Features of the anatomy of the genital organs in women
The female reproductive system performs several functions, one way or another related to procreation. The anatomy of this system includes the internal and external genitalia. The internal genital organs are located in the pelvic cavity. These include:
- The vagina is an elastic tube 10–12 cm long with walls 3–4 mm thick. This is the channel for the exit of the fetus during childbirth and the receiver of male seed during sexual intercourse.
- The uterus is the reproductive organ where the embryo is born. Located behind the bladder. It is distinguished by powerful muscle tissues that can expand during pregnancy.
- Fallopian tubes located on both sides of the uterus. Their function is to move the fertilized egg into the uterus.
- The ovaries are paired glands located in the abdominal cavity below the level of the navel. Responsible for the maturation of eggs.
External organs of the female reproductive system:
- The pubis is a soft tissue formation above the labia.
- Labia. They are divided into large and small. Protect the vagina and maintain thermal conditions.
- The clitoris is an erogenous zone with high sensitivity. Responsible for sexual arousal.
The pelvic muscles in women are conventionally divided into three layers, differing in location. The deepest is divided into the pubic, ischial and iliac parts. All parts are attached to the pubic symphysis and pubic bone.
Inguinal region anatomy. MCPC Rusakov V.I. 1997
The groin area has the shape of a right triangle. Its boundaries are: below - the Poupart ligament, above - the line connecting the right and left anterior superior iliac spines, and on the inside - the outer edge of the rectus abdominis muscle (Fig. 39).
Inguinal region anatomy. MCPC Rusakov V.I. 1997
The groin region contains the following layers: skin, subcutaneous tissue, superficial fascia, deep fascia, aponeurosis of the external oblique muscle, internal oblique muscle, transversus abdominis muscle, transversalis fascia, preperitoneal fatty tissue and peritoneum.
The fibers of the aponeurosis of the external oblique muscle of the abdomen go from top to bottom and inside. The lower thickened edge of the aponeurosis seems to stretch between the anterior superior axis of the ilium and the pubic bone. It turns downwards and backwards and forms a groove, which is an independent anatomical formation called the inguinal (pupart) ligament. The aponeurosis of the external oblique abdominal muscle and the Poupartian ligament are dense and strong. But they can be underdeveloped and disintegrating.
A denser aponeurosis is found in women. The outer edge of the inguinal ligament is attached to the upper anterior iliac spine, and the inner one splits and forms two legs: the inner (superior) and the outer (id). The inner leg is attached to the pubic symphysis, and the outer leg is attached to the pubic tubercle of the pubic bone.
A triangular space is formed between the legs, the outer edge of which is limited by arched bundles of the aponeurosis, which are called interpeduncular bundles (Fig. 40). This triangular space is called the superficial ring of the inguinal canal. Through it, the spermatic cord emerges from the inguinal canal in men, and the round ligament of the uterus in women. The dimensions of the superficial inguinal ring range from 2-3X1-2 cm. It is generally accepted that a normal inguinal ring allows only the tip of the index finger to pass through.
Inguinal region anatomy. MCPC Rusakov V.I. 1997 2
The lower edges of the internal oblique and transverse abdominal muscles are adjacent to the inguinal ligament, leaving only space for the spermatic cord in men or the round ligament of the uterus in women. This space in which the spermatic cord or round ligament of the uterus passes is called the inguinal space or (which is not entirely correct) the inguinal canal. The canal appears only when a hernia forms.
The inguinal space runs in the direction of the pupart ligament from the internal (deep) inguinal ring to the superficial one. The walls of the inguinal space are: anterior—aponeurosis of the external oblique muscle, posterior—transverse fascia, upper—edges of the internal oblique and transverse muscles, lower—pupart ligament (Fig. 41). In men, the inguinal space is shorter and wider, in women it is longer and narrower.
Inguinal region anatomy. MCPC Rusakov V.I. 1997 3
The given anatomical features of the structure of the groin region in men and women decipher the more frequent formation of inguinal hernias in men, who have a weaker aponeurosis of the external oblique abdominal muscle than women, less perfect internal oblique and transverse muscles and a wider inguinal space (canal), containing more massive formation (spermatic cord).
The interpretation of the more frequent formation of inguinal hernias in men is complemented by two more circumstances: men more often perform heavy physical work and may have some diseases (contributing to the appearance of hernias), which women do not suffer from at all (prostate adenoma, phimosis) or suffer from extremely rarely (urethral strictures) .
For a complete understanding of inguinal hernias, their appearance and development, it is necessary to know the anatomy of the anterior abdominal wall from the abdominal cavity. In the lower part of the inner surface of the anterior abdominal wall, from the navel downwards there are five folds of the peritoneum (Fig. 42), between which there are six fossae - three fossae on each side.
Inguinal region anatomy. MCPC Rusakov V.I. 1997 4
Along the midline from the bladder to the navel is the median umbilical fold (plica urabilicalis mediana), in which the obliterated urinary duct is located. More lateral is a paired fold (medial umbilical fold—plica umbilicalis media), formed along the obliterated umbilical arteries; even more lateral there is a second paired fold covering the lower epigastric vessels, the lateral umbilical fold (plica umbilitcalis lateralis).
Below, between the median and medial umbilical folds, a supravesical fossa (fossa supravesicalis) is formed. Very rare so-called supravesical hernias can originate here. Between the medial and lateral folds there is the middle inguinal fossa (fossa inguinalis medialis), which, in the sagittal plane, corresponds to the position of the superficial inguinal ring. In the area of the middle inguinal fossa, direct inguinal hernias originate, going directly into the superficial ring of the inguinal canal (Fig. 43).
Inguinal region anatomy. MCPC Rusakov V.I. 1997 5
Outside the lateral umbilical fold is the lateral fossa of the peritoneum (fossa inguinalis lateralis), corresponding to the internal ring of the inguinal canal. Here, the spermatic cord or round ligament of the uterus passes into the thickness of the abdominal wall, and then into the inguinal canal. In the area of the lateral fossa (internal inguinal ring), an oblique inguinal hernia begins to form. During the development of a hernia, the hernial sac passes through the inguinal gap, turning it into a canal, exits through the superficial inguinal ring under the skin, and then descends into the scrotum.
Embryological and anatomical data show that inguinal hernias are direct and oblique, and oblique inguinal hernias are congenital (with non-fusion of the peritoneal inguinal process) and acquired (Fig. 44).
With oblique inguinal hernias, the hernial sac travels from the deep inguinal ring, through the inguinal canal under the skin at the root of the scrotum and can, under conditions favorable for the development of a hernia, descend into the scrotum, forming an inguinal-scrotal hernia.
Congenital hernias are detected immediately after birth or in the first years of life; acquired hernias develop most often in adults. It is clear that in patients with congenital hernias, from the moment of birth there is a formed “protrusion” of the peritoneum, which turns into a hernial sac when elements of the abdominal contents first penetrate into it.
Inguinal region anatomy. MCPC Rusakov V.I. 1997 6
Acquired hernias go through all stages of development from expansion of the inguinal ring to a complete hernia. Inguinal-scrotal hernias are rare, and only in older men: patients consult a doctor early and promptly get rid of the hernia in the early stage of the disease.
There are also so-called combined hernias:
- 1) direct and oblique inguinal hernia,
- 2) direct inguinal hernia and supravesical hernia,
- 3) oblique and direct inguinal hernia and supravesical hernia.
Double inguinal hernias (oblique and direct) were described by N. A. Kukoverov (1928), N. I. Kukudzhanov (1949) and others. A similar observation was made in our clinic. The hernial sacs in such cases are separated from each other by the inferior epigastric artery.
Rare interstitial or parainguinal hernias also have a certain practical significance:
- 1) preperitoneal hernia—the hernial sac is located between the peritoneum and the transverse fascia; the hernial sac can have a different direction,
- 2) intramural hernia—the hernial sac partially passes through the inguinal canal and is located under the aponeurosis of the external oblique muscle or between the internal and transverse abdominal muscles,
- 3) superficial inguinal hernia—the hernial sac emerges from the superficial ring of the inguinal hernia and is located under the skin above the aponeurosis of the external oblique abdominal muscle or descends to the thigh and perineum. The types of peri-inguinal hernias are explained in Figure 45.
Inguinal region anatomy. MCPC Rusakov V.I. 1997 8
Preperitoneal hernias often have two pockets, one of which goes into the inguinal canal. Predisposing factors to the formation of preperitoneal inguinal hernias are a high inguinal space, a very narrow and unyielding superficial ring of the inguinal canal, looseness of the surrounding tissues and congenital protrusions of the peritoneum (E. P. Berezina, 1947; V. S. Mayat, 1947; N. I. Kukudzhanov , 1949).
Preperitoneal hernias, as well as interstitial ones, are most often recognized. are found during surgery for strangulation. However, there is reason to agree with Ficai et al. (1970) and with A. M. Lokhin (1971), who prove the possibility of preoperative recognition of this type of hernia.
An extremely rare inguinal hernia is the encysted hernia (hernia encystica), first described in 1833 by Cooper. The development of Cooper's hernia is associated with incomplete fusion of the peritoneal-inguinal process, which is divided along its length by a septum.
When a hernia forms, a double sac is formed: internal and external. During the development of a hernia, the internal sac seems to be invaded into the proximal part of the unfused peritoneal-inguinal process. Therefore, it is clear that the internal hernial sac is covered with a serous membrane on both sides. The contents of the external hernial sac are the internal hernial sac along with the organs that have prolapsed into it (Fig. 46).
Inguinal region anatomy. MCPC Rusakov V.I. 1997 9
There are two types of Cooper's hernia:
- 1) hernia encystica testicularis—formed as a testicular hernia, when there is a testicle in the external hernial sac;
- 2) hernia encystica funicularis—formed as a cord hernia. There may be a hole at the bottom of the internal sac, and then both sacs communicate with the abdominal cavity.
Knowledge of the given rare forms of inguinal hernias prevents diagnostic errors and errors during the operation.
Weakness of the pelvic floor muscles: problems and consequences
If your pelvic floor muscles are weak, you are at risk for the following problems:
- anorgasmia (loss of sensation and inability to experience sexual pleasure);
- urinary incontinence while walking, coughing, playing sports;
- prolapse and prolapse of the uterus outside the vagina;
- severe abdominal pain.
20% of women aged 21–29 years and 55% of women aged 30 to 40 experience certain symptoms associated with weakening of the pelvic muscles. In the age group over 45 years old, muscle weakness occurs in 75% of cases. If you ignore the problem, the condition progresses, causing complications.
Pain in the groin: what causes it
The most common cause of groin pain in women is inflammatory diseases of the genital area. The woman's general condition worsens, her body temperature rises, and pain occurs if she touches her stomach.
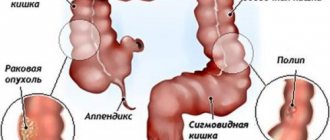
One of the common pathologies is appendicitis, which manifests itself as severe pain in the right groin. First, throbbing pain occurs in the epigastric region and eventually descends below. The patient begins to feel even worse during movement and experiences pain when lying on his left side. Other symptoms of appendicitis are nausea, vomiting, and problems with bowel movements.
Cystic formations affecting the internal genital organs cause pain in the groin area. They are characterized by nagging painful sensations and when the cyst ruptures they become more acute: the patient’s general condition worsens, vomiting occurs, body temperature rises, and blood pressure drops.
Severe pain in the groin bothers a woman during an ectopic pregnancy. The pain is cramping in nature and intensifies over time.
A rupture of a femoral artery aneurysm is expressed by intense pain in the groin and causes bleeding.
Intestinal diseases cause pain in the groin. In addition, malignant tumors, intestinal obstruction, and diverticulitis contribute to pain. The main symptoms of these pathologies: bloated stomach, problems with stool.
A stone stuck in the ureter causes pain on one side of the groin area. The painful sensations are acute and sharp in nature and last for several minutes or throughout the day. The pain is localized in the lumbar region, and the irradiation point is the groin.
When the lymph nodes in the groin become inflamed, pain occurs near the affected area. The node becomes thicker and becomes larger.
In rare cases, pain occurs due to an inguinal hernia, since in the female body the inguinal gap is not as wide as in men, and the tissue is stronger.
Muscle pain in the groin is mainly observed in female athletes after heavy exertion or competition. Muscles suffer in those who play volleyball, tennis and basketball. The pain is nagging or aching, but with injury it becomes more acute.
Pain in the groin area during movement is caused by a chronic form of hip disease. The symptom appears on one side of the groin, may begin while walking and disappear over time, but reappear during a long walk.
Pain in the groin also occurs in pregnant women; it develops for the following reasons:
- weakening of cartilage due to hormones;
- the fetus puts pressure on the pelvic bones;
- stretching and weakening of the ligaments that attach the uterus to the walls of the pelvis;
- increased myometrial tone and threat of miscarriage;
- deficiency of calcium and magnesium.
In addition to diseases that provoke pain in the groin area, the symptom occurs due to menstruation. The pain is cramping and aching in nature and begins a few days before menstruation. After the completion of menstrual flow, the pain syndrome disappears.
Indications for training
Training for pelvic floor muscle dysfunction is prescribed by a doctor after eliminating contraindications. Considering the structure of the organs located in the female pelvis, symptoms of muscle weakness can be determined independently. Indications for starting intimate ligament training are factors such as:
- Childbirth planning. Due to the strengthened muscular corset, the uterus will receive the necessary support, and the risk of prolapse or prolapse of the organ will be reduced.
- The period during pregnancy and after childbirth. Due to trained muscles, the birth process is accelerated and facilitated, and the risk of perineal ruptures is reduced. After childbirth, the genitals will quickly recover to their previous state.
- Age over 30 years. Most women have weakened pelvic floor muscles with age if they are not trained. To avoid problems in the future, even in the absence of unpleasant symptoms, gymnastics of the intimate muscles is indicated.
- Injuries and surgeries in the female pelvic floor. In this case, the natural contraction of muscles is disrupted, and with it the transmission of nerve impulses. As a result, incontinence, anorgasmia and other problems develop.
- Hormonal disbalance. Poor blood circulation due to metabolic disorders leads to thinning of the vaginal walls and a decrease in its elasticity.
- Physical inactivity. A sedentary lifestyle leads to loss of elasticity and muscle tone. They contract worse, which affects the functioning of all pelvic organs.
Advantages of ultrasound of the inguinal canals in our clinic
- We save your time. Arrive at a predetermined time, complete the test without wasting time in queues, and receive a decrypted result in just five minutes.
- We guarantee accurate results. We use a high-precision ultrasound scanner Mindray DC-8. The high level of training of specialists allows us to guarantee a high-quality examination.
- We detect the disease in its early stages. The study allows us to identify abnormalities characteristic of the disease at an early stage and quickly begin treatment. This makes therapy more effective and cheaper.
- We treat patients with care. Ultrasound examination is completely safe, painless and does not cause discomfort. An ultrasound of the groin area can be done at any age.
- We conduct research at home. If you are unable to come to the clinic, call us. A portable ultrasound scanner allows you to conduct studies at home.
Contraindications to strengthening the pelvic muscles
Physical exercise has contraindications, so you must first consult a gynecologist or other specialized specialist so as not to harm your health. You should not do exercises for the perineum in the following cases:
- damage to the mucous membranes of the vagina and uterus;
- chronic diseases at the time of exacerbation (cystitis, endometritis);
- recent surgeries on the pelvic organs;
- the presence of neoplasms of any type;
- erosion of the uterine wall;
- pathologies of the heart and blood vessels.
Other contraindications relate to increased uterine tone, the risk of miscarriage and premature birth.
What is it and how does it work
Ultrasound of the inguinal canals is a procedure that is performed to identify inguinal hernias and distinguish them from varicoceles; identify a spermatic cord cyst (funiculocele), inguinal lymphadenitis or tumors of the testicle and its appendages.
Ultrasound radiation is reflected from the patient's tissues at different frequencies and returns to the receiver. The computer converts the ultrasonic waves into a picture, which is displayed on the screen. After studying the image, the doctor deciphers it and draws conclusions.
Usually, an ultrasound of the inguinal canals is combined with an examination of the abdominal cavity and pelvis to find out what exactly is in the hernial sac. The procedure does not cause any discomfort, is absolutely safe and takes ten to fifteen minutes.
How is the operation performed?
Surgery begins with preparation. At this stage, the patient undergoes certain tests repeatedly. He is prescribed a complex of minerals and vitamins. Such a diet will prepare the body for the stress that lies ahead during surgery.
In the preoperative period, it is strictly forbidden to take drugs that negatively affect blood clotting. One week before surgery, you must stop taking any contraceptives. Alcoholic drinks and tobacco products are prohibited. The patient is advised to spend a long time in the fresh air.
The doctor chooses anesthesia based on the individual characteristics of the body. During the operation the following types of anesthesia are used:
- local;
- general;
- regional.
If the patient experiences a strong feeling of anxiety, he is prescribed sedatives. During the intervention, laparoscopy or open surgery is performed. In the latter case, the surgeon makes an incision, which allows access to the problem area. If the output of internal organs is insignificant, then the contents are corrected. In emergency cases, the surgeon can remove damaged tissue.
Laparoscopy involves making small punctures through which surgical equipment is inserted. This method allows to minimize damage to skin tissue and significantly shorten the patient’s rehabilitation period.
Indications for ultrasound of the inguinal canals
Ultrasound of the inguinal canals is prescribed for suspected inguinal hernias in order to detect the hernial sac, assess its size, contents and condition of the inguinal canal. Inguinal hernias are characterized by the following symptoms:
- the appearance of a protrusion in the groin area;
- enlargement of one of the testicles or half of the scrotum in men;
- enlargement of one of the labia in women;
- the appearance of pain in the groin area;
- nausea and vomiting;
- stool retention.
Treatment of groin pain in women
To treat groin pain, a woman should follow a strict diet. Exclude fried, flour, sweet, salty and smoked foods from the menu. Eat plant-based foods. Limit your intake of fats and carbohydrates. Steamed fish and meat, fruits and vegetables are suitable. Be sure to drink clean drinking water. Salt should be excluded, as pain in the groin may indicate kidney problems. It is advisable to include physical therapy and massage in your daily routine after a doctor’s prescription.
Drug treatment should not be started without visiting a doctor. At the KDS Clinic you will be referred for blood, stool, urine and biochemistry tests. It is necessary to do an ultrasound diagnosis of the pelvic organs. In some cases, magnetic resonance imaging is used to obtain a clearer effect, however, this procedure has a number of contraindications. It is prohibited:
- Children under sixteen years of age. The child’s body is not yet strong, so the radiation will damage healthy organs.
- Pregnancy. During pregnancy, magnetic resonance imaging is strictly prohibited. It will harm the development of the fetus.
- Lactation period.
Is it possible to cure an inguinal hernia without surgery?
The organs extend beyond the peritoneum through an opening created artificially or as a result of anatomical changes. To eliminate it, suturing is necessary. This means that treatment of the pathology is not possible without surgery to remove an inguinal hernia in women. Today, hernioplasty is performed for this purpose - the only effective method for eliminating various types of hernias.
Treatment also includes conservative therapy. It is aimed at stopping the development of the pathological process, as well as preventing the occurrence of complications. Treatment in the preoperative period is possible if there are some contraindications: the patient’s advanced age and severe decompensated condition. Only in such cases is treatment of inguinal hernia in women considered without surgery.
Inguinal hernia - symptoms and treatment
Any inguinal hernia is subject to surgical treatment. No other methods - taking medications, wearing bandages, following the advice of healers, fortune tellers and other adherents of alternative medicine - will eliminate it.
If there is an inguinal hernia, it must be operated on routinely in the surgical department. If an inguinal hernia is suddenly strangulated, the operation procedure changes to emergency. Ideally, the operation should be performed within two hours from the moment of infringement. So it’s better to put fears aside and solve the problem as early as possible.
Now let's look at the types of operations used to treat inguinal hernia. Putting aside the historical aspects and dozens of previously proposed proprietary techniques that are already being used, we can say: there are actually 3-4 methods left for plastic surgery of the inguinal canal. There is an open method and a laparoscopic one.
An open or external method of hernia repair is when, under general or spinal (but not local, this is also a thing of the past!) anesthesia, a 6-8 cm long incision is made in the groin area, and the inguinal canal is opened. Then the hernia is eliminated - by isolating, opening and excising the hernial sac, returning the hernial contents (intestine, omentum or bladder) to its place in the abdominal cavity. Next comes the most important part of the operation - strengthening, or plastic surgery of the inguinal canal. All the variability of the author's proposals lay precisely in this stage. Nowadays, the Lichtenstein method is almost always used, which involves sewing a polypropylene mesh implant into the back wall of the inguinal canal.[2][3][10]
Polypropylene is practically the same material that fishing line is made from, only thinner, more flexible and properly sterilized. It is very durable, does not dissolve, and its rupture is practically impossible. The mesh size is selected individually. The mesh is attached with separate sutures to the strong tendon structures of the groin area. The duration of the operation is on average from 30 minutes to 2 hours. The method is reliable: 95-98% probability of no relapse.[2][3][7][10] Among the nuances is the possibility of local wound complications (the formation of fluid accumulations near the mesh, the possibility of wound suppuration, pain after surgery, and sometimes persistent long-term pain associated with damage to the nerve trunks passing in the operation area).
Laparoscopic method of hernia repair. The full name is transperitoneal preperitoneal laparoscopic hernioplasty (TAPP in its English abbreviation) and total extraperitoneal inguinal hernioplasty (TEP).[1][4][10] Preferred over open method. The most modern, advanced and reliable method of getting rid of an inguinal hernia. It was first tested in 1991 in Europe, and has been widely used clinically in Russian medicine relatively recently—for 10 years. It is not performed in every clinic (an expensive laparoscopic stand and instruments are required) and not by every specialist (a certain level of training and experience is required). It is performed under general anesthesia, like any laparoscopic operation. Three incisions and punctures of the abdominal wall are made, 1-1.5 cm long. Carbon dioxide is injected into the abdominal cavity (it’s safe!), followed by the introduction of a video camera and special long instruments through special hollow tubes (trocars). During the operation, the hernia is eliminated from the inside, from the abdominal cavity. Then a mesh implant is installed from the inside (there are variations, but in general it corresponds to what is installed using the open method). The anatomical layer of mesh installation - preperitoneal - differs from the open method. The size of the mesh installed during laparoscopy is larger than with the open Lichtenstein method - on average 15x10 cm. And, what is very important, the zone of anatomical overlap of the mesh is also larger and covers the potential exit sites of 3 hernias - oblique inguinal, direct inguinal and femoral on the corresponding side. The mesh is attached with special staples to the tendon structures of the groin area and is closed from the inside by the peritoneal membrane to prevent the formation of adhesions. The reliability of the method is very high: the probability of relapse is 1-5%.[5][6][7][9][10] The advantages of the laparoscopic technique, in addition to high reliability, are also: high cosmetic effect (small incisions heal with the formation of almost imperceptible scars), low incidence of wound complications, lower level of pain, quick - within one day - mobilization of the patient, shorter stay in the hospital .[4][6][8][9]