Anatomy and physiology
The large intestine is separated from the overlying small intestine by a muscular valve, the so-called. ileocecal sphincter or bauhinian valve. The large intestine is located in the lower part or floor of the abdominal cavity and includes the following sections:
- Caecum (lat. – caecum). It is 3-8 cm long and 4-7 cm wide. This section of the large intestine is equipped with a vermiform appendix, the appendix. The cecum with the appendix is projected onto the right middle and lower part of the anterior abdominal wall.
- Colon (lat. – colon). The longest section of the small intestine. The colon, about 4 cm in diameter, borders the entire lower floor of the abdominal cavity with loops of the small intestine and other organs. Hence the name. In the colon, its initial ascending part is distinguished. 12-20 cm long from the cecum to the right bend, the so-called. hepatic angle. The transverse colon is its middle part, 50 cm long, from the hepatic angle to the splenic angle, the left bend. The descending part, 22-23 cm long, runs from the splenic angle to the sigmoid colon. Due to the fact that the transverse part sags slightly, the configuration of the colon resembles the letter M.
- Sigmoid colon (lat. - colon sigmoideum). The same applies to the colon, and in the form of two loops 54-55 cm long and 4 cm in diameter is located between the descending part and the rectum. It is projected onto the anterior abdominal wall in its lower left part.
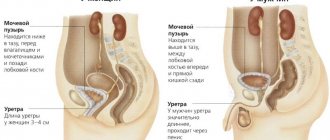
- Rectum (lat. - rectum). Located in the pelvic cavity. The length of the rectum is 14 cm. The width in the initial sections is 4 cm, then it expands into the ampulla of the rectum 7.5 cm, and ends with a narrow opening of the anus.
Compared to other parts of the gastrointestinal tract , the large intestine has its own characteristics. Unlike the pink small intestine, the large intestine has a grayish color. On the outside it is covered with a serous connective tissue membrane. Parts of the colon, and in some cases the cecum, are fixed to the walls of the abdominal cavity by the mesentery. This mobile anatomical formation is formed by two layers of peritoneum. Vessels and nerves pass through the mesentery to the intestines.
The middle muscular layer is represented by an inner circular or circular layer and an outer longitudinal layer. Peristaltic (wave-like) contractions of these muscles ensure the movement of the food bolus through the intestinal tube.
But, unlike other parts of the gastrointestinal tract, the outer muscle layer here is continuous only at the junction of the cecum with the appendix , and in the rectum. And for the most part it is represented by three ribbons. These tapes seem to tighten the intestinal tube. As a result, protrusions and haustra are formed on its surface. The haustrae are separated from each other by transverse grooves. These grooves correspond to the semilunar folds of the mucous membrane.
There are no villi on the mucous membrane, like in the small intestine. It contains secretory glands that secrete digestive juice. Colonic juice is secreted at rest, but its amount is small.
Food contents enter the large intestine from the small intestine in small portions at the moment the ileocecal sphincter opens. In response to mechanical irritation, juice secretion increases many times over. It contains: amylase, lipase, and a number of other digestive enzymes. But in general, the content of enzymes in the juice of the large intestine is low, 20 times less than in the juice of the large intestine.
The amount of absorbed food components is also small. Here, those food components that are not absorbed in the small intestine are absorbed in small quantities. The main function of the large intestine is to absorb water from the bolus of food and form feces in a daily amount of 150 g or more.
When eating plant foods, more feces are formed than when eating foods of animal origin. Plant foods contain a large amount of indigestible fibers that absorb intestinal toxins. The final section of the gastrointestinal tract, the rectum, serves as a reservoir for feces. The act of defecation is controlled by muscle valves - the internal and external sphincter.
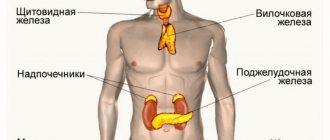
The functioning of the large intestine is largely influenced by the microflora it contains, represented by bifidobacteria, lactobacilli, and bacteroides.
The main functions of physiological intestinal microflora:
- The final breakdown of undigested food components.
- Inactivation of bile components and digestive juices that enter the large intestine from the overlying sections of the gastrointestinal tract.
- Neutralization of toxic products formed during the digestion of food.
- Synthesis of vitamin K and some B
- Destruction of pathogenic intestinal microflora.
- Participation in other nonspecific immune reactions.
Along with microflora, immune protection is provided by accumulations of lymphoid tissue located in the mucous membrane, lymphatic follicles.
The role of the intestines in the functioning of the human body
Many people are interested in where the human intestines are located.
?
With the help of this organ, the body gets rid of toxins and waste. All antibodies secreted by organs and organ systems are eliminated through the gastrointestinal tract during life. All digested unnecessary substances are excreted from the body along with feces. Here are the main functions of the human intestine
.
Small intestine
Anatomy of the human intestine
- read on. The section of the gastrointestinal tract that goes immediately after the stomach and is the longest section of the intestine. Due to the presence of a large number of villi, it is in the small intestine that further digestion and absorption of all useful substances that are needed to build the cells of the body take place. It also synthesizes a large number of hormones and vitamins. One of them is cholecystokinin. It is the most important hormone necessary for controlling appetite, giving a feeling of fullness and a good mood.
Colon
An important section of the gastrointestinal tract, it does not have loops, but it goes around the small intestine. It is important that there is a valve between the sections of the intestine. It is he who prevents the food bolus from returning from the large intestine back to the small intestine. The large intestine does not absorb useful nutrients; it absorbs water, electrolytes and vitamins. The main function of this section of the intestine is the formation and removal of undigested substances.
Diseases and symptoms
Diseases of the large intestine:
- Chronic non-infectious inflammatory processes of the cecum, colon and sigmoid colon - typhlitis, colitis, sigmoiditis.
- nonspecific ulcerative colitis;
- appendicitis;
- acute intestinal infections;
- helminthiases;
- diseases of the rectum - proctitis, paraproctitis, hemorrhoids, anal fissures;
- cancer of various parts of the large intestine;
- colonic benign tumors, polyps;
- colonic obstruction caused by paralysis of smooth muscles, blockage of the intestinal lumen by a tumor, and other reasons.
Typical symptoms of chronic diseases:
- widespread aching abdominal pain;
- bloating, flatulence ;
- diarrhea, constipation , their alternation;
- pain, feeling of incomplete bowel movement after bowel movement;
- admixture of mucus, blood in the stool;
- dark “cherry” or tarry stools are a sign of intestinal bleeding.
Intestinal obstruction and other acute diseases are characterized by the patient’s severe general condition. Peritonitis (inflammation of the peritoneum) with sharp pain and tension in the muscles of the abdominal wall is possible. Intoxication is accompanied by nausea and vomiting. With intestinal obstruction, vomiting may take on a fecal character.
Chronic diseases of the large intestine, as a rule, occur against the background of dysbiosis with emaciation, anemia, vitamin deficiencies, and decreased immunity.
Possible complications during treatment
The side effects that may occur depend mainly on the type of bowel resection and your overall health. They include:
- obstruction (obstruction) of the intestine,
- paralyzed or inactive bowel
- damage to nearby organs such as the bladder, ureter or spleen, anastomotic leak associated with infectious problems,
- excessive bleeding wound infection,
- hernia,
- thrombophlebitis,
- inability to control urination.
The attending physician should be informed of any of the following problems after surgery: severe pain, swelling, redness, drainage or bleeding in the incision area, muscle pain, dizziness or fever, constipation, nausea or vomiting, rectal bleeding or black, tarry stools.
Diagnostics
Diagnosis of the large intestine begins with a digital examination of the anus. Next, laboratory and instrumental studies begin. , endoscopy of the large intestine is diagnostically valuable - sigmoidoscopy and colonoscopy . During sigmoidoscopy, the doctor examines the rectum and sigmoid colon, and during colonoscopy, the entire large intestine.
Irrigoscopy is an X-ray diagnosis of the large intestine after filling through the anus with a contrasting barium suspension. Plain radiography of the abdominal organs without the use of contrast is informative in case of intestinal obstruction. The so-called Kloiber cups, horizontal fluid levels in the intestinal lumen. This is a symptom specific to intestinal obstruction.
Of the laboratory tests, the main place is occupied by the diagnosis of stool. Depending on the tasks assigned, feces are taken for:
- general analysis (coprogram);
- occult blood;
- worm eggs;
- bacterial culture on nutrient media.
A supporting role is played by a general and biochemical blood test, immunodiagnostics and blood culture on nutrient media.
Differences
The main difference between the two sections of the intestine is the functions they perform. After all, the main function of the small intestine is the absorption of nutrients, and the large intestine is fecal formation. They also have different diameters, in thick ones it ranges from 4 to 9 cm, in thin ones - from 2 to 4 cm.
The color of the large intestine should be grayish, and the small intestine should be pink. The large intestine has outgrowths and protrusions. The large intestine is approximately 5.5 mm thick, and the small intestine is almost 2 times thinner. Based on all of the above, you can understand the principles by which the digestive system works. Now you know where the intestines are in women
, and what functions it performs.
Observation program after treatment method
After your bowel resection you will need to stay in the hospital for several days. The patient should be given warm, liquid food for 1-2 days after surgery. Solid foods and meals will be introduced gradually. If a colostomy or ileostomy has been performed, a specially trained health care professional will teach the patient how to care for themselves. Temporary ostomies usually remain in place for several months. After the rest of the colon has healed, another operation, an anastomosis, will be performed. The hole in the stomach will be closed. A nasogastric tube is inserted through the nose into the stomach during surgery and may be left in place for 24 to 48 hours after surgery. This eliminates stomach secretions and prevents nausea and vomiting. It will remain until bowel activity resumes. Postoperative patient care also includes monitoring of blood pressure, pulse, respiration and temperature. Fluid intake and output are measured, and the color and amount of drainage from the wound is observed at the incision site. The patient can get out of bed approximately 8-24 hours after surgery. Most patients will stay in the hospital for 5-7 days, although laparoscopic surgery can reduce this stay to 2-3 days. Postoperative weight loss accompanies almost all bowel resections. Weight and strength are slowly restored over several months. You will need to follow a diet prescribed by your doctor. Full recovery from surgery may take two months. Laparoscopic surgery can reduce this time to one to two weeks.
Pain syndrome with damage to the large intestine
Many different diseases can cause pain in the large intestine. A number of factors lead to the development of such violations:
- sedentary lifestyle;
- eating disorders, including frequent overeating or following a strict diet;
- abuse of spicy, fatty, smoked foods;
- disruption of the digestive system in patients due to advanced age;
- chronic constipation;
- hypotension accompanied by impaired peristalsis;
- constant use of pharmacological drugs.
These factors can cause disturbances in the functioning of both the entire digestive tract and the large intestine separately. At the same time, it is usually quite difficult to establish the cause of the pain syndrome, and almost impossible on your own. In general, dysfunctions of the digestive system can be divided into two main groups:
- inflammatory in nature: colitis, diverticulitis, Crohn's disease, etc.;
- non-inflammatory disorders: atonic constipation, tumor processes, endometriosis, etc.
Diseases of the large intestine can significantly impair the patient's quality of life. To prevent the development of complications, it is necessary to promptly pay attention to the appearance of alarming signs of pathology.
Ulcerative colitis
Ulcerative colitis is an inflammatory lesion of the tissues of the large intestine. The disease has a chronic course and is characterized by fairly frequent relapses. To date, it has not been possible to accurately determine the cause of the development of the pathology, but it is classified as a disorder of autoimmune origin.
Colitis is most often detected in people of two age groups: patients 25-45 years old and patients over 55-60 years old.
There are three categories of disease progression:
- acute colitis;
- chronic with periodic exacerbations;
- chronic continuous, in which remission is not observed for 6 months or more.
The clinical picture of ulcerative colitis is generally synonymous with other diseases of the large intestine and is manifested by the following symptoms:
- Intense, long-lasting abdominal pain. Their localization largely depends on which part of the colon was affected by the pathological process.
- Diarrhea or constipation. In this case, bloody inclusions may be observed in the feces.
- Signs of intoxication of the body: nausea, cephalalgia, dizziness, drowsiness and lethargy.
Lack of therapy for colitis can lead to perforation of the intestinal wall and, as a consequence, massive intestinal bleeding. This condition is life-threatening for the patient.
Colitis therapy should be carried out comprehensively, taking into account the severity and form of the disease. In case of radical damage to the intestine, the patient is indicated for hospitalization. Therapy for ulcerative colitis:
| Drug name | Image | pharmachologic effect |
| Mesalazine | Anti-inflammatory and antimicrobial agent | |
| 5-ASK | Anti-inflammatory and cytoprotective effects | |
| Prednisolone | Anti-inflammatory, immunosuppressive effect | |
| Cyclosporine | Immunosuppressant |
Crohn's disease
Crohn's disease is a chronic inflammatory bowel disease, which is characterized by the formation of ulcerations on the intestinal mucosa, in place of which granulomas subsequently grow, adhesions and strictures form, which narrows the intestinal lumen and impairs its patency.
Researchers have identified several factors that are important in the mechanism of chronic intestinal inflammation, but the trigger point in the pathological process is not known. Contributing factors include:
- Failure in the body's immune system. In the mechanism of maintaining inflammation, the autoimmune component plays an important role, that is, the pathological reaction of the immune system to the body’s own tissues, as well as to those intestinal microorganisms that are not pathogenic and are necessary for the absorption of food;
- Hereditary predisposition. It is known that people with Crohn's disease often have relatives suffering from chronic inflammatory bowel diseases, such as ulcerative colitis;
- The damaging effects of external factors: unhealthy diet, bad habits, unhealthy lifestyle, infection.
Drug treatment of Crohn's disease during an exacerbation consists of the use of antidiarrheals, anti-inflammatory drugs (hormonal therapy with corticosteroids), antibacterial drugs and drugs that suppress excessive activity of the immune system (immunosuppressants).
Therapy for Crohn's disease
| Drug name | Image | pharmachologic effect |
| Sulfasalazine | Anti-inflammatory, antibacterial effect | |
| Budenofalk | Decongestant, antihistamine effect – corticosteroid | |
| Azathioprine | Immunosuppressive drug | |
| Imodium | Antidiarrheal agent | |
| Acetaminophen | Analgesic effect |
Diverticular disease
Diverticular disease of the colon, a disease characterized by the formation of multiple thinned protrusions of the mucous membrane on the intestinal walls beyond the intestinal wall, most often affects patients in older age groups. According to statistics, the occurrence of colon diverticulosis in the age group under 40 years old occurs in less than 5%. At older ages, the disease occurs more often, and in patients over 85 years of age, this disease is registered in 65% of cases.
Factors that, according to experts, influence the development of diverticular disease include:
- genetic predisposition
- lack of physical activity
- obesity
- smoking
- decrease in beneficial gut bacteria
- increase in pathogenic bacteria in the intestines
- taking certain medications, including steroidal and nonsteroidal anti-inflammatory drugs such as ibuprofen
The older a person is, the higher the risk of developing diverticular disease. The 40-year mark is considered a milestone. In general, by the time they reach their 80th birthday, most people have this disease.
Therapy for diverticular disease
| Drug name | Image | pharmachologic effect |
| Cefoxitin | Antibacterial action | |
| Portalac syrup | Prebiotic with laxative effect | |
| Domperidone | Stimulation of gastrointestinal motility | |
| No-shpa | Antispasmodic effect | |
| Tylenol | Analgesic effect |
If there is no effect from conservative therapy, the patient needs surgical intervention.
Malignant neoplasms
Neoplasms of the large intestine can be both malignant and benign. At the same time, the first group of tumors is characterized by slow growth and does not cause a significant deterioration in the patient’s quality of life.
Carcinomas develop more aggressively, which leads to the appearance of a characteristic clinical picture of cancer:
- attacks of vomiting, admixture of feces in the vomit;
- loss of appetite leading to cachexia;
- lethargy, drowsiness, weakness;
- low-grade fever;
- stool disorders;
- melena - black stool mixed with blood;
- cutting and tearing pain in the area of tumor formation.
The thick gastrointestinal tract is an important part of the digestive system. Pain in this part of the gastrointestinal tract may indicate the development of serious pathologies and require urgent consultation with a specialist.