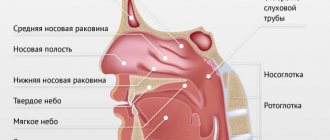
Hypertrophic pharyngitis is one of the varieties of the chronic form of the disease. It usually begins to appear 6-8 months after acute inflammation was diagnosed, which was not properly treated. The hypertrophic form of pathology affects not only the posterior wall of the pharynx, but also its lateral parts.
With pathology, the mucous membrane of the pharynx not only becomes thicker, but its density also increases. These changes are pathological, and as a result, it begins to function incorrectly and becomes inflamed. Also with this disease, the appearance of lymphoid granules is noted, which look like pink grains. The disease can appear in people of any age, but more often affects adults, since they often do not properly treat the acute form of the disease and suffer it on their feet. Gradually, disruption of the pharyngeal mucosa can also spread to the uvula. Hypertrophic pharyngitis symptoms increase as the damage to the mucous membrane progresses.
Causes
The disease develops against the background of the fact that negative factors cause excessive activity of the immune system, due to which it begins to provoke the development of a number of neoplasms on the mucous membrane, associated with the detection of even minor pathogens. As a result, inflammation develops and tissue changes occur. The main factors causing hypertrophic pharyngitis, in addition to its advanced acute form, are the following:
- living in areas with unfavorable environmental conditions;
- working in hazardous industries in violation of safety rules;
- long regular stay in a room in which the air is very dry and warm;
- smoking – not only active but also passive smoking has a negative effect on the mucous membrane and the body as a whole;
- abuse of alcoholic beverages - even not strong ones, they irritate and damage the tissues of the pharynx, making them more susceptible to pharyngitis;
- diseases of the cardiovascular system, in which blood circulation in the tissues of the pharyngeal mucosa is disrupted, as well as those that lead to congestion in the respiratory system;
- serious metabolic disorders, especially against the background of pathologies of the endocrine system;
- regular occurrence of allergies;
- disturbances in the structure of the pharynx;
- constant significant lack of vitamins.
Chronic pathologies of the nasopharynx, such as tonsillitis, sinusitis and rhinitis, can also cause the disease. Pathogenic bacteria will abundantly penetrate the mucous membrane and remain dormant in it until factors unfavorable for the immune system appear. When they develop an exacerbation of the disease.
Sore throat: possible causes, diagnosis and treatment
Sore throat is a common complaint of patients when visiting an otolaryngologist, therapist, pediatrician and general practitioner. The causes of sore throat can be infectious and inflammatory diseases of bacterial and viral etiology, inflammatory processes in the pharynx, larynx and surrounding organs caused by non-infectious factors, and non-infectious pathology (
). Before proceeding with pharyngoscopy, it is necessary to carefully detail the patient’s complaints and collect an anamnesis. The patient can call a sore throat the unpleasant sensations of scratching, burning, soreness, rawness, the feeling of a “foreign body,” the intensity of which is conveniently assessed on a 10-point scale, where the maximum manifestation of pain is rated at 10 points, the minimum at 1 point.
It is important to determine what, in the patient’s opinion, preceded the onset of pain and what other symptoms it is accompanied by. If there is hyperthermia, then the inflammatory nature of the disease is most likely: pharyngitis, tonsillitis (tonsillitis) [16]. Refusal of food and water can provoke severe pain in aphthous stomatitis (Fig. 2), tonsillitis of the lingual tonsil, paratonsillar and retropharyngeal abscess, Ludwig's angina (phlegmon of the floor of the mouth). With these diseases, drooling is possible, and inflammation of the paramygdaloid tissue and tissues of the floor of the mouth leads to trismus of the masticatory muscles (inability to open the mouth), a forced position of the head tilted to the painful side.
The occurrence of such a condition requires immediate contact with a medical specialist to sanitize the area of inflammation. Epiglottitis, an inflammation of the epiglottis caused by Haemophilus influenzae (more common in young children), gives similar symptoms. Along with refusal to eat, salivation, pain and hyperthermic symptoms, epiglottitis is accompanied by voice disturbance (it becomes dull, hoarse) and difficulty breathing. There is a forced position of the patient in a sniffing position, as if holding porridge in the mouth, the mouth opens freely, but a rough examination of the pharynx with a spatula can lead to laryngospasm and death. Therefore, with the above symptoms, pharyngoscopy is performed carefully; during it, you can see a hyperemic, edematous epiglottis behind the root of the tongue.
Other causes of sore throat accompanied by sore throat and cough can be in children and young people: drainage of discharge from the nasopharynx due to adenoiditis or sinusitis; irritation of the respiratory tract by dry air, smoke, including active and passive smoking; childhood infectious diseases [9]. In adults, a common cause of such complaints, often with a feeling of a lump in the throat, a “foreign body,” is an exacerbation of chronic pharyngitis associated with pathology of the gastrointestinal tract: gastritis, esophagitis, gastroesophageal reflux, cholecystitis, gastric ulcer. Severe dysphagia, regurgitation and pain when swallowing can be caused by esophageal varices [14].
A carefully collected anamnesis allows us to find out the dynamics of complaints, the time of their appearance, the connection with a previous injury or medical examination (gastroscopy), foreign body entry, contact with an infectious patient, hypothermia (drinking cold beer, ice cream), occupational or household hazards (irritants, dust , hot air, taking concentrated solutions of vinegar, spices, medications: corticosteroids, antibiotics, diuretics, local decongestants and others). Sore throat can occur as a manifestation of sexually transmitted diseases: gonococcal pharyngitis, syphilis, chlamydia of the respiratory tract. Infection with the human immunodeficiency virus contributes to the formation of inflammatory viral, tumor and mycotic lesions of the mucous membranes [3].
Chronic pathology of the kidneys, endocrine system, blood, previous radiation and chemotherapy can lead to the formation of a chronic inflammatory and atrophic process in the pharynx. The first manifestation of hyperglycemia [5] may be thirst and dry mouth, accompanied by catarrhal changes in the pharynx. Similar complaints occur with Itsenko–Cushing syndrome [5]. In patients with hypothyroidism, swallowing is often impaired, speech becomes slurred due to swelling and dryness of the tongue and lips, and it is difficult to perform pharyngoscopy.
Non-infectious pathology of the organs of the neck and chest cavity - angina pectoris, myocardial infarction - can manifest itself as intense pain in the pharynx and behind the sternum. Long-lasting dysphagia and unpleasant sensations in the form of a lump or foreign body in the throat, which are not amenable to anti-inflammatory therapy, can cause [14] tumors of the larynx, laryngopharynx, thyroid gland, and pharyngoesophageal (Zencker) diverticula. Many days of fasting, dieting, dyspepsia and heavy menstruation lead to a deficiency of vitamins and minerals. Vitamin A deficiency [5] causes dryness and erosion of the mucous membranes.
Vitamin B2 deficiency produces a triad of symptoms: dermatitis, cheilitis and glossitis (bright red, smooth and shiny dry tongue), accompanied by burning and pain in the mouth when talking and eating. Vitamin C hypovitaminosis occurs with dietary deficiency of ascorbic acid, inflammatory processes in the intestines and is manifested by pain, hemorrhagic and ulcerative-necrotic manifestations in the oral cavity and in the area of the palatine tonsils, mobility and tooth loss. Similar changes in the oral cavity and pharynx give rise to blood diseases (leukemia). Against the background of iron loss (with hyperpolymenorrhea), Plammer-Vinson syndrome is formed, characterized by superficial glossitis, dysphagia, cracks in the corners of the mouth, nail dystrophy, seborrheic dermatitis of the face, blepharitis, conjunctivitis, and decreased vision at dusk. B12 deficiency anemia associated with impaired absorption of this vitamin in the stomach due to anacid gastritis, tapeworm infestation, or increased consumption in pregnant women, manifested by Möller-Gunter glossitis (bright red tongue with smoothed papillae) and atrophy of the pharyngeal mucosa, burning pain in the tongue, weakness, crawling sensation in the limbs. A blood test reveals macrocytes, megalocytes, hyperchromic anemia, leukopenia.
Diseases of the spine [2] (cervical osteochondrosis, tuberculous spondylitis, radiculitis) can cause pain in the pharynx. Neuralgia of the glossopharyngeal nerve manifests itself as intense pain in the pharynx, especially against the background of chronic stress in anxious and suspicious patients. Metabolic disorders, intoxication, and trauma contribute to its occurrence. Characterized by unilateral pain in the root of the tongue, tonsil, lasting several minutes, accompanied by dry throat and subsequent hypersalivation. The therapeutic effect is achieved by lubricating the root of the tongue and pharynx with local anesthetics. Neuralgia of the superior laryngeal nerve [1, 6] gives similar symptoms, but also includes a painful dry cough and spasm of the vocal folds during inspiration [6].
Pain in the pharynx can be caused by an odontogenic process: periodontitis, teething pathology, galvanism [4, 17]. Rarely, unilateral pain in the pharynx occurs, the cause of which is the long styloid process (Eagle syndrome), accessible to palpation in the area of the palatine tonsil [15].
Rare causes of pain in the pharynx are ulcerations on the mucous membrane of tuberculous etiology [14]. In this case, there is a prolonged cough, weight loss, and swollen lymph nodes.
A final diagnosis is possible based on oropharyngoscopy. The main differential diagnosis for pain in the pharynx is between its most common causes - acute (or exacerbation of chronic) pharyngitis and sore throats caused by streptococcal infection (group A beta-hemolytic streptococcus - GABHS).
Acute pharyngitis is a viral infection of the pharynx in 90% of cases. Its main symptoms are: increased body temperature, sore throat when the throat is empty, when eating, soreness and a dry cough that does not bring relief. Patients indicate the localization of unpleasant sensations on the back wall of the pharynx. In the pharynx (Fig. 3), hyperemia of all parts is detected: the posterior wall, arches, tonsils, and there may be vesicular rashes (herpes, enterovirus). Plaques are not typical, there is often a runny nose and other catarrhal phenomena - nasal congestion, sneezing. If a rash is detected on the skin and mucous membranes, it is necessary to exclude an infectious disease - measles, scarlet fever, rubella [8]. Adenoviral infection manifests itself in the form of conjunctivitis, enlarged lymph nodes, fever, runny nose, and there may be plaque in the throat.
The disease progresses in waves: on the 7th–10th day of illness, a repeated increase in body temperature and a return of symptoms are possible. Enterovirus infection (“summer flu”) manifests itself in the form of dyspeptic, myalgic, and meningeal syndromes. Pharyngoscopy reveals bubbles on the mucous membrane of the oropharynx. In making the diagnosis of viral pharyngitis, the following help: knowledge of the epidemiological situation, dynamic observation of the patient, a variety of clinical manifestations (abdominal pain, vomiting, eye damage, meningeal symptoms, myalgia), lymphocytosis in the blood with normal ESR, lack of effect from antibacterial therapy, serological data research, polymerase chain reaction and others.
Sore throat is a general infectious disease with local manifestations in the form of acute inflammation of one or more components of the lymphadenoid pharyngeal ring, most often the palatine tonsils (tonsillitis), pharyngeal tonsil (adenoiditis), lingual tonsil, lateral ridges of the pharynx and larynx.
The classification of acute tonsillitis (according to I.B. Soldatov, 1975) involves the division into primary tonsillitis: catarrhal, lacunar, follicular, ulcerative-membranous; and secondary: for acute infectious diseases (diphtheria, scarlet fever, measles, tularemia, typhoid fever, infectious mononucleosis) and diseases of the blood system (agranulocytosis, alimentary-toxic aleukia, leukemia). There are special forms of tonsillitis [10]: viral, fungal, syphilitic.
With catarrhal tonsillitis, there is hyperemia and enlargement of the palatine tonsils, regional lymphadenitis, no plaque, a blood test shows slight leukocytosis, increased ESR. Catarrhal sore throat often has to be differentiated from viral pharyngitis, in which there is a cough, there may be a runny nose, and there is no enlargement or tenderness of the lymph nodes.
Follicular tonsillitis is manifested by bright hyperemia and swelling of the tonsils, subepithelial rounded yellowish elevations (follicles).
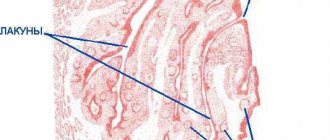
With lacunar tonsillitis, white-yellow plaques appear at the mouths of the lacunae of the tonsils (Fig. 4), which can merge with each other and cover the entire surface without going beyond the tonsils, being removed without leaving a bleeding surface, rubbing between two spatulas, dissolving in the vessel with water.
It is important to determine the streptococcal etiology of acute tonsillitis. This can be done using the McIsaac screening scale [12], which includes symptoms and their assessment in points (
).
A patient’s symptoms with a score of 3 means the probability of streptococcal etiology is 30%, and a score of 4 means about 70%. If the clinical picture is determined to be 0–1 points, then systemic antibiotic therapy is not indicated. At 2–3 points, antibiotics are necessary only if the infection is bacteriologically confirmed. Antibiotics should be prescribed when symptoms of 4–5 points are detected.
Diphtheria of the pharynx occurs in the form of localized, widespread, toxic I, II, III degrees and hypertoxic forms. With it, gray plaques are detected on the surface of the tonsils, tightly fused with the underlying tissues, they may spread to the arches, the mucous membrane of the posterior pharyngeal wall, the uvula (Fig. 5), and when you try to remove them, the mucous membrane bleeds. Plaques do not rub down and do not dissolve in water. In the toxic form, the neck is noticeably thickened due to swelling of the subcutaneous fat, pressure is painless and does not leave pits.
Infectious mononucleosis is an acute infectious disease caused by the Epstein-Barr virus, characterized by fever, sore throat, enlarged lymph nodes, pharyngeal tonsil, liver, and spleen. Plaques on the tonsils, as in lacunar tonsillitis (Fig. 6), but can spread beyond them. A general blood test (the appearance of atypical mononuclear cells), serological research methods (enzyme-linked immunosorbent assay (ELISA), Paul-Bunnel-Davidson reaction) help in diagnosing the disease.
Fungal infections of the pharynx in the form of curdled films, easily removed when scraped with a spatula, are caused mainly by yeast-like fungi of the genus Candida (about 90% of cases); less commonly, there are mold fungi of the genus Aspergillus, Penicillium [7]. C. albicans permanently or temporarily lives on human mucous membranes, skin and intestines. Factors contributing to the development of mycoses are: treatment with broad-spectrum antibacterial drugs, cytostatics and corticosteroids, diabetes mellitus, blood diseases, tumors, gastrointestinal diseases, vitamin imbalance. Candidiasis of the oral cavity, pharynx and esophagus occurs in more than 90% of AIDS patients (Fig. 7) [3].
Diagnosis of sore throats should include throat and nasal swabs for diphtheria (BL). Express determination of streptococcal antigen using test strips from the surface of the tonsils makes it possible to justify antibacterial therapy. A general blood test facilitates the differential diagnosis of primary and secondary acute tonsillitis. Opinions on the question “Should I do a smear?” controversial. It is needed to confirm the GABHS etiology of the disease in doubtful cases [16].
Therapeutic tactics for pain in the pharynx can be presented in the form of a diagram ().
For the treatment of acute pharyngitis, a gentle diet, hot foot baths, warm compresses on the front surface of the neck, warm alkaline drink (mineral water, milk with honey), steam inhalations, and smoking cessation are recommended. The attitude towards gargling is ambiguous [16]. Fresh infusions of mint, chamomile, calendula, eucalyptus, sage, and caragana are effective for relieving sore throat. Antiseptics of artificial origin (dichlorobenzene, metacresol, hexethidine, benzalkonium, thymol, ambazone, chlorhexidine) are bactericidal in their mechanism of action, which can lead to suppression of the normal microflora of the oral cavity, so they should be used with caution in children under 6 years of age [9]. For the treatment of sore throat, the most important painkillers are those containing menthol, tetracaine, lidocaine or flurbiprofen. Children from 6 months of age can use the herbal preparation Tonsilgon, which has an antiseptic and analgesic effect, but does not contain either menthol or lidocaine.
Menthol preparations and any sprays cannot be used before 3 years of age due to the possible development of laryngospasm.
Local combination drugs (antiseptics and painkillers) in the form of finished dosage forms are the most popular for the treatment of sore throat. One of them is TheraFlu LAR, a universal and highly effective local drug with an antiseptic and analgesic effect. TheraFlu LAR contains benzoxonium chloride and lidocaine. Available in the form of a spray and tablets, the content of lidocaine in which is 0–75 mg and 1 mg, respectively.
Recent in vitro and in vivo studies confirm the broad antiseptic spectrum of benzoxonium chloride and its activity against the main pathogens of the most common diseases of the oral cavity and pharynx. At the same time, the balance of the bacterial flora in the mouth is not disturbed, even with prolonged use of benzoxonium chloride.
Benzoxonium chloride has:
- bactericidal effect against aerobic and anaerobic gram-positive and gram-negative bacteria;
- fungicidal effect against Candida albicans, Aspergillus spp. and yeast fungi;
- antiviral activity against membrane viruses, including herpes virus, influenza virus, parainfluenza viruses, the causative agent of vesicular stomatitis.
Lidocaine is a local anesthetic that reduces pain in the throat when swallowing.
Adults should take the drug 1 lozenge every 2–3 hours (no more than 10 tablets per day) or as a spray, 4 sprays 3–6 times a day. Children aged 4 years and older are prescribed 1 lozenge every 2-3 hours (no more than 6 tablets per day) or as a spray, 2-3 sprays 3-6 times a day. The required duration of treatment, as a rule, does not exceed five days. The drug is well tolerated by patients, side effects are recorded extremely rarely. Possible short-term local irritation of the mucous membrane, allergic reactions.
Indications for its use are: pharyngitis, laryngitis, catarrhal tonsillitis, stomatitis, ulcerative gingivitis. Contraindications to the use of TheraFlu LAR: pregnancy (first trimester), breastfeeding, hypersensitivity to lidocaine, children under 4 years of age. TheraFlu LAR can be used by people with diabetes, as it does not contain sugar. Thanks to the combined effect - antibacterial and analgesic, TeraFlu LAR can relieve all symptoms of viral pharyngitis and be used in the complex therapy of bacterial sore throats.
Systemic antibiotic therapy in the treatment of patients with “sore throat” is indicated mainly for acute tonsillitis (angina) of suspected or established streptococcal etiology (GABHS) and is carried out with penicillins, and if they are intolerant, with macrolides; cefuroxime (Axetin) is effective. Clindamycin and lincomycin are reserve drugs [11]. Epiglottitis caused by Haemophilus influenzae is effectively treated with protected penicillins.
Literature
- Alimetov Kh. A. Secondary neuropathy of the upper laryngeal nerve / M materials of the anniversary All-Russian. scientific-practical conf. with international participation “Modern aspects and prospects for the development of otorhinolaryngology. M., September 29–30, 2005. P. 46.
- Alimetov Kh. A. Spondylogenic pharyngeal dyskinesia / Materials of the anniversary All-Russian. scientific-practical conf. with international participation “Modern aspects and prospects for the development of otorhinolaryngology. M., September 29–30, 2005. P. 22.
- Bessarab T.P., Yushchuk N.D., Anyutin R.G., Potekaev S.N. HIV infection in otorhinolaryngological practice // Attending Doctor, 2000. No. 1. P. 26–30.
- Inflammatory diseases of the mucous membrane of the pharynx, oral cavity and periodontium. Scientific review. Solvay pharma, 2002. P. 2.
- Diseases of the mucous membrane of the oral cavity and lips / Ed. E. V. Borovsky, A. L. Mashkilleyson. 1984. 400 p.
- Karpova O. Yu. Clinic, diagnosis and treatment of laryngoneurosis / Materials of the anniversary All-Russian. scientific-practical conf. with international participation “Modern aspects and prospects for the development of otorhinolaryngology. M., September 29–30, 2005. P. 53.
- Kunelskaya V. Ya., Kasimov K. On the issue of the clinic, diagnosis and treatment of candidal tonsillitis in children // Vestn. otorhinolaryngology. 1980. No. 4. P. 50–52.
- Nisevich N. I., Uchaikin V. F. Infectious diseases in children. M.: Medicine, 1985. 298 p.
- Acute respiratory diseases in children: treatment and prevention. Scientific and practical program of the Union of Pediatricians of Russia / Ed. A. A. Baranova. M., 2008.
- Otorhinolaryngology: national guide / Ed. V. T. Palchuna. M.: GEOTAR-Media, 2008. 960 p.
- Rational antimicrobial pharmacotherapy: Hand. for practicing doctors. Under general ed. V. P. Yakovleva, S. V. Yakovleva. M.: Litterra, 2003. 108 p.
- Sidorenko S.V., Guchev I.A. Tonsillopharyngitis: issues of diagnosis and antibacterial therapy // Consilium medicum. Infections and antimicrobial therapy. 2004. 4: 36–38.
- Folomeeva O. M., Amirdzhanova V. N., Yakusheva E. O. et al. Incidence of rheumatic diseases in the Russian population (analysis over 10 years) // Ter. Archive. 2002. No. 5. P. 5–11.
- Shevrygin B.V., Mchedlidze T.P. Handbook of otorhinolaryngology. M.: Triada-X, 1998. 448 p.
- Shulga I. A., Zaitsev N. V., Zaitseva V. S. Variants of the structure of the stylohyoid complex / Materials of the Anniversary All-Russian. scientific-practical conf. with international participation “Modern aspects and prospects for the development of otorhinolaryngology. M., September 29–30, 2005. P. 75.
- Etiopathogenetic therapy of diseases of the upper respiratory tract and ear: Methodological recommendations. Compiled by S.V. Ryazantsev, Kotserovets V.I. St. Petersburg: National Register, 2008. 100 p.
- Yakovleva V.I. Diagnosis and treatment of neurogenic diseases of the maxillofacial region: Textbook. manual for institutes and faculties. improved doctors. Minsk: Vysh. school, 1989. 102 p.
M. V. Subbotina , Candidate of Medical Sciences Irkutsk State Medical University , Irkutsk
Contact information about the author for correspondence
Kinds
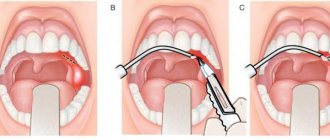
This form of the disease can have two types. Depending on which of them is diagnosed, the exact treatment method is determined. Granular hypertrophic pharyngitis affects only the back wall of the pharynx. With it, tissue swelling is not felt so much at the onset of the disease, which is why not all patients seek medical help in a timely manner.
Lateral hypertrophic pharyngitis is manifested by more acute pain and difficulty breathing. It is extremely difficult to ignore it for a long time, which is why treatment most often begins on time. The diagnosis is made after examining the patient's pharynx.
Symptoms of laryngeal cancer
There are no common signs for laryngeal cancer
, they are determined by the parameters of the tumor, its position, and growth rate. At the very beginning, it is sometimes difficult to notice a malignant formation.
Common symptoms of throat cancer
relate:
- pain in the throat, including when swallowing,
- sore throat,
- frequent bronchitis,
- hoarse voice,
- changes in the shape of the neck (swelling),
- a sharp decrease in body weight,
- discomfort in the ears.
Forecast
With timely, complete and systematic treatment of the disease, the prognosis for the patient is favorable. In this case, it is possible to stop pathological changes in the mucosal tissues. After quality therapy, exacerbations of the disease are extremely rare.
If treatment is started late, when the throat lesion is already quite serious, then the prognosis for the patient is relatively positive, since it will not be possible to ensure a long remission, but at the same time the risk of complications will be eliminated.
What does throat cancer look like: photos and pictures
For a more detailed understanding of the localization of throat cancer and the extent of its invasion into nearby organs, the tumor is usually characterized by stages:
- Stage I – asymptomatic, vocal and swallowing functions are not impaired, the tumor is discovered by chance at a routine appointment with an otolaryngologist, measuring 2–3 cm;
- Stage II is the stage of intensive tumor growth and its spread to nearby areas of the larynx. A characteristic clinical picture appears (cough, shortness of breath, change in voice, etc.). Surgical treatment at this stage consists of partial or complete resection of the larynx followed by plastic surgery;
- Stage III – metastasis, tumor growth into all layers of the larynx and complete loss of vocal cord function. As a rule, surgery at this stage does not give good results, so radiation and/or chemotherapy is added to therapy;
- Stage IV – dissemination of metastases to target organs (lungs, brain). Treatment is palliative only.
Photo of the larynx 1. Cancer of the larynx in the glottis area
Photo of the larynx 2. Stages of throat cancer (I – III)
What not to do
During the treatment period there are certain restrictions, by violating which the patient risks significantly aggravating his condition. The doctor will not be able to guarantee the patient a positive result of therapy if the following actions are allowed:
- smoking during treatment;
- use of alcohol preparations for gargling;
- eating spicy food;
- staying in a dusty room;
- violation of medical instructions regarding treatment.
If there are no violations in the course of therapy, then it is possible to stop the disease at the beginning of its development without the use of surgical methods of therapy. Treatment of hypertrophic pharyngitis in adults and children is the same.
Treatment of laryngeal cancer
There are two treatment options for throat cancer
– surgery and conservative treatment. A specific method is selected based on a combination of factors, primarily the location and size of the formation. Radiation and chemotherapy are often used initially. In most cases, in the first stages, conservative treatment gives positive results, and the larynx continues to function fully.
throat cancer treatment
Sometimes surgery may be necessary; now, for small tumors, only a small part of the larynx is cut out; in case of serious damage, the entire organ must be removed. Then you will need to restore your voice; exercises will have to be done for at least 2 months.
After recovery, it is necessary to be under the supervision of a doctor for several more years, as there is a possibility of relapse and all kinds of complications. During treatment, you should eat food rich in vitamins and microelements. You should avoid sweets, spices, spicy, fried, salty foods, because such foods affect the larynx.
Diagnostics
Only an external examination of the pharynx is not enough to identify not only the disease itself, but also the causes of its occurrence, as well as the condition of the body. Because of this, the doctor, having identified pharyngitis by eye during the initial examination, necessarily prescribes further tests to the patient, which help to obtain a complete picture of the health condition and select the most effective treatment.
1. A swab from the pharynx followed by inoculation on a nutrient medium. It is necessary to determine the composition of pathogenic microflora and its sensitivity to certain antibiotics.
2. Biochemical blood test. It requires venous blood. The study reveals the presence of antibodies to certain inflammatory agents, hormonal parameters and the presence or absence of malignant cells.
3. Clinical blood test. Blood from a finger is used. Shows the percentage of the ratio of its main components. Deviation of one or another up or down makes it possible to detect a number of pathologies.
4. General urine analysis. The study of the material allows you to accurately assess the severity of inflammation in the body, as well as whether there are any disturbances in the functioning of the kidneys against its background.
5. Biopsy of tissue of the pharyngeal mucosa. Not always prescribed. The procedure is necessary if there is a suspicion of the development of a cancer process. When examining a tissue sample, the presence or absence of malignant (cancerous) cells in the mucosa is determined.
If necessary, an electrocardiogram and x-ray of the sinus area may also be prescribed. These procedures are rarely required. They are usually carried out if complications of the disease begin to develop. In young children, an X-ray of the lungs may also be necessary, since quite often, against the background of inflammation of the larynx, pneumonia or bronchopneumonia appears quickly enough.
Diagnosis of laryngeal tumors
Methods for diagnosing throat cancer
:
- throat examination,
- palpation,
- fibrolaryngoscopy – a piece of tissue is taken with a special instrument, hard-to-reach areas of the throat are examined,
- a separate point should be the cytological and histological examination of samples taken from the throat,
- computed tomography is used to look at cartilage,
- MRI is necessary to study the folds, subglottic region and other parts,
- Ultrasound of the lymph nodes of the neck and liver is necessary if there is a danger of metastases spreading there.