The most common upper respiratory tract infections are infections of the lining of the nose (ie, rhinitis or “runny nose”), throat infections (pharyngitis), and infections of the voice box or larynx (laryngitis).
The first place where pathogenic microorganisms (usually viruses, and sometimes bacteria) settle is the nasopharynx area. The symptoms are almost always the same: sore throat, runny nose and cough. Rhinopharyngitis is the most common reason for consultation with general practitioners. This pathology is nothing more than a cold, which is an inflammation of the nasopharynx in adults and children and is mainly viral in nature. It is essentially an infectious disease that causes inflammation in the upper part of the throat and usually goes away on its own after 7 or 10 days. But what is it - nasopharyngitis?
General description of nasopharyngitis
Rhinopharyngitis (nasopharyngitis) - inflammation of the mucous membrane of the nasopharynx. It is a mild illness, most common in children aged six months to four years, but can also affect adults.
Rhinopharyngitis can be caused by more than 200 types of viruses, the most common are:
- rhinoviruses, which make up 30-80%;
- influenza viruses - 10-15%;
- adenovirus - 10-15%.
Nasopharyngitis caused by a rhinovirus is most contagious during the first three days after symptoms appear.
Most of these viruses are predominant in winter, but you can get nasopharyngitis at any time of the year.
And even if this is not a serious disease, it still needs to be treated correctly in order to get rid of it as soon as possible.
Rhinopharyngitis is mainly of viral origin, but can recur up to several times a year; in this case, it is necessary to look for an allergic cause: mites, pollen or animal dander.
Types of nasopharyngitis:
- catarrhal;
- atrophic;
- purulent;
- chronic;
- allergic;
- subatrophic rhinopharyngitis;
- rhinonasopharyngitis.
Factors that contribute to the development of nasopharyngitis include dry and damaged mucous membranes during cold periods, a suppressed immune system, stress, fatigue and an overall unhealthy lifestyle.
Treatment of acute and chronic pharyngitis
F
Aringitis is an acute or chronic inflammation of the pharyngeal mucosa, which is accompanied by pain, soreness or discomfort in the throat. Since, from an anatomical point of view, the pharynx is divided into three sections - upper (nasopharynx), middle (oropharynx) and lower (hypopharynx), inflammatory processes developing here can also be divided according to their predominant localization. However, this division will be very conditional, especially in acute pharyngitis, due to the fact that acute viral and bacterial infections diffusely affect the mucous membrane of the upper respiratory tract and are migrating, often descending in nature. Morphological changes in the mucous membrane in chronic pharyngitis usually have a predominant localization in one of the anatomical parts of the pharynx, which makes it possible to tentatively identify individual nosologies, for example, chronic nasopharyngitis.
Etiology and classification
According to the etiological factor, acute pharyngitis can be divided into viral, bacterial, fungal, allergic, traumatic (as a result of a foreign body or surgical intervention) and caused by exposure to irritating factors (hot liquid or steam, acids, alkalis, radiation, etc.). Chronic pharyngitis is usually classified not according to etiology, but according to the nature of the changes developing in the mucous membrane: catarrhal (simple), atrophic (subatrophic) and hypertrophic. These forms of chronic inflammation are often combined. Thus, the presence of diffuse atrophic changes in the mucous membrane can be combined with focal hyperplasia of the lymphoid tissue of the posterior pharyngeal wall or tubopharyngeal ridges.
| Classification of pharyngitis Spicy
Chronic
|
The most common form of acute inflammation of the pharyngeal mucosa is catarrhal pharyngitis during ARVI. It is known that approximately 70% of pharyngitis is caused by viruses, including rhinoviruses, coronaviruses, respiratory syncytial virus, adenovirus, influenza and parainfluenza viruses. The most common causative agent of acute pharyngitis is rhinoviruses. Research in recent years shows that their importance is growing rapidly, and now rhinoviruses are responsible for more than 80% of acute respiratory viral infections during autumn epidemics. Viral infection is often only the first phase of the disease, and it “paves the way” for subsequent bacterial infection. In Fig. 1 and below provide information about the main pathogens of acute pharyngitis.
Rice.
1. Bacteria and fungi - the causative agents of acute pharyngitis (according to CA Dagnelie, 1994) Viruses - the causative agents of acute pharyngitis
(in descending order of frequency):
Basic:
- Rhinoviruses
- Coronaviruses
- Adenoviruses
- Influenza virus
- Parainfluenza virus
Rare:
- Respiratory syncytial virus
- Herpes simplex viruses (types 1 and 2)
- Enteroviruses
- Coxsackie virus
- Epstein–Barr virus
- Cytomegalovirus
- AIDS virus
These generalized data, taken from foreign manuals on otorhinolaryngology and infectious diseases, are very conditional, since the concept of “sore throat”, used in English (the Russian-language analogue is acute pharyngitis or pharyngotonsillitis), is not a definition of a specific nosological form, but rather a collective term for several diseases [3–6,10]. In addition to the nonspecific form, there are other types of pharyngitis associated with specific pathogens, for example, Epstein-Barr virus in infectious mononucleosis, Yersinia enterocolitica
for yersenial and gonococcus for gonorrheal pharyngitis, as well as
Leptotrix buccalis
for leptotrichosis of the pharynx.
Clinic and diagnostics
For the clinical picture of acute pharyngitis
Characterized by soreness, dryness, discomfort and pain in the throat when swallowing (especially with an empty throat), less often - general malaise, a rise in temperature. When the tubopharyngeal ridges become inflamed, the pain usually radiates to the ears. On palpation, there may be pain and enlargement of the upper cervical lymph nodes. Pharyngoscopy reveals hyperemia of the posterior wall of the pharynx and palatine arches, individual inflamed lymphoid granules, but there are no signs of inflammation of the tonsils characteristic of angina. It should be remembered that acute pharyngitis may be the first manifestation of some infectious diseases: measles, scarlet fever, rubella measles. In some cases, differential diagnosis with Kawasaki disease and Stevens-Johnson syndrome is required.
For the clinical picture of chronic pharyngitis
An increase in temperature and a significant deterioration in general condition are not typical. The sensations are characterized by patients as dryness, soreness and a feeling of a lump in the throat, which causes a desire to cough or “clear the throat”. The cough is usually persistent, dry and easily distinguishable from the cough that accompanies the course of tracheobronchitis. Discomfort in the throat is often associated with the forced need to constantly swallow mucus in the back of the throat, which makes patients irritable, interferes with their normal activities and disrupts sleep.
With atrophic pharyngitis, the mucous membrane of the pharynx looks thinned, dry, and often covered with dried mucus. Injected vessels may be visible on the shiny surface of the mucous membrane. In the hypertrophic form, pharyngoscopy reveals foci of hyperplastic lymphoid tissue randomly scattered on the posterior wall of the pharynx or enlarged tubopharyngeal ridges located behind the posterior palatine arches. At the time of exacerbation, these changes are accompanied by hyperemia and swelling of the mucous membrane, but usually the paucity of objective findings does not correspond to the severity of the symptoms that bother patients.
Chronic pharyngitis is often not an independent disease, but a manifestation of the pathology of the entire gastrointestinal tract: chronic atrophic gastritis, cholecystitis, pancreatitis. The entry of acidic gastric contents into the pharynx during sleep with gastroesophageal reflux disease and hiatal hernia is often a hidden cause of the development of chronic catarrhal pharyngitis, and in this case, without eliminating the underlying cause of the disease, any local treatment methods provide an insufficient and short-lived effect. Smoking and tonsillectomy lead to the development of atrophic changes in the pharyngeal mucosa.
Pharyngitis often develops with constantly difficult nasal breathing. It can be caused not only by switching to mouth breathing, but also by the abuse of vasoconstrictor drops, which flow from the nasal cavity into the pharynx and have an unnecessary anemic effect there. Symptoms of pharyngitis may be present with the so-called postnasal drip (postnasal drip). In this case, discomfort in the throat is associated with the flow of pathological secretions from the nasal cavity or paranasal sinuses along the back wall of the pharynx. In addition to constant coughing, this condition can cause wheezing in children, which requires differential diagnosis with bronchial asthma.
The main factors contributing to the development of chronic pharyngitis:
- constitutional features of the structure of the mucous membrane of the pharynx and the entire gastrointestinal tract;
- prolonged exposure to exogenous factors (dust, hot dry or smoky air, chemicals);
- difficulty breathing through the nose (breathing through the mouth, abuse of decongestants);
- smoking and alcohol abuse;
- allergy;
- endocrine disorders (menopause, hypothyroidism, etc.);
- vitamin deficiency A;
- diabetes mellitus, heart, pulmonary and kidney failure.
For persistent sore throat that cannot be treated with conventional therapy, differential diagnosis is required with a number of syndromes that develop in certain systemic diseases and diseases of the nervous system. Plummer–Vinson syndrome occurs in women aged 40 to 70 years against the background of iron deficiency anemia. Sjogren's syndrome is an autoimmune disease, accompanied, in addition to severe dryness of the mucous membrane of the gastrointestinal tract, by diffuse enlargement of the salivary glands. Eagle syndrome (stilalgia) is characterized by severe, persistent, often unilateral pain in the throat caused by elongation of the styloid process, which is located on the lower surface of the temporal bone and can be palpated above the upper pole of the tonsil. A number of neuralgias (glossopharyngeal or vagus nerve) can also cause sore throat, especially in older people.
Treatment
In case of acute and exacerbation of chronic pharyngitis, not accompanied by pronounced disorders of the general condition, symptomatic treatment is sufficient, including a gentle diet, hot foot baths, warm compresses on the front surface of the neck, milk with honey, steam inhalations and gargling. Smoking should be stopped. Uncomplicated pharyngitis usually does not require systemic antibiotics. In this situation, it becomes justified to carry out not systemic, but local antimicrobial therapy, which can also be prescribed in the form of monotherapy. However, a survey conducted in Belgium showed that in general, 36% of doctors resort to prescribing antibiotics for acute respiratory viral infections and pharyngitis [7]. This article will discuss drugs for the local treatment of acute and chronic pharyngitis.
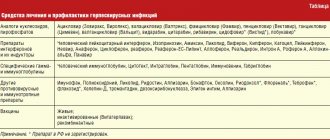
The main drugs for local antimicrobial therapy presented on the Russian market are listed in Table. 1. These drugs usually contain one or more antiseptics (chlorhexidine, hexetidine, benzydamine, ambazone, thymol and its derivatives, alcohols, iodine preparations, etc.), essential oils, local anesthetics (lidocaine, tetracaine, menthol), less often – antibiotics (fusafunzhin, framycetin) or sulfonamides, deodorizing agents. Preparations may also contain bacterial lysates (Imudon), natural antiseptics (plant extracts, bee products), synthesized factors of nonspecific protection of mucous membranes, which also have an antiviral effect (lysozyme, interferon), vitamins (ascorbic acid).
Antimicrobial drugs can be prescribed in the form of rinses, insufflations, inhalations, as well as tablets and lozenges. The main requirements for drugs applied to the mucous membrane are:
- a wide spectrum of antimicrobial action, preferably including antiviral and antimicrobial activity;
- lack of toxic effect and low rate of absorption from mucous membranes;
- low allergenicity;
- no irritating effect on the mucous membrane.
Most of those listed in table. 1 drugs (Hexalize, Drill, Septolete, Faringosept, Neo-angin, Strepsils, etc.) are available in the form of tablets, lozenges or lozenges. This form of drugs has relatively low activity, and their use is limited to mild forms of the disease. In addition, the doctor should remember the toxicity of chlorhexidine, which is part of many drugs (Antiangin, Drill, Sebidine, Eludril) and should not allow their unlimited, uncontrolled use by patients (especially children).
The prescription of a number of drugs is limited by their high allergenicity and irritating effect. This includes drugs containing iodine derivatives (iodinol, iox, vocadine, povidone-iodine), propolis (proposol), sulfonamides (bicarmint, ingalipt). Preparations containing herbal antiseptics and essential oils are effective and harmless, but their use is contraindicated in patients suffering from allergies to pollen, and the number of people with this disease in some geographic areas is up to 20% of the population.
Due to the fact that within the framework of this article it is impossible to give a detailed overview of all the drugs listed in Table 5, we will focus only on those drugs that are regularly used in our practice and the effectiveness of which has been confirmed by our own experience.
Inhalation antibiotic fusafyungin (Bioparox)
– a drug that combines antibacterial properties with anti-inflammatory properties and is produced in the form of a dosed aerosol, has been used in the treatment of respiratory tract infections for more than 20 years. Due to the very small size of aerosol particles, fusafunzhin is able to penetrate into the most inaccessible parts of the respiratory tract and exert its therapeutic effect there. The high antimicrobial effectiveness of fusafyungin in acute pharyngitis, laryngitis and tracheobronchitis has been confirmed by a large number of observations. The spectrum of antimicrobial activity of fusafyungin is adapted to microorganisms that are most often the causative agents of upper respiratory tract infections; it is also active against mycoplasma infections. The unique quality of this drug is the stability of its spectrum of action: during its use, no new strains of bacteria resistant to it have emerged. In addition to antibacterial properties, fusafungin has its own anti-inflammatory effect, which has been demonstrated in experimental studies [8]. It enhances phagocytosis of macrophages and inhibits the formation of inflammatory mediators. This explains the effectiveness of the drug for viral pharyngitis, although the drug does not have a direct inhibitory effect on viruses. When prescribing fusafunzhin, a smoother course after tonsillectomy was noted [1].
Imudon
fundamentally different from all drugs used for local treatment of pharyngitis.
It is a multivalent antigenic complex, which includes lysates of 10 bacteria, as well as two causative agents of fungal infections (Candida albicans and Fusiformis fusiformis),
most often causing inflammatory processes in the oral cavity and pharynx. Imudon activates phagocytosis, helps increase the number of immunocompetent cells, increases the content of lysozyme and secretory IgA in saliva. Data have been obtained indicating that the administration of imudon for acute, as well as catarrhal, hypertrophic and subatrophic forms of chronic pharyngitis is more effective than traditional methods of treatment, such as inhalation of alkaline and antibacterial drugs, cauterization of granules with a solution of silver nitrate and the use of other anti-inflammatory and analgesic drugs [2]. If necessary, imudon combines well with local or systemic antibiotics, helping to reduce recovery time and maintain local immune defense, which is especially important during antibiotic therapy. Imudon is available in the form of lozenges.
Hexetidine
(Hexoral) is available both as a rinse solution and an aerosol. Unlike chlorhexidine, the drug is low-toxic. It is active against most bacteria - the causative agents of pharyngitis and tonsillitis, as well as fungi. In addition to being antimicrobial, hexetidine has a hemostatic and analgesic effect, which justifies its use not only after tonsillectomy and opening of a peritonsillar abscess, but also after extensive operations in the pharynx (for example, operations for obstructive sleep apnea syndrome, etc.). The combination of the above-mentioned effects with the deodorizing effect of the drug is beneficial in patients with tumors of the upper respiratory tract, in particular, those receiving radiation therapy.
Antiseptic for mucous membranes octenisept
has, perhaps, the widest spectrum of antimicrobial action, covering gram-positive and gram-negative bacteria, chlamydia, mycoplasma, fungi, protozoa, as well as herpes simplex viruses, hepatitis B and HIV. The effect of the drug begins within a minute and lasts for an hour. Octenisept has no toxic effect and is not absorbed through intact mucous membranes. We use a solution of octenisept, spraying this solution onto the mucous membranes using an insufflator [9]. Of course, the main disadvantage of this drug is that it is not available in forms convenient for independent use, and its use is mainly limited to the practice of specialized departments.
Local antibacterial agents can be widely used in the treatment of pharyngitis.
The choice of the optimal drug is determined by the spectrum of its antimicrobial activity, the absence of allergenicity and toxic effect. Of course, the most effective local drugs will not completely replace the need for systemic administration of antibiotics for sore throat and pharyngitis caused by beta-hemolytic streptococcus. On the other hand, due to the nonbacterial etiology of many forms of pharyngitis, the emergence of an increasing number of resistant strains of bacteria, as well as the undesirable effects of general antibiotic therapy, local administration of drugs with a broad spectrum of antimicrobial activity is in many cases the method of choice. Literature:
1. Luchikhin L.A., Buyanovskaya O.A., Derevyanko S.N., Paukova M.V. The effectiveness of Bioparox treatment of acute inflammatory diseases of the upper respiratory tract. Vestn. otorhinol., 1996; 2: 38–42.
2. Luchikhin L.A., Malchenko O.V. The effectiveness of the drug Imudon in the treatment of patients with acute and chronic inflammatory diseases of the pharynx // Vestn. otorhinol., 2001; 3:62–4.
3. Dagnelie CF Sore Throat in General Practice. A Diagnostic and Therapeutic Study. Thesis. Rotterdam, 1994.
4. Hansaker DH, Boone JL Etiology of Infectious Diseases of the Upper Respiratory Tract. In: Ballenger JJ, Snow JB, editors, Otorhinolaryngology: Head and Neck Surgery. 15th edition. Baltimore: Williams & Wilkins, 1996, 69–83.
5. Gwaltney JM The common cold. In: Mandell GL, Bennet JE, Dolin R, editors, Principles and Practice of Infectious Diseases. 4th Edition. NY: Churchill Livingstone - 1996, 561–6.
6. Gwaltney JM Pharyngitis. Ibid., 566–9.
7. de Melker R. Prescribing patterns for respiratory tract infections: Dutch data from international perspective. In: Program and abstracts of the 3rd International Meeting on Upper Respiratory Tract Infections. Crete, 1997, S1.
8. Otori N., Paydas G., Stierna P., Westrin KM The anti-inflammatory effect of fusafungine during experimentally induced rhinosinusitis in rabbit. Eur Arch Otorhinolaryngol 1998; 255:195–201.
9. Piskunov GZ, Piskunov SZ, Lopatin AS Substantiation of the use of Octenisept in acute and chronic inflammation of nasal mucosa. In: Liber Amicorum. Prof. Dr. EHHuizing 1976–1997. Utrecht, 1997; 181–5.
10. Rice DH Microbiology. In: Donald PJ, Gluckman JL, Rice DH, Editors, The Sinuses. New York: Raven Press, 1995, 57–64.
Combined drug -
Imudon (trade name)
(Solvay Pharma)
Combined drug -
Strepsils (trade name)
(Boots Healthcare International)
Symptoms and first signs
The incubation period is quite short, amounting to 16 hours after infection enters the body.
Initial symptoms are mild fatigue, a feeling of cold, sneezing and a slight headache, they soon develop into nasopharyngitis with a stuffy nose, nasal discharge, sore throat and low-grade fever, peaking at 2-4 days.
During the incubation period, the first symptoms of nasopharyngitis appear, namely:
- unusual and unexplained fatigue occurs;
- fever appears, rarely exceeding 38.5 degrees;
- runny nose, first clear, then thick (yellowish to greenish);
- nasal congestion, which may be accompanied by shortness of breath;
- mild sore throat and redness;
- fairly dry cough;
- sneezing;
- ear pain;
- tearfulness;
- the body “aches”;
- headache and/or abdominal pain;
- loss of appetite.
Fever lasts two or three days in the case of nasopharyngitis. To reduce your fever, you can take paracetamol at recommended doses at least 6 hours apart.
Diagnostics
When exactly should you go to the doctor?
- if the child is less than three months old;
- if the fever lasts more than 72 hours and does not decrease;
- if there is pain in the ear;
- if there are spots on the skin;
- if there is bleeding from the nose or urine with blood elements;
- if the child has breathing problems.
The diagnosis of nasopharyngitis is clinical, that is, it is established by examination and observation of symptoms. Does not require additional examination. A thorough clinical examination will eliminate the complication or associated pathology, such as otitis media, and evaluate possible risk factors.
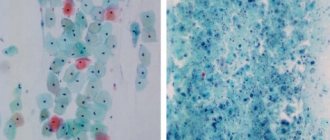
If you see an otolaryngologist (ENT), he or she may perform a rhinoscopy to examine the inside of the nose using a rhinoscope, a rigid or flexible optical device. In the case of nasopharyngitis, rhinoscopy shows a very red and congested mucous membrane of the nose and throat.
Causes of inflammation of the nasopharynx
The genetic markers for vitamin E absorption are ApoA5. The zinc finger protein regulates the transcription of genes whose products regulate triglyceride levels and SCARB1. Scavenger receptor B1 is involved in the metabolism of lipids and vitamin E.
Rhinopharyngitis or nosopharyngitis
- an inflammatory disease that affects the mucous membrane of the pharynx and nose.
The causes of inflammation can be:
- viruses (most often rhinovirus, but also adenoviruses, ECHO viruses, influenza, parainfluenza, coronaviruses);
- bacteria (streptococci, staphylococci, mycoplasmas, chlamydia, meningococci);
- irritating substances, allergens (household, fungal, plant, food allergens, house dust, waste products of animals, birds, insects, components of household chemicals, tobacco smoke).
We have prepared for you a list of studies that will help you deal with this problem:
30 working days
Gut microbiome
12000 ₽
More details
How to treat nasopharyngitis
Rhinopharyngitis usually goes away on its own. Treatment is aimed at limiting cold symptoms while keeping the patient comfortable and avoiding overexertion if necessary.
The following measures are prescribed:
- regular rinsing of the nasal sinuses (with saline, nasal spray, thermal or sea water);
- taking painkillers for pain and antipyretics for fever.
In the first days, a cough due to nasopharyngitis is often dry and painful, then people often wonder how to treat it. In this case, you can, on the doctor's recommendation, buy cough syrup. But be careful: as soon as the cough becomes wet and accompanied by mucus, syrups should be avoided. Because a wet cough helps evacuate germs. Cough is an excellent natural treatment for nasopharyngitis.
Also, keep in mind that a fever is just an expression of the body fighting an infection. In fact, viral infections of this type are often “self-limiting,” meaning that they will heal on their own. However, it is important to monitor your temperature and make sure it is not too high to prevent febrile seizures.
Contrary to what many parents believe, antibiotics do not help fight viral infections. Thus, treatment of nasopharyngitis consists of controlling symptoms. In some cases, antihistamines may be used to relieve allergies, antitussives to relieve coughing, or expectorants to help clear secretions. Antipyretics also help control fever.
Rhinopharyngitis usually lasts about 7-10 days. During this period, it is important to give the body sufficient rest. The healing process can be supported by keeping the mucous membrane moist, drinking enough fluids, or using inhalations and decongestants.
Diagnosis of tracheitis
In addition to the standard history taking, external examination, assessment of respiratory function, initial examination of the throat and auscultation using a phonendoscope, there are laboratory and instrumental diagnostic methods, as well as additional studies that can lead the doctor to tracheitis4. It is on the basis of diagnosis that the causes of tracheitis and methods of its treatment are determined.
- General and biochemical blood test. The simplest test to distinguish between viral and bacterial infections (based on C-reactive protein and other indicators)
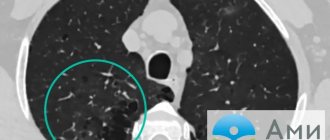
- X-ray or radiography. The most common and familiar way to check the chest. The picture can be taken in front or side projections. The image clearly shows the lungs and trachea. Thanks to x-rays, it becomes much easier to identify signs of tracheitis and distinguish it from bronchitis or pneumonia.
- Taking and examining smears. A standard procedure in which the doctor uses a sterile cotton swab to take a swab from the mouth. Next, the material is sent to the laboratory, where all the necessary studies are carried out, identifying the pathogen and its sensitivity to antibiotics.
- Laryngotracheoscopy. The endoscope comes into play. This study is the most informative. A special tube with a camera is inserted into the larynx and trachea, thereby the doctor can visually identify characteristic features, swelling, redness, etc. and possible causes of the disease (with a viral infection there are specific changes in the organ). If the study involves the bronchi, the procedure is called tracheobronchoscopy.
- Taking sputum for analysis. In this case, the sputum of a sick person is collected and sent for bacteriological examination (microbiological examination). This procedure is used for a more comprehensive diagnosis of chronic cough to exclude other bacterial diseases (tuberculosis).
- Pharyngoscopy. The standard method is for the doctor to examine the throat using a spatula. First of all, pharyngitis is diagnosed, which makes it clear about the possible development of tracheitis.
- Rhinoscopy. The procedure is an examination of the nasal cavity. For this, an optical device is used - a rhinoscope. Rhinitis is detected as a consequence of a respiratory infection, which means progression of tracheitis is possible.
- X-ray of the sinuses. X-ray, images of which will determine the presence of sinusitis or sinusitis if they are suspected. The progression of the disease may also affect the development of inflammation in the trachea.
- Allergy tests. In rare cases, tracheitis occurs due to an allergic reaction. Allergy tests allow you to determine which allergens your body responds to. Various substances are applied to the skin; if a reaction occurs in the form of redness, itching or swelling, then the allergen has been identified.
In addition to the help of a therapist and otolaryngologist (ENT), to determine the causes and make a diagnosis, consultations with doctors such as an allergist, pulmonologist and even a phthisiatrician may be required.
Complications of nasopharyngitis
The risk of complications increases without treatment or when the body cannot heal itself. On the one hand, viruses in the respiratory tract will multiply, infecting areas that are still healthy, and on the other hand, nasopharyngitis can pave the way for bacterial superinfections. Superinfection is when a viral infection sets the stage for a subsequent bacterial infection due to a weakened immune system. If your general health does not improve or your symptoms worsen, you should see your doctor as soon as possible.
Rhinopharyngitis rarely causes complications, but some people with weakened immune systems may experience a secondary bacterial infection in the form of:
- tonsillitis (inflammation of the tonsils of viral or bacterial origin);
- laryngopharyngitis;
- tracheitis (inflammation of the trachea, causing an irritating cough);
- bronchitis (inflammation of the bronchi, which usually manifests itself in the form of cough and difficulty breathing);
- sinusitis (inflammation of the sinuses associated with an infection of viral or bacterial origin);
- otitis (inflammation or infection of the ear);
In this case, consultation is necessary, as well as treatment with antibiotics if a bacterial infection is proven.
In children under 3 months of age, complications occur more often due to insufficient maturation of the immune system. Therefore, in this case, as in pregnant women, with constant fever, careful monitoring of the condition is necessary.
Chronic tracheitis
The symptoms of chronic and acute tracheitis and the process of the disease itself are almost identical. The main difference between chronic tracheitis and acute is the long course of the disease. Symptoms of tracheitis either subside or flare up again during the next onslaught of ARVI. With an exacerbation of the chronic form of the disease, the cough is more severe, and pain in the chest area causes more discomfort.
As a rule, the chronic form develops against the background of untreated acute tracheitis as a result of problems with the immune system or exposure to adverse factors. But in rare cases, chronic tracheitis occurs locally, developing simultaneously with bronchitis in people exposed to smoking, alcohol, and liver, kidney and heart diseases.
The causative agent is still a viral, bacterial, fungal infection or, in rare cases, an allergic reaction.
In certain groups of people, the chronic form of tracheitis is more likely to develop. This is facilitated by 2:
- Smoking and drinking alcohol, especially during infectious tracheitis
- Reduced immunity or immunodeficiency, hereditary and acquired
- Ecology and hazardous place of work (constant inhalation of gases, dust, etc.)
- Liver, heart and kidney diseases
- Other chronic diseases of the respiratory system - sinusitis, sinusitis, rhinitis or laryngitis
Traditional treatment
Treatment with folk remedies will help improve your condition and maintain your health.
- Using a humidifier. To thin out secretions, it is recommended to humidify the surrounding air and maintain the room temperature to 19 degrees.
- Inhalation of eucalyptus essential oils.
It is necessary to do inhalations so that it has a decongestant effect, helping to clear a stuffy nose. Essential oils can also be used in chest massage. But remember that treating colds with essential oils is contraindicated for children, pregnant or lactating women, patients with asthma or epilepsy. Consult your doctor before use. - Elder. Has antipyretic and anti-edematous effects. This plant can be used as an herbal tea (let steep for at least 10 minutes) or as a gargle (with cooled herbal tea) several times a day.
- Chamomile. For children, a runny nose can be very uncomfortable because it prevents them from breathing, causing them to be irritable and may lose their appetite. In these cases, it is best to resort to homemade solutions prepared with the addition of salt or chamomile.
Rhinopharyngitis can be treated well with folk remedies if you follow the above steps and know how to treat it.
Prevention
There are several rules to strengthen your immune system and prevent disease.
- Wash your hands often and teach your children to do it correctly, especially after blowing their nose.
- Do not share personal items such as glasses, dishes, or a sick person's towel.
- Protect your mouth when you cough or sneeze with a disposable tissue. If you don’t have a disposable tissue, cough into the crease of your elbow rather than into your palm.
- Don't overheat the house, keep the room temperature between 18 C and 20 C to keep the air humid. Too dry air makes symptoms worse.
- Ventilate the room regularly, even when it’s cold.
- Get enough sleep and avoid stressful situations.
- Consume vitamin C and honey daily in preventative doses.
Good to know! Rhinopharyngitis remains contagious for a long time, in some cases up to 21 days.
Possible causes of sinusitis
- Untreated colds: 5 to 10% of neglected colds turn into sinusitis.
- Dental procedures and untreated oral infections because the maxillary molars and premolars are located close to the maxillary sinuses.
- Congenital or traumatic anatomical anomalies: deviated septum, too narrow nasal passage, nasal polyps (often of allergic origin).
Therefore, specialists who can help with rhinosinusitis include: ENT doctors, therapists, dentists and plastic surgeons.
It should be noted that during treatment for acute or chronic sinusitis, you may begin to feel better after taking antibiotics, but sometimes symptoms worsen and additional treatment and even hospitalization may be required. In order to effectively combat sinusitis, it is necessary to first eliminate the underlying disease - a cold, dental caries, or, if necessary, perform rhinoplasty, surgical correction of the nasal septum (septoplasty), polypectomy, etc.
In the case of acute sinusitis, the disease usually lasts up to 4 weeks. Two-thirds of people with acute sinus inflammation improve without any treatment. If your doctor has reason to believe that the sinus infection is caused by bacteria rather than viral agents, you will be prescribed antibiotic therapy. The number of days you take an antibiotic depends on the type of antibiotic and the severity of the infection. When you take an antibiotic, you should take it until the end of the prescribed treatment period, even if you feel better, otherwise the infection may not be completely cured and the microbes will have the opportunity to develop resistance to the medicine.
With chronic sinusitis , the illness usually lasts 12 weeks or longer. Chronic sinusitis is more difficult to treat and responds more slowly to antibiotics than acute sinusitis. Treatment of chronic sinusitis will require a long course of antibiotic therapy. You may be prescribed more than one antibiotic. In complex treatment, it may be necessary to prescribe a nasal spray with corticosteroids, which reduces inflammation and swelling of the mucous membrane of the nasal passages.
People with impaired immune system function and those taking immunosuppressive drugs (for example, long-term therapy with glucocorticosteroids) have an increased risk of chronic sinusitis caused by atypical and fungal pathogens. The peculiarity of fungal sinusitis is that it does not respond to treatment with antibiotics and may require the prescription of antifungal drugs, corticosteroids, or surgical treatment. Surgery may be indicated if you have been taking antibiotics for a long period of time but symptoms still persist or complications have developed (for example, a bone infection in the face).