. Contains Atlantic water, chamomile and aloe extract. The drug eliminates swelling of the mucous membranes and promotes the restoration of damaged tissues. Advantages – safe for small children, pregnant and lactating women.
- Aqua Maris. A seawater-based spray relieves inflammation and prevents the development of complications. Advantages – safety, efficiency. Disadvantages - price.
- Cameton. The spray contains camphor, eucalyptus oil and levomenthol. Combined medicine, antiseptic, removes signs of inflammation, moisturizes mucous membranes, improves sputum discharge. Advantages – convenient attachment, improvements are noticeable after 2-3 days of use, price. Disadvantages – not suitable for treating children under 5 years of age, specific taste.
- Inhalipt. A drug with the best price-quality ratio. The spray fights bacteria, relieves pain and soreness, and moisturizes the mucous membrane. Advantages - high efficiency, convenient sprayer, reasonable cost. The disadvantage is the pronounced taste of mint and eucalyptus.
- Argento-sept. A spray with an antibacterial and moisturizing effect, it relieves even severe pain and swelling of the tonsils. Advantages: safety, fast action, pleasant aftertaste. The disadvantage is the price.
Moisturizing sprays can be used for prevention during epidemics of colds.
What diseases cause a sore throat?
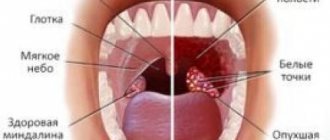
Unpleasant sensations of scratching, rawness, a feeling of a foreign body in the throat, pain when swallowing food - all these symptoms can accompany pharyngitis, tonsillitis and laryngitis. These viral diseases are quite common, they lead to discomfort in the throat and can disrupt many of our plans.
Pharyngitis is an acute or chronic inflammation of the mucous membrane of the pharynx, most often of a viral nature. That is, it makes no sense to treat it with antibiotics; symptomatic treatment would be appropriate. Tonsillitis is an inflammation of the palatine tonsils (they are also called tonsils), and laryngitis is an inflammation of the mucous membrane of the larynx and vocal cords, often of a viral nature. Symptomatic therapy is also successfully used in the treatment of these diseases.
Antibacterial drugs for these diseases are required in 5-15% of cases when the cause of the disease is streptococci.2 To determine the pathogen, a bacteriological examination of a throat smear is necessary, the result of which may take some time, sometimes up to several days. Therefore, for a sore throat, in many cases, the doctor may recommend symptomatic local therapy that helps combat the discomfort.
Antibacterial therapy for acute infections of the ENT organs
AND
Infectious diseases of the ENT organs are a very large group of inflammatory diseases, each of which a person experiences several times in life.
This group includes inflammatory diseases of the paranasal sinuses (rhinosinusitis), pharynx and tonsils (tonsillopharyngitis, tonsillitis) and middle ear (otitis). The significance of these diseases is determined by their extreme prevalence, especially in childhood. Thus, in the United States, 31 million cases of acute rhinosinusitis (ARS) are registered annually. According to estimates, in Russia 10 million people suffer from ARS annually
, but this figure also looks underestimated, since it takes into account only severe manifest forms. According to the National Center for Disease Statistics in the United States, costs associated with the diagnosis and treatment of ARS in 1996 amounted to $5.8 billion.
Acute otitis media (AOM) is one of the most common childhood diseases
. By the age of three, 71% of children experience AOM, and in the first 7 years of life, up to 95% of children have a history of at least one episode of this disease [10,11]. According to the HMO (Health Maintenance Organization), 48% of children have single episodes of acute perforated or non-perforated otitis media in the first 6 months of life or more than 2 episodes in 12 months of life.
There is no exact information about the prevalence of sore throats and acute tonsillopharyngitis (ATP), but it is clear that these are also one of the most common human infectious diseases. In adults, damage to the palatine tonsils is typical; in children, adenoiditis, an inflammation of the pharyngeal tonsil, is more common. In early childhood (up to 3 years) and in old age (after 50 years) the incidence of sore throats is lower, which is associated, respectively, with age-related imperfections or age-related involution of the lymphoid tissue of the pharynx.
The pathogenesis of ARS, AOM and ATP is based on an inflammatory reaction, which usually develops against the background of an acute respiratory viral infection (ARVI). Viral infection of the mucous membrane is the first phase of the disease. Studies using computed tomography and magnetic resonance imaging have shown that 90% of patients with ARVI develop catarrhal inflammation of the mucous membrane in the paranasal sinuses and there is stagnation of secretions [6]. This actually means that catarrhal sinusitis of viral etiology, along with rhinitis, laryngitis and laryngotracheitis, is one of the typical manifestations of ARVI. However, only 2% of patients develop secondary purulent inflammation caused by the addition of a bacterial infection, the conditions for which arise in the mucous membrane damaged by the virus. Under conditions of normally functioning mucociliary transport, bacteria are not able to contact the epithelial cells of the nasal cavity for a long enough time. When affected by a virus, the cilia of the mucous membrane cannot work at full strength, and the speed of mucociliary transport is significantly reduced. In conditions of stagnation of secretions and a decrease in the partial pressure of oxygen in the paranasal sinuses, optimal conditions are created for the development of bacterial infection.
Streptococcus pneumoniae is considered the main causative agent of ARS.
and
Haemophilus influenzae
: they are cultured from the sinuses in approximately 70–75% of patients [2,6].
Other pathogens include Moraxella catarrhalis, Staphilococcus aureus, Streptococcus pyogenes, Streptococcus viridans,
etc. Anaerobic bacteria are detected in MS in 4–11% of cases, and the main ones are anaerobic streptococci. However, the spectrum of ARS pathogens can vary significantly depending on geographic, socioeconomic and other conditions.
A similar mechanism underlies the pathogenesis of AOM, with disruption of the patency of the auditory tube playing a leading role in the development of the disease. It leads to the creation of negative pressure in the tympanic cavity and extravasation of fluid. The resulting exudate is initially sterile, but after pathogenic bacteria enter the tympanic cavity, it becomes inflammatory in nature. The results of a microbiological study of punctate tympanic cavity indicate that, as with ARS, the main causative agents of AOM are Streptococcus pneumoniae and Haemophilus influenzae
- precisely those microorganisms, various strains of which populate the nasopharynx in most children.
These two microorganisms together account for approximately 60% of bacterial pathogens [7,11]. Less commonly sown are Moraxella catarrhalis
(3–10%),
Streptococcus pyogenes
(2–10%), and
Staphylococcus aureus
(1–5%).
About 20% of cultures from the tympanic cavity turn out to be sterile. A significant proportion of AOM have a viral etiology. Mycoplasma pneumoniae
, which, in particular, can cause bullous hemorrhagic myringitis,
Chlamydia trachomatis
and
Chlamydophila pneumoniae
, may have a certain role in the etiology of AOM .
Approximately 70% of ATF are caused by viruses (rhinoviruses, coronaviruses, respiratory syncytial virus, adenovirus, influenza and parainfluenza viruses), of which rhinoviruses are the most common pathogen. The main bacterial causative agent of sore throats and ATF is considered to be group A b-hemolytic streptococcus (GABHS), the presence of which is confirmed in approximately 31% of patients [9]. Among other possible pathogens, hemolytic streptococci of other groups, Staphylococcus aureus, Enterobacteriaceae, and Haemophilus influenzae are mentioned.
There are several specific forms of OFT, among which the following are important. Acute epiglottitis is an inflammation of the lymphoid tissue of the epiglottis. The causative agent of the disease is often Haemophilus influenzae
type B, less often -
S. pneumoniae, S. aureus
and a number of other pathogens. The disease is manifested by high fever, severe sore throat, and sometimes difficulty breathing. When examined with a laryngeal mirror or endoscope, a sharply enlarged edematous epiglottis is visible; foci of abscess formation are often visible under the mucous membrane. In severe cases, a sharply enlarged epiglottis occupies the entire lumen of the laryngopharynx and leads to the development of laryngeal stenosis, which may require tracheostomy.
Sore throat of the lateral (tubopharyngeal) ridges of the pharynx
develops more often in people who have previously undergone tonsillectomy. In this case, there is compensatory hyperplasia of the tubopharyngeal ridges, which combine the tubal tonsils and accumulations of lymphoid tissue in the lateral walls of the pharynx, which, when inflamed, are brightly hyperemic, swollen, and contain small abscesses visible through the mucous membrane. The clinical picture is almost no different from ordinary tonsillitis, with the exception of the characteristic irradiation of pain in the ears due to the involvement of the tubal tonsils.
Adenoiditis
– inflammation of the pharyngeal tonsil usually occurs in children and is manifested by difficulty in nasal breathing, drainage of mucopurulent discharge along the back wall of the pharynx, and cervical lymphadenitis. Posterior rhinoscopy or, more precisely, endoscopy of the nasopharynx allows us to establish the correct diagnosis.
Main goals of treatment
for infections of the ENT organs are:
- reducing the duration and severity of symptoms of the disease;
- prevention of the development of complications (orbital, intracranial, rheumatic fever, phlegmon and abscesses);
- eradication of the pathogen.
From this point of view, the main method of treating infections of the ENT organs is systemic antibiotic therapy
, which is based on knowledge of typical pathogens or on culture sensitivity testing of specific microorganisms isolated from the affected sinus, pharynx or middle ear cavity. Although microbiological testing plays a role in selecting the optimal antibiotic, in most cases this choice is empirical. The choice of an antibiotic aimed at a specific pathogen identified during a bacteriological study does not at all guarantee success due to the high probability of “traveling” microflora entering the test material during sampling [2]. In addition, the clinical picture of moderate and severe infections dictates the need for systemic administration of antibiotics, without waiting for the results of a microbiological study, which takes several days.
Direct bacterioscopy can to some extent suggest the type of pathogen. The presence of chains or pairs of small gram-positive cocci in the preparation indicates that the probable causative agent is streptococcus (pneumococcus), large gram-positive cocci - staphylococcus. The detection of gram-negative bacteria usually indicates the presence of Haemophilus influenzae, and various microorganisms - a mixed aerobic-anaerobic infection. When choosing an antibacterial drug, the sensitivity of typical pathogens to it is of paramount importance: S. pneumonia
and
H. influenzae
.
The growing resistance of these microorganisms to many major antibiotics in recent years is a major problem in the rational antibiotic therapy of bacterial infections. Already, almost 5% of H. influenzae
in Russia are not sensitive to unprotected penicillins [3].
Acute rhinosinusitis
. The effectiveness and appropriateness of antibiotic therapy for ARS is often critically debated, and placebo-controlled studies often yield conflicting results. This is due to two main factors:
- predominantly viral etiology of the disease;
- a pronounced tendency towards spontaneous recovery.
Two recent studies found no statistically significant differences at all between doxycycline and placebo and amoxicillin and placebo in the treatment of ARS. In the last mentioned study, the clinical effectiveness of amoxicillin was 83%, and placebo was 77% [8]. In this regard, it is believed that not all ORS are subject to antibiotic treatment, but only their moderate and severe forms.
. Since additional research methods (RG, CT, ultrasound and diaphanoscopy) do not allow differentiating viral and bacterial damage to the SNP and are not indicators of the severity of the disease, the main criteria when deciding whether to prescribe an antibiotic are the patient’s general condition and complaints, medical history and the presence of purulent discharge in nasal passages.
From a clinical point of view, signs of ARS caused by typical pathogens ( S. pneumoniae
and
H. influenzae
), are the presence of fluid level on the x-ray, decreased sense of smell and good response to traditional therapy. Distinctive features of ARS caused by other microorganisms are the presence of foul-smelling nasal discharge, a total decrease in pneumatization of the SNP on an x-ray, and a slower positive dynamics of the x-ray picture during treatment [5].
Microbiological examination of the contents of the paranasal sinuses does not always reveal the true causative agent of ARS, and the results of an in vitro
do not always correlate with the clinical effectiveness of specific antibiotics.
The reasons for this may be a significant increase in antibacterial activity as a result of the unidirectional effect of the antibiotic and its metabolite and the ability of the drug to specifically achieve bactericidal concentrations at the site of infection. These qualities are characteristic of macrolide antibiotics
, in particular clarithromycin, the clinical effectiveness of which significantly exceeds the results of laboratory sensitivity testing.
Taking into account the range of typical pathogens and Russian data on their antibiotic resistance, the drug of first choice for ARS is amoxicillin
. An adequate dose for adults is 3–3.5 g/day, for children – 80–90 mg/kg/day; The daily dose is divided into three doses, regardless of food. The effect of empirical antibiotic therapy should be monitored, and the criterion of effectiveness is, first of all, the dynamics of the main clinical manifestations of the disease (headache, discharge, nasal congestion) and the general condition of the patient. If there is no noticeable clinical effect after three days, amoxicillin should be replaced with an antibiotic active against penicillin-resistant pneumococci and b-lactamase-producing strains of Haemophilus influenzae. In this case, if treatment is carried out on an outpatient basis, amoxicillin-clavulanate is prescribed orally. For young children, the drug is prescribed in powder form for the preparation of a suspension. Another treatment option is cephalosporins, particularly cefuroxime axetil.
In addition to amoxicillin and cephalosporins, modern macrolides, for example, clarithromycin (Fromilid)
, which is the drug of choice for intolerance to penicillin drugs, when cephalosporins cannot be prescribed due to the possibility of cross-allergy. Research in recent years shows that in terms of clinical effectiveness and eradication of bacterial pathogens, clarithromycin is in no way inferior to protected penicillins and cephalosporins. In addition, clarithromycin has been found to have immunostimulating properties. In particular, it increases the phagocytic activity of neutrophils and macrophages, increases the degranulation of phagocytes, the bactericidal activity of leukocytes, and also increases the activity of T-killers.
Clarithromycin has a local anti-inflammatory effect, which is due to inhibition of cytokine production, reduction of hypersecretion of mucus and sputum in the respiratory tract and sputum viscosity. These properties of clarithromycin may have an additional effect (in addition to antibacterial) in the treatment of chronic infections of the ENT organs, such as otitis media, sinusitis.
Most studies report that clarithromycin is well tolerated. According to summary data from controlled studies, when treated with clarithromycin, adverse events were observed in 19.6% of patients, among whom nausea (3%), diarrhea (3%), dyspepsia (2%), abdominal pain (2%), headache pain (1%). Comparative studies showed that the frequency of side effects when using clarithromycin was the same as azithromycin, roxithromycin, amoxicillin and lower than erythromycin.
Fromilid (clarithromycin) is available in tablets for oral administration (250 and 500 mg). In adults with acute tonsillopharyngitis, clarithromycin is prescribed orally at a dose of 250 mg every 12 hours; The duration of treatment is 10 days. For more severe sinusitis and suspected or documented H. influenzae
, it is advisable to increase the dose of clarithromycin to 500 mg every 12 hours. In children, clarithromycin is prescribed at the rate of 7.5 mg/kg 2 times a day.
If the patient is hospitalized and the intramuscular route of administration is preferable, it is possible to prescribe an inhibitor-protected antibiotic of the penicillin group - ampicillin-sulbactam or cephalosporins: cefotaxime or ceftriaxone. The optimal drugs for intravenous administration are amoxicillin-clavulanate, clarithromycin and cephalosporins.
The drugs of second choice, which are prescribed in case of ineffectiveness of the first course of anibiotic therapy, are currently fluoroquinolones of the III–IV generations: levofloxacin, moxifloxacin, sparfloxacin. The spectrum of antimicrobial action of this group of drugs is maximally adapted to pathogens of upper respiratory tract infections, and their calculated bacteriological effectiveness approaches 100%, which is confirmed by studies conducted in Russia. When developing new fluoroquinolones, the disadvantage of drugs of the 1st–2nd generation was eliminated - low effectiveness against S. pneumonia
, characteristic, in particular, of ciprofloxacin. The main side effect of fluoroquinolones of the III–IV generation is their negative effect on growing connective and cartilage tissue, therefore these drugs are contraindicated in children and adolescents. In this situation, modern macrolide antibiotics again become second-line drugs in patients under 16 years of age.
Acute otitis media
. Not all forms of AOM require the prescription of antibiotics, since with an uncomplicated course of this disease, 80–90% of children recover without antibiotic therapy. In these cases, it is sufficient to prescribe analgesics, topical drugs, thermal procedures, toileting and anemia of the nasal mucosa. With a decrease in temperature, a decrease in ear pain and symptoms of intoxication, you can limit yourself to symptomatic therapy. Patients with AOM who are not receiving systemic antibiotic therapy should be monitored by a physician so that if there is no clinical improvement within the first 24–48 hours, there is an opportunity to re-evaluate and adjust treatment accordingly. It is considered mandatory to prescribe antibiotics in all cases of AOM in children less than two years old (with an otoscopically confirmed diagnosis!), as well as in patients with immunodeficiency conditions [1]. Treatment with antibiotics reduces the risk of developing mastoiditis and intracranial complications of AOM.
As with ARS, the initial choice of antibiotic for AOM is usually empirical. The standard protocol for antimicrobial therapy outlined in many clinical guidelines differs little from what has been said about the treatment of ARS. Taking into account typical pathogens and Russian data on antibiotic resistance, the drug of first choice for AOM is amoxicillin. An adequate dose for children is 80–90 mg/kg/day, for adults – 3–3.5 g/day, divided into three doses, regardless of food. If there is no sufficient clinical effect after three days, amoxicillin should be replaced with an antibiotic active against pneumococci with a high level of penicillin resistance and b-lactamase-producing strains of Haemophilus influenzae: either amoxicillin-clavulanate or cephalosporins (cefuroxime axetil orally or ceftriaxone intramuscularly once a day in three days).
Acute tonsillopharyngitis/tonsillitis
. Antibacterial therapy for these diseases has the following goals:
- reducing the severity of symptoms of the disease and its duration;
- reducing the risk of developing rheumatic fever;
- reduction in the frequency of purulent complications (peritonsillitis, neck phlegmon);
- prevention of the spread of streptococcal infection.
Patients with a sore throat, runny nose, cough, pharyngeal congestion and no fever usually have a viral infection, for which there is no need to prescribe antibiotics. The decision to prescribe systemic empirical antibiotic therapy for ATF is based on the presence of four main clinical criteria of the disease:
plaque on the tonsils, soreness of the cervical lymph nodes, fever and lack of cough. In patients with exudative ATP, fever and cervical lymphadenitis in the absence of cough (3–4 mentioned signs), systemic antibiotic administration is indicated due to the high probability of GABHS infection. If 1 or 2 of the mentioned signs are present, antibacterial therapy is prescribed only if the culture result is positive or the rapid analysis is positive. The latest method for diagnosing GABHS infection is based on the identification of streptococcal antigen in throat swabs by enzymatic or acid extraction of the antigen followed by its agglutination, demonstrating the formation of an antigen-antibody complex.
Antibacterial therapy for ATF is aimed at eradicating the main causative agent of sore throats and metatonsillar complications - GABHS. The drug of choice is phenoxymethylpenicillin [4,12], the advantages of which are a narrow and targeted spectrum of action, good tolerability, minimal impact on the normal microflora of the gastrointestinal tract and low price. For recurrent tonsillitis/OPT, treatment is recommended to begin with amoxicillin-clavulanate or macrolide antibiotics (azithromycin, clarithromycin, midecamycin), which provide at least an equal percentage of eradication of the pathogen. Eradication of GABHS is usually achieved by oral administration of cephalosporins, however, their wider spectrum of action and stronger effect on the normal intestinal microflora place them in the category of alternative drugs. In case of clinical ineffectiveness of the first course of empirical antibiotic therapy, microbiological examination of throat swabs and determination of the sensitivity of the identified pathogen is necessary. In case of severe clinical symptoms and symptoms of intoxication, parenteral administration of antibiotics is indicated.
It is known that GABHS causes no more than a third of ATF and its presence in the pharynx does not always correlate with the severity of the clinical picture. In only 30–50% of people, microbiological identification of GABHS in the pharynx is confirmed by clinical manifestations
. In this regard, the American Academy of Pediatric Infections does not recommend repeated courses of antibiotic therapy for patients in whom GABHS is cultured from the throat. The only exceptions are children with a family history of rheumatism [12]. The variety of forms of inflammatory diseases of the pharynx and their causative agents makes it justified to prescribe drugs with a wider spectrum of antimicrobial action than penicillin - primarily modern macrolides (clarithromycin).
Treatment of laryngeal sore throat (epiglottitis) requires special attention.
To prevent the development of laryngeal stenosis, urgent hospitalization and parenteral administration of cephalosporins (cefotaxime, ceftriaxone) or amoxicillin-clavulanate are required. If there is obvious abscessation of the epiglottis (it is confirmed by indirect laryngoscopy), it is necessary to open the abscess with a laryngeal knife. Literature:
1. Kosyakov S.Ya., Lopatin A.S. Modern principles of treatment of acute otitis media, prolonged and recurrent acute otitis media. RMJ 2002; 10, No. 20: 903–909.
2. Lopatin A.S. Acute inflammatory diseases of the paranasal sinuses. Clinician's Handbook 2002; No. 1: 29–32.
3. Strachunsky L.S., Kamanin E.I., Tarasov A.A. The influence of antibiotic resistance on the choice of antimicrobial drugs in otorhinolaryngology. Consilium Medicum 2002: 3, no. 8: 352–357.
4. Strachunsky L.S., Kozlov S.N. Modern antimicrobial therapy. Guide for doctors. CD. – 2002.
5. Tarasov A.A. Features of the clinical picture and rationale for the choice of antibiotics for acute bacterial sinusitis of various etiologies. Author's abstract. dis. Ph.D. honey. Sci. Smolensk, 2003.
6. Antimicrobial Treatment Guidelines for Acute Bacterial Rhinosinusitis / Sinus and Allergy Partnership. Otolaryngol. Head Neck Surg 2000; 123, N1, Part 2: S1–S32.
7. Bergeron MG, Ahroheim C, Richard JE et al. Comparative efficacies of erythromycin–sulfisoxazole and cefaclor in acute otitis media: a double blind randomized trial. Pediatr Infect Dis J 1987; 6:654–660.
8. van Buchem FL, Knottnerus JA, Schrijnemaekers VJ, Peeters MF. Primary–care–based randomized placebo–controlled trial of antibiotic treatment in acute maxillary sinusitis. Lancet 1997; 349:683–687.
9. Dagnelie CF. Sore Throat in General Practice. A Diagnostic and Therapeutic Study. Thesis. Rotterdam, 1994.
10. Daly KA, Brown JE, Lindgren BR et al. Epidemiology of otitis media onset by six months of age. Pediatrics 1999; 103:1158–66.
11. Healy GB. Otitis media and middle ear effusions. In: Ballenger JJ, Snow JB, Ed. Otorhinolaryngology: Head and Neck Surgery. 15th edition. Baltimore: Williams & Wilkins, 1996: 1003–1009.
12. Principles of appropriate antibiotic use for acute pharyngitis in adults: Background. Ann Emerg Med 2001; 37: 711–719.
How to properly treat a sore throat?
To relieve a sore throat, choose Strepsils® Intensive (honey-lemon lozenges), which contain flurbiprofen, a medicine that has an analgesic effect.
The drug has a local analgesic and anti-inflammatory effect on the mucous membrane of the mouth and throat: it reduces swelling, difficulty swallowing, pain and irritation in the throat4.
The drug does not contain antibiotics and, accordingly, does not increase the risk of developing resistance. The product contains natural honey. Strepsils® Intensive (honey-lemon lozenges) help eliminate sore throat in infectious and inflammatory diseases of the oral cavity and pharynx, regardless of the cause (be it viruses, bacteria or fungi).
Tantum Verde
The active substance of this throat spray is benzydamine, which is a non-steroidal anti-inflammatory drug. "Tantum Verde" relieves inflammation, provides local anesthesia and is a broad-spectrum antiseptic. Tantum Verde throat spray can be used in adults and children over 3 years of age. Tantum Verde throat spray is a convenient plastic bottle with a thin spout that can be folded. To spray the liquid, just press the green pump on top - the solution is sprayed in a stream. This throat spray has a sweetish, herbal, slightly bitter taste. You can spray your throat with Tantum Verde every one and a half to three hours (although the dosage differs depending on age). The undoubted advantage of Tantum Verde, in addition to its effectiveness, is its economical consumption - this throat spray lasts for a long time. If the process is not started, you can completely cure your throat in three days. Tantum Verde is usually well tolerated, but sometimes a dry throat or burning sensation may occur.
Tantum Verde
Angelini, Italy
Tantum Verde is a non-steroidal anti-inflammatory drug for topical use.
The active substance is benzydamine hydrochloride, a derivative of indozoles. When used locally, it has anti-inflammatory and analgesic properties due to the suppression of prostaglandin synthesis and stabilization of cell membranes. It is well absorbed through mucous membranes and accumulates in inflamed tissues. Eliminated by the digestive system (with feces) and the kidneys (with urine). from 207
5.0 2 reviews
1482
- Like
- Write a review