Overdose
According to reviews of Bellaspon, an overdose of the drug is manifested by a number of symptoms, including: diarrhea, nausea, thirst, vomiting, chills, unconsciousness, convulsions, cardiovascular disorders, peripheral vasoconstriction.
Chronic overdose may occur in patients with hypersensitivity. In case of chronic overdose, circulatory disorders, trophic disorders in the periphery, and sometimes gangrene of the fingers are observed. Blood pressure changes, arrhythmias, anginal pain, convulsions, and clouding of consciousness appear. An overdose can result in coma with severe suppression of cardiovascular activity, renal failure, hypotension, shock, and sometimes even death.
To treat an overdose, symptomatic therapy with preliminary gastric lavage is used.
In case of chronic intoxication, it is sufficient to stop taking Bellaspon.
In particularly severe cases, it is necessary to maintain adequate blood flow in the damaged areas in order to prevent the development of gangrene. Maintenance therapy should be aimed at maintaining normal activity of the cardiovascular system, kidneys, and maintaining electrolyte balance.
Contraindications
According to the instructions, Bellaspon is not prescribed for:
- porphyria;
- glaucoma;
- hypersensitivity to the components of the drug;
- severe disorders of the kidneys and liver;
- severe atherosclerosis;
- arterial hypertension;
- strong increase in body temperature;
- prostate hypertrophy;
- respiratory failure;
- drug or alcohol dependence;
- under 6 years of age, during pregnancy and breastfeeding.
Experience with the use of Bellataminal in patients with gastrointestinal diseases
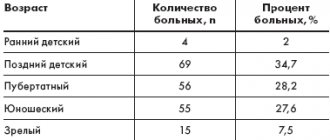
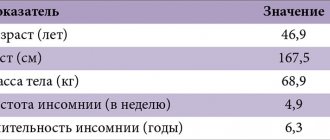
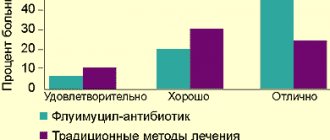
Diseases of the gastrointestinal tract (GIT) in 45–90% of cases lead to damage to the nervous system. The nervous system in diseases of the gastrointestinal tract is involved primarily at the beginning of the formation of somatic pathology, determining neurosomatic mechanisms, and secondarily as a manifestation of somato-neurological disorders. Patients with this pathology experience psychopathological disorders in the form of anxiety and depressive disorders, as well as autonomic dysfunctions predominantly at the suprasegmental level. Dysfunction of the autonomic nervous system (ANS) is considered as a pathogenetic factor in non-infectious gastrointestinal pathology. The connection between the ANS and gastroduodenal motility, which plays an important role in the development of gastroduodenal pathology (GDP), has been studied. One of the reasons for the chronicity of the pathological process in the mucous membrane of the gastroduodenal zone is sphincter disorders, the manifestations of which are duodenogastric reflux (DGR) and gastroesophageal reflux (GER). In the development of sphincter disorders, a priority role is given to dysfunction of the ANS [7]. A relationship has been established between the state of the parasympathetic division of the ANS and the presence of GDR in patients with chronic gastroduodenitis (CGD). In the pathogenesis of chronic gastroduodenal pathology (CGDP), an important role is given to the functioning of the ANS, because It has been proven that CGDP occurs as a result of the depletion of protective and adaptation mechanisms. The prevalence of parasympathetic regulation, leading to disruption of the secretory-motor function of the stomach, is considered as a possible mechanism for the formation of HDP. Violation of the trophism of the gastric mucosa is explained by a decrease in the activity of the sympathetic component of the ANS [2,4,6,9]. Materials and methods of research. Clinical examination of patients was carried out using standard methods and included analysis of anamnestic information, assessment of complaints, neurological and somatic status, and psychological testing of a number of features of the emotional sphere. In order to exclude organic changes in the somatic sphere of patients, a comprehensive laboratory and instrumental examination was carried out. Ultrasound of the abdominal organs with cholecystoscopy and esophagogastroduodenoscopy (EFGDS) were used. Laboratory diagnostic methods included standard studies of hemogram, urogram, coprogram, basic biochemical parameters of blood serum (total protein, albumin, bilirubin, liver transaminases, glucose, amylase, alkaline phosphatase, electrolytes). We used rapid diagnostics of Helicobacter pylori infection using the HELIK test system. All patients underwent a comprehensive examination before and after completion of the course of therapy, which included an assessment of the state on the Spielberger-Khanin scale of reactive and personal anxiety, which allows one to judge the severity of changes, a study of autonomic dysfunction (questionnaires edited by A.M. Vein), and a scoring questionnaire was used subjective characteristics of sleep (edited by V.L. Golubev, 2010). Research results. 31 patients (12 boys, 19 girls) aged 17–18 years were observed. Their main complaints were abdominal pain, heartburn and belching. Pain syndrome was observed in 100% of patients, while heartburn was noted by 13 (41.9%), belching – by 23 (74%), not only with air, but also with sour or bitter air. Quite often, patients had complaints such as heaviness and discomfort in the abdomen and nausea: 12 (38.7%), 6 (19.3%) and 13 (54.8%), respectively; 8 patients (25.8%) complained of bitterness in the mouth. These complaints are characteristic signs of impaired motility of the upper digestive tract. The defining symptoms of impaired motility of the lower digestive tract were flatulence - in 4 (12.9%) and pathological frequency of stool - in 10 (32%) of those examined. Based on the results of EGD, an analysis of endoscopic changes in the mucous membrane of the upper gastrointestinal tract in patients included in the study was carried out. All of them had inflammatory changes of varying severity in the esophagus, stomach and duodenum. Inflammatory changes in the mucous membrane of the esophagus were represented by catarrhal esophagitis (1st degree esophagitis) in 3 (9.7%) patients. In 1 (3.2%) patient, erosive changes in the esophageal mucosa were detected - single erosions (2nd degree esophagitis). Motor disturbances in the area of the cardioesophageal junction in the form of cardia insufficiency and GER were detected according to EGD data in 3 (9.7%) and 1 (3.2%) patient, respectively. Endoscopically visualized superficial gastritis - in 14 (45.1%), follicular gastritis - in 1 (3.2%), superficial gastritis and superficial duodenitis - in 16 (51.6%) people. Motility disorders in the pyloroduodenal zone in the form of DGR according to EGD data were more common - they were observed in 11 (35.4%) patients, pyloric sphincter insufficiency was determined in 8 (25.8%) patients. Biliary dysfunction was confirmed by echography in 100% of those examined. In 29.1% of patients, Helicobacter pylori infection was detected using a urease breath test. The girls were characterized by emotional lability, tearfulness, unstable mood, suspiciousness, and a tendency to dramatize their condition. In young men, irritability, hot temper, a decrease in the degree of self-control, and a pessimistic assessment of their condition predominated. Taking into account the emotional state of patients, Bellataminal was added to the basic treatment of gastrointestinal diseases - a combination drug containing belladonna alkaloids, phenobarbital and ergotamine, which has α-adrenergic blocking, M-anticholinergic and sedative properties. The drug was prescribed 1 tablet 2 times a day. All patients had sleep disturbances (difficulty falling asleep, shallow night sleep). A score was made for the time of falling asleep, duration of sleep, presence of night awakenings, dreams, quality of sleep, quality of awakening before and after the use of Bellataminal (Table 1). During the treatment, there was a significant improvement in the quality of sleep of patients, which had a positive effect on psycho-vegetative manifestations. Autonomic dysfunction of varying severity was observed in all patients before taking Bellataminal in complex therapy. The severity according to subjective criteria was 48.7±1.83; according to objective indicators, the average score was 50.5±2.14. After using the drug, there was a decrease in the manifestations of autonomic lability both in subjective (34.4±1.9; p<0.05) and (32.5±2.04; p<0.05) objective indicators. When assessing the level of anxiety before using Bellataminal, both reactive and personal anxiety also prevailed (Table 2). The results presented in the table indicate that treatment with Bellataminal led to a significant improvement in indicators of personal and reactive anxiety. Conclusion. A chronic inflammatory process that develops in the entire body system causes disorders of the nervous system. In this regard, patients of childhood and adolescence with diseases of the digestive system are characterized by emotional lability, anxiety disorders, and sleep disorders. An important link in the formation of pathology of the digestive system is dysfunction of the ANS. The use of Bellataminal in the complex therapy of gastrointestinal diseases leads to a marked reduction in the manifestations of autonomic dysfunction, personal and reactive anxiety, as well as normalization of the gastrointestinal tract. The complex use of medications in combination with the normalization of physical and neuropsychic stress can significantly reduce the number of esophagitis and gastroesophageal reflux disease and the development of complications that arise from this pathology in patients of childhood and adolescence.
Literature 1. Autonomic disorders: Clinic, treatment, diagnosis / ed. A.M. Veina. M.: Medical Information Agency, 1998. 752 p. 2. Belmer S.V., Gasilina T.V., Khavkin A.I., Eiberman A.S. Functional disorders of the digestive system in children. M.: RGMU, 2005. 36 p. 3. Lobakov A.I., Belousova E.A. Abdominal pain: difficulties of interpretation and methods of relief // Medical newspaper. 2001. No. 05. 4. Rational pharmacotherapy of diseases of the digestive system: A guide for practicing physicians. / Under the general editorship. V.T. Ivashkina. M.: Litterra, 2003. 1046 p. 5. Somatoneurology: a guide for doctors / ed. A.A. Skoromets. St. Petersburg: SpetsLit, 2009. 655 p. 6. Khavkin A.I., Belmer S.V., Volynets G.V., Zhikhareva N.S. Functional diseases of the digestive tract in children. Principles of rational therapy // Pediatrician's Handbook. 2006. No. 2. P. 17–32. 7. Shcherbakov P.L. Gastroesophageal reflux disease in children // Diseases of the digestive organs. 2007. T. 9. No. 2. P. 42–47. 8. Gottrand F. The role of Helicobacter pylori in abdominal pain in children // Arch Pediatr. 2000 Feb. Vol. 7(2). R. 197–200. 9. Rasquin–Weber A., Hyman PE, Cucchiara S., Fleisher DR, Hyams JS, Milla PJ, Staiano Childhood functional gastrointestinal disorders // Gut. 1999. Vol. 45. Suppl. 2.P. 1160–1168.
Interaction with other drugs
Bellaspon significantly weakens or suppresses the effect of indirect anticoagulants, thymoleptics, glucocorticoids, oral contraceptives, cardiac glycosides, sex hormones, quinidine, doxycycline.
Bellaspon enhances the effect and toxicity of chloral hydrate, pethidine, methotrexate, cyclophosphamide, 6-mercaptopurine.
When administered simultaneously with sympathomimetics, the vasoconstrictor effect of ergotamine is enhanced. Parallel use of antirheumatic and cortisone-like drugs, salicylates increases the likelihood of damage to the gastric mucosa.
Bellaspon enhances the effect of substances that inhibit the central nervous system. But a weakening of their action may also be observed due to increased enzymatic activity.
Long-term use of the drug during anesthesia with fluorothane or enflurane may increase the risk of toxic effects on the liver.
Alcohol, hydantoin, valproic acid, urine acidifiers, oral antidiabetic drugs, MAO inhibitors enhance the effect of phenobarbital.
The effect of phenobarbital is reduced by antacids, cholestyramine, phenylbutazone, and drugs that alkalinize urine.
special instructions
During treatment with Bellaspon, the consumption of alcoholic beverages is not recommended.
When taking Bellaspon, you should not engage in activities that require increased concentration, high speed of psychomotor reactions, or coordination of movements.
When prescribing the drug to persons with anemia, hyperthyroidism or the elderly, the potential risks and benefits of using the drug should be weighed.
After long-term use of Bellaspon (several months), the dosage of the drug should be gradually reduced, since it is addictive.
If there is a need to take the drug, breastfeeding women should stop breastfeeding.
Side effects
According to reviews, Bellaspon can cause side effects in the form of:
- mild mental disorders, decreased visual acuity, paresthesia;
- itching, urticaria, skin rashes;
- sensations of dry mouth, drowsiness, nausea, constipation, vomiting.
With prolonged use of the drug, drug dependence may occur.
Also, reviews of Bellaspon note isolated cases of loss of taste, appetite, trembling, edema, cyanosis, muscle weakness, clouding of consciousness in elderly patients.