Topamax, 60 pcs., 25 mg, capsules
The effect of Topamax® on the concentrations of other antiepileptic drugs (AEDs)
Concomitant use of Topamax® with other AEDs (phenytoin, carbamazepine, valproic acid, phenobarbital, primidone) does not affect their plasma Css values, with the exception of certain patients in whom the addition of Topamax® to phenytoin may cause an increase in plasma phenytoin concentrations . This may be due to inhibition of a specific polymorphic isoform of the enzyme of the cytochrome P450 system (CYP2C19 isoenzyme). Therefore, phenytoin plasma concentrations should be monitored in any patient taking phenytoin who develops clinical signs or symptoms of toxicity.
In a pharmacokinetic study in patients with epilepsy, the addition of topiramate to lamotrigine did not affect the latter's Css at doses of topiramate 100–400 mg/day. During therapy and after discontinuation of lamotrigine (average dose 327 mg/day), Css of topiramate did not change.
Impact of other AEDs on the concentration of Topamax®
Phenytoin and carbamazepine reduce plasma concentrations of Topamax®. The addition or removal of phenytoin or carbamazepine during treatment with Topamax may require a change in the dose of the latter. The dose should be selected based on achieving the desired clinical effect. The addition or removal of valproic acid does not cause clinically significant changes in the plasma concentration of Topamax® and therefore does not require a change in the dose of Topamax®. The results of these interactions are summarized in Table 1.
Table 1
| Added PEP | PEP concentration | Topamax® drug concentration |
| Phenytoin | 1 ** | $ (48%) |
| Carbamazepine | 1 | $ (40%) |
| Valproic acid | 1 | 1 |
| Phenobarbital | 1 | NI |
| Primidon | 1 | NI |
1 - No effect.
** - Increased concentration in isolated patients.
$ - Decreased plasma concentration.
NI - Not studied.
Other drug interactions
Digoxin.
In a single-dose study, the plasma AUC of digoxin decreased by 12% when coadministered with Topamax®. The clinical significance of this observation is unclear. When prescribing or discontinuing Topamax® in patients taking digoxin, special attention should be paid to monitoring the concentration of digoxin in the serum.
CNS depressants.
In clinical studies, the consequences of simultaneous use of Topamax® with alcohol or other substances that depress the functions of the central nervous system have not been studied. It is not recommended to take Topamax® together with alcohol or other drugs that cause depression of central nervous system function.
St. John's wort.
When taking Topamax together with drugs based on St. John's wort
(Hypericum perforatum),
the plasma concentration of topiramate may decrease and, as a result, the effectiveness of the drug may also decrease. Clinical studies of the interaction of Topamax® and drugs based on St. John's wort have not been conducted.
Oral contraceptives.
In a drug interaction study with oral contraceptives using a combination product containing norethisterone (1 mg) and ethinyl estradiol (35 mcg), Topamax® at doses of 50–800 mg per day did not have a significant effect on the effectiveness of norethisterone and at doses of 50–200 mg per day - on the effectiveness of ethinyl estradiol. A significant dose-dependent decrease in the effectiveness of ethinyl estradiol was observed at doses of Topamax® 200–800 mg per day. The clinical significance of the described changes is unclear. The risk of decreased contraceptive effectiveness and increased breakthrough bleeding should be considered in patients taking oral contraceptives in combination with Topamax®. Patients taking estrogen-containing contraceptives should be informed of any changes in the timing and pattern of menstruation. The effectiveness of contraceptives may be reduced even in the absence of breakthrough bleeding.
Lithium.
In healthy volunteers, a decrease in lithium AUC by 18% was observed while taking topiramate at a dose of 200 mg/day. In patients with manic-depressive psychosis, the use of topiramate in doses up to 200 mg/day did not affect the pharmacokinetics of lithium, however, at higher doses (up to 600 mg/day), the AUC of lithium was increased by 26%. When using topiramate and lithium simultaneously, the concentration of the latter in the blood plasma should be monitored.
Risperidone.
Drug interaction studies with single and multiple doses of topiramate in healthy volunteers and patients with bipolar disorder yielded similar results. When coadministered with topiramate at doses of 250 or 400 mg/day, the AUC of risperidone taken in doses of 1–6 mg/day is reduced by 16 and 33%, respectively. At the same time, the pharmacokinetics of 9-hydroxyrisperidone did not change, and the total pharmacokinetics of the active substances (risperidone and 9-hydroxyrisperidone) changed slightly. The change in systemic exposure of risperidone/9-hydroxyrisperidone and topiramate was not clinically significant and this interaction is unlikely to be of clinical significance.
Hydrochlorothiazide.
Drug interactions were assessed in healthy volunteers with the separate and combined use of hydrochlorothiazide (25 mg) and topiramate (96 mg). Study results showed that when topiramate and hydrochlorothiazide were taken concomitantly, the topiramate Cmax increased by 27% and the topiramate AUC increased by 29%. The clinical significance of these studies has not been established. Prescribing hydrochlorothiazide to patients taking topiramate may require a dose adjustment of topiramate. The pharmacokinetic parameters of hydrochlorothiazide were not significantly altered by concomitant therapy with topiramate.
Metformin.
Drug interactions were assessed in healthy volunteers receiving metformin or a combination of metformin and topiramate. Study results showed that when topiramate and metformin were taken concomitantly, the Cmax and AUC of metformin increased by 18 and 25%, respectively, while the clearance of metformin when used concomitantly with topiramate decreased by 20%. Topiramate had no effect on metformin plasma Tmax. The clearance of topiramate is reduced when used concomitantly with metformin. The extent of the observed changes in clearance has not been studied. The clinical significance of the effect of metformin on the pharmacokinetics of topiramate is unclear. If Topamax® is added or discontinued in patients receiving metformin, the patient's condition should be carefully monitored to assess the course of diabetes mellitus.
Pioglitazone.
Drug interactions were assessed in healthy volunteers with the separate and simultaneous use of pioglitazone and topiramate. A decrease in the AUC of pioglitazone by 15% was detected, without changing the Cmax of the drug. These changes were not statistically significant. For the active hydroxymetabolite pioglitazone, a decrease in Cmax and AUC was also detected by 13 and 16%, respectively, and for the active ketometabolite, a decrease in both Cmax and AUC was detected by 60%. The clinical significance of these data is unclear. When patients use Topamax® and pioglitazone simultaneously, the patient's condition should be carefully monitored to assess the course of diabetes mellitus.
Glibenclamide.
A drug interaction study was conducted to examine the pharmacokinetics of glibenclamide (5 mg/day) at steady state, administered alone or concomitantly with topiramate (150 mg/day) in patients with type 2 diabetes mellitus. When topiramate was used, the AUC of glibenclamide was reduced by 25%. Systemic exposure to 4-trans-hydroxy-glibenclamide and 3-cis-hydroxy-glibenclamide was also reduced (by 13 and 15%, respectively). Glibenclamide did not affect the pharmacokinetics of topiramate at steady state. A statistically insignificant decrease in the AUC of pioglitazone by 15% was found with no change in Cmax. When prescribing topiramate to patients receiving glibenclamide (or prescribing glibenclamide to patients receiving topiramate), the patient's condition should be carefully monitored to assess the course of diabetes mellitus.
Other drugs.
Concomitant use of Topamax® with drugs that predispose to nephrolithiasis may increase the risk of kidney stones. During treatment with Topamax®, the use of drugs that predispose to nephrolithiasis should be avoided, as they may cause physiological changes that contribute to nephrolithiasis.
Valproic acid.
The combined use of topiramate and valproic acid in patients who tolerate each drug separately is accompanied by hyperammonemia with or without encephalopathy. In most cases, symptoms and signs disappear after stopping one of the medications. This adverse event is not due to a pharmacokinetic interaction. The relationship between hyperammonemia and the use of topiramate alone or in combination with other drugs has not been established. When topiramate and valproic acid are taken together, hypothermia (an unintentional decrease in body temperature below 35 °C) may occur in combination with hyperammonemia or independently. This phenomenon can occur both after the start of co-administration of valproic acid and topiramate, and with an increase in the daily dose of topiramate.
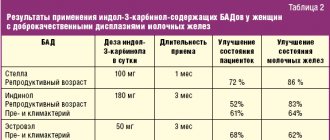
Additional drug interaction studies: A number of clinical studies have been conducted to evaluate potential drug interactions between topiramate and other drugs. The results of these interactions are summarized in Table 2.
table 2
| Added drug | Concentration of added drug* | Topiramate concentration* |
| Amitriptyline | Increase in Cmax and AUC of nortriptyline metabolite by 20% | NI |
| Dihydroergotamine (oral and s.c.) | 1 | 1 |
| Haloperidol | Increase in metabolite AUC by 31% | NI |
| Propranolol | Increase in Cmax for 4-OH propranolol by 17% (topiramate 50 mg) | Increase in Cmax by 9 and 16%; AUC of 9 and 17% for propranolol 40 and 80 mg every 12 hours, respectively |
| Sumatriptan (oral and subcutaneous) | 1 | NI |
| Pizotifen | 1 | 1 |
| Diltiazem | Reduced AUC of diltiazem by 25% and desacetyldiltiazem by 18%; 1 for N-demethyldilthiazem | Increase AUC by 20% |
| Venlafaxine | 1 | 1 |
| Flunarizine | Increase in AUC by 16% (50 mg every 12 hours)** | 1 |
* — Expressed as % of Cmax values in blood plasma and AUC during monotherapy.
1 - No changes in plasma Cmax and AUC (<15% of baseline data).
** With multiple doses of flunarizine alone, a 14% increase in AUC was observed, which may be due to drug accumulation during the process of reaching steady state.
NI - not studied.
Topamax® (Topamax®)
The effect of Topamax® on the concentrations of other antiepileptic drugs (AEDs)
Concomitant use of the drug Topamax® with other AEDs (phenytoin, carbamazepine, valproic acid, phenobarbital, primidone) does not affect the values of their equilibrium concentrations in plasma, with the exception of certain patients in whom the addition of the drug Topamax® to phenytoin may cause an increase in the concentration of phenytoin in the plasma. plasma. This may be due to the inhibition of a specific polymorphic isoform of the cytochrome P450 enzyme (CYP2Cmeph). Therefore, phenytoin plasma concentrations should be monitored in any patient taking phenytoin who develops clinical signs or symptoms of toxicity. In a pharmacokinetic study in patients with epilepsy, the addition of topiramate to lamotrigine did not affect the steady-state concentration of the latter at doses of topiramate 100-400 mg per day. During and after discontinuation of lamotrigine (average dose 327 mg per day), the equilibrium concentration of topiramate did not change.
Effect of other antiepileptic drugs on the concentration of Topamax®
Phenytoin and carbamazepine reduce plasma concentrations of Topamax®. The addition or removal of phenytoin or carbamazepine during treatment with Topamax® may require a change in the dose of the latter. The dose should be selected based on achieving the desired clinical effect.
The addition or removal of valproic acid does not cause clinically significant changes in the plasma concentration of Topamax® and, therefore, does not require a change in the dose of Topamax®.
The results of these interactions are summarized in the following table:
| Added PEP | PEP concentration | Topamax ® concentration |
| Phenytoin | ↔** | ↓ (48%) |
| Carbamazepine | ↔ | ↓ (40%) |
| Valproic acid | ↔ | ↔ |
| Phenobarbital | ↔ | NI |
| Primidon | ↔ | NI |
↔ = No effect
** = Increased concentration in isolated patients
↓ = Decrease in plasma concentration
NI = Not studied
AED = antiepileptic drug
Other drug interactions
Digoxin:
In a single-dose study, the area under the breakthrough bleeding curve should be taken into account in patients taking oral contraceptives in combination with Topamax®. Patients taking estrogen-containing contraceptives should be informed of any changes in the timing and nature of menstruation. The effectiveness of contraceptives may be reduced even in the absence of breakthrough bleeding.
Lithium:
In healthy volunteers, a decrease in lithium AUC by 18% was observed while taking topiramate at a dose of 200 mg per day. In patients with manic-depressive psychosis, the use of topiramate in doses up to 200 mg per day did not affect the pharmacokinetics of lithium, however, at higher doses (up to 600 mg per day), the AUC of lithium was increased by 26%. When using topiramate and lithium simultaneously, the concentration of the latter in the blood plasma should be monitored.
Risperidone
: Drug interaction studies conducted with single and multiple doses of topiramate in healthy volunteers and patients with bipolar disorder yielded similar results. With simultaneous use of topiramate in doses of 250 or 400 mg per day, the AUC of risperidone, taken in doses of 1-6 mg per day, is reduced by 16% and 33%, respectively. At the same time, the pharmacokinetics of 9-hydroxyrisperidone did not change, and the total pharmacokinetics of the active substances (risperidone and 9-hydroxyrisperidone) changed slightly. The change in systemic exposure of risperidone/9-hydroxyrisperidone and topiramate was not clinically significant and this interaction is unlikely to be of clinical significance.
Hydrochlorothiazide
: Drug interactions were assessed in healthy volunteers with the separate and combined administration of hydrochlorothiazide (25 mg) and topiramate (96 mg). The results of the studies showed that with simultaneous administration of topiramate and hydrochlorothiazide, there is an increase in the maximum concentration of topiramate by 27% and the area under the curve "conkonkonkoncon" This adverse reaction is not due to a pharmacokinetic interaction.
When topiramate and valproic acid are taken together, hypothermia (an unintentional decrease in body temperature below 35 ° C) may occur in combination with hyperammonemia or independently. This phenomenon can occur either after starting to take valproic acid and topiramate together, or when the daily dose of topiramate is increased.
Additional drug interaction studies: A number of clinical studies have been conducted to evaluate potential drug interactions between topiramate and other drugs.
The results of these interactions are summarized in the following table:
| Added drug | Concentration of added druga | Topiramate concentration |
| Amitriptyline | increase in maximum concentration and AUC of nortriptyline metabolite by 20% | not studied |
| Dihydroergotamine (oral and subcutaneous) | ↔ | ↔ |
| Haloperidol | increase in metabolite AUC by 31% | not studied |
| Propranolol | increase in maximum concentration for 4-OH propranolol by 17% (topiramate 50 mg) | increase in maximum concentration by 9% and 16%, increase in AUC by 9 and 17%, (for propranolol 40 mg and 80 mg every 12 hours) respectively |
| Sumatriptan (oral and subcutaneous) | ↔ | not studied |
| Pizotifen | ↔ | ↔ |
| Diltiazem | 25% reduction in diltiazem AUC and 18% reduction in desacetyldiltiazem, and ↔ for N-demethyldiltiazem | AUC increase by 20% |
| Venlafaxine | ↔ | ↔ |
| Flunarizine | 16% increase in AUC (50 mg every 12 hours)b | ↔ |
a is expressed as a percentage of the values of maximum plasma concentration and AUC during monotherapy
↔ = No change in maximum plasma concentration and AUC (≤15% of baseline data)
b A 14% increase in AUC was observed with multiple doses of flunarizine alone, which may be due to drug accumulation during steady state.
Experience with the use of topiramate in children and adults
In the last decade, many new original antiepileptic drugs (AEDs) have been synthesized, which are included in the daily clinical practice of both pediatric and adult epileptologists. The main goal of modern pharmacology in the treatment of epilepsy is to create an “ideal” drug that suppresses not only seizures, but also has a true antiepileptogenic effect with a maximum efficacy/tolerability ratio. The increase in the number of AEDs significantly expands the possibilities in the treatment of epilepsy, especially in drug-resistant forms, and at the same time puts the doctor in a difficult position in choosing an adequate drug. The situation gets worse with the advent of each new drug, since patients with drug-resistant epilepsy may experience transient improvement after taking each of the newly prescribed AEDs, and this creates the illusion of their effectiveness. At the same time, only the accumulation of experience in the use of these drugs makes it possible to expand the group of AEDs. New drugs showed better tolerability, lower potential for interaction with other AEDs; in addition, they are easier to use. One such drug is topiramate (Topamax).
Topamax belongs to the class of sulfamate-substituted monosaccharides. The action of the drug is due to several mechanisms: blockade of voltage-dependent calcium and sodium channels (preventing the activation of GABAergic transmission), suppression of excitation mediators (glutamate), inhibition of carbonic anhydrase. Thus, the imbalance of the inhibitory GABAergic and excitatory glutamatergic systems is corrected. Thanks to this effect, the range of use of the drug for various forms of epilepsy, both in the form of mono- and as part of complex therapy, is expanding.
Topamax is characterized by linear pharmacokinetics and rapid absorption; at doses up to 200 mg/day it is not metabolized in the liver. Since the half-life is approximately 21 hours, the optimal dose is 1-2 times a day, regardless of meals. Topamax has no effect on the concentration of other AEDs, which, in turn, do not affect its therapeutic activity. The disadvantages of Topamax include slow titration. The “therapeutic window” of the drug is very wide - from 2 to 10 mg/kg/s. In children, the clearance of topiramate is increased and the half-life is shorter. Therefore, at the same dose per 1 kg of body weight, plasma concentrations of Topamax in children may be lower. In this regard, it is necessary to select higher doses compared to adults - up to 15 mg/kg/s. It should be emphasized that Topamax is classified in the third group of AEDs in terms of potential teratogenic effects, i.e., it has minimal teratogenicity (LE Leppic, 2001).
Publications by domestic authors note the promise of using the drug in the treatment of children and adults. Foreign doctors have extensive experience in using Topamax in the form of mono- and add-therapy with sufficient monitoring of pediatric and adult patients. Also, double-blind studies were conducted abroad to compare the effectiveness of Topamax, carbamazepine and valproate (Privitera M. et al., 2003; etc.).
The purpose of this study was to evaluate the effectiveness and safety of Topamax in children and adults as initial therapy, mono- and polytherapy.
An open randomized study included 199 patients (100 men and 99 women) aged 2 to 50 years who received Topamax for 6–36 months (Table 1). All patients were subjected to dynamic clinical observation, EEG, MRI (in several cases CT), and, if necessary, polygraphic sleep recording was performed.
| Table 1. Distribution of patients by age |
In the majority of patients, the disease debuted in childhood - 66.7% (Table 2).
When analyzing risk factors, the following data were obtained. Hereditary complications were noted in 15 patients, perinatal pathology - in 79, traumatic brain injury - in 19 patients, neuroinfections - in 12, cerebral dysplasia - in 22, cysts - in 7, brain tumors - in 4, mesial temporal sclerosis - in 4, vascular diseases - in 3, tuberous sclerosis - in 1, others (Sturge-Weber disease, Randu-Osler disease, etc.) - in 6; Risk factors were not identified in 27 patients. The data presented show that perinatal pathology is one of the main risk factors for the occurrence of epilepsy.
| Table 2. Distribution of patients by disease onset |
According to the forms of the disease, patients were distributed as follows: symptomatic/cryptogenic epilepsy - 159 patients, idiopathic: rolandic epilepsy - 3, epilepsy with generalized convulsive seizures - 2, childhood absence epilepsy - 4, juvenile absence epilepsy - 4, juvenile myoclonic epilepsy - 7 patients. It was not possible to classify the form of the disease in 20 people.
Mental disorders of a paroxysmal nature were observed in the analyzed group before taking Topamax in 9 patients, delayed psycho-speech development was diagnosed in 10 children, dysphoria was noted in 18 cases, depression in 16, cognitive impairment was observed in 23 patients, intellectual impairment of varying severity was noted in 15 cases.
The following features were identified in the women included in this study: a connection with the onset of menstruation at the onset of the disease - in 18 patients, catamenial epilepsy was diagnosed in 6. Pregnancy took place in 2, childbirth - in one case (the child is healthy). Hormonal disorders in the form of dysmenorrhea and/or polycystic ovary syndrome were diagnosed in 17 women, 9 of them before taking AEDs and 8 after the start of treatment (7 patients were simultaneously receiving valproate).
The dose of Topamax ranged from 2 to 15 mg per 1 kg of body weight per day. Monotherapy was administered to 48 patients; in 151 cases the drug was used as an additional drug.
In 40 patients (20.1%), the drug was discontinued due to ineffectiveness or negative effects: aggravation of seizures in the form of their frequency and/or severity, the appearance of seizures of another type, the addition of waking seizures to sleep attacks (total 14 cases - 7%) . In 12 cases (6%), the drug was discontinued due to severe side effects such as excitability, lethargy, speech impairment due to the formation of kidney stones, the development of cystitis with hematuria, weight loss of more than 10 kg, as well as unusual disorders: severe insomnia, psycho-emotional disorders (melancholy), skin pigmentation.
133 patients continued to receive Topamax; of these, 54 (40.6%) were used as monotherapy and 79 (59.4%) as polytherapy. In 65 cases (48.9%) remission was achieved, in 22 (16.5%) seizures were stopped by 50% or more.
The study identified the reasons that served as the basis for prolonging the use of Topamax in 46 patients (34.6%), in whom, according to generally accepted criteria, significant improvement (cessation or significant reduction in seizures) was not observed. A positive effect of the drug on other factors was established, namely: elimination of secondary generalization of seizures or the transition of complex partial seizures into simple ones (17 patients), easier recovery from a seizure (10 people), or a combination of several factors (19 patients).
Side effects that were transient in nature were observed in 36 patients (27%) in the form of excitability (11 patients), retardation, slow speech (6 patients), loss of body weight by 3–10 kg (17 patients), parasthesia (2 patients) . They stopped on their own or when the dose of Topamax was adjusted.
Topamax is an AED with different mechanisms of action: like carbamazepines, it affects sodium channels, like valproates, it affects calcium channels, like benzodiazepines and valproates, it has a GABAergic effect, like acetazolamide it inhibits carbonic anhydrase; Its antiglutamate effect cannot be ruled out either. Thanks to these mechanisms, the drug has a broad-spectrum antiepileptic effect. It is no coincidence that the greatest attention at the last European (Vienna, 2004) and international (Paris, 2005) congresses on the treatment of epilepsy was focused on Topamax along with oxcarbazepine and levetiracetam. There is already significant experience in using Topamax in Russia. According to our data, Topamax treatment is carried out in at least 600 patients. A large number of studies concern childhood epilepsy. In our observation, 25% of patients were pre-pubertal, and the onset of the disease at this age was noted in 75% of patients. And although we do not have experience with the use of Topamax in children of a younger age group, there are reports in the literature of the successful use of Topamax from the age of four months (A. Grinspan et al., 2005).
The effect of Topamax, defined in the literature by the number of respondents responding to therapy with a cessation or reduction of seizures by more than 50%, is assessed differently. For example, according to a study by M. Bujand et al (2004), complete cessation of seizures was noted in 39%, and according to J. Kruja et al (2004) - in only 4.3%, YH Yi et al (2005) - in 22.2%. At the same time, the number of patients whose number of seizures was reduced by more than 50% was 56–58%. In general, such a high percentage of positive results does not correspond to modern data, according to which, despite the introduction of new AEDs, the number of pharmacoresistant patients is at least 1/4 - 1/3 of observations (W. Loscher, D. Schmidt, 2002; D. Schmidt, W Loscher, 2004). Such a discrepancy requires special analysis and most likely requires long-term prospective observation for an objective assessment. As for the spread of the data presented, the result may depend on whether Topamax was used for resistant forms as the first drug or as an additional drug. However, even in the latter case, the result (complete cessation of seizures) ranges from 4.3% (J. Kruja et al., 2004) to 39% (M. Bujand et al., 2004). Only long-term prospective observations can be of value, since the effectiveness of the drug often decreases over time. But information about the duration of prospective observation is not always provided. There may be influence of other factors or their combinations. Thus, according to some data, Topamax, used as the first drug in the elderly, caused the cessation of seizures in 77.3% of patients; no improvement was recorded in only 9.1% of cases (Y. Chinvarun et al., 2005).
The results of our observations confirm the effectiveness of Topamax in the treatment of epilepsy. At least this is obvious for symptomatic/cryptogenic epilepsy, since this particular group of patients was quite representative - 159 people. Noteworthy is the fact that the effectiveness of Topamax was high both in mono- and polytherapy (40.6% and 59.4%, respectively), especially since Topamax was not the first choice drug in all cases. Thus, in 12 patients, it replaced previously prescribed valproate due to planned pregnancy or the presence of side effects such as dysmenorrhea and polycystic ovary syndrome. Moreover, in 4 patients whose seizures were not completely controlled with valproate, treatment became successful after they were switched to Topamax. S. Rielke and A. Schreinea (2005), who have experience in transferring therapy from valproate to Topamax in 65 patients aged 12 years and older, noted positive results in 73% of patients, including cessation of seizures in 48%.
Recently, due to increased attention to the treatment of epilepsy in women, the importance of the problem of replacing valproates with modern AEDs will apparently increase. One of the difficult methodological problems is assessing the effectiveness of drugs, in particular AEDs. We analyzed data on patients who did not give up Topamax, although the frequency of their attacks did not change. For the first time, the criterion of effectiveness was not considered to be a reduction in the frequency of seizures, but the possibility of simplifying and facilitating recovery from an attack. Thus, Topamax was effective in 43.7% of cases in accordance with generally accepted methods and in 66.8% taking this factor into account.
The effectiveness of AEDs, in particular Topamax, according to the results of this study was 66.8%, in 40.6% as monotherapy and in 59.4% as additive. Topamax can not only reduce the frequency of attacks, but also help ease their course and recover from an attack. In children, a larger dose per 1 kg of body weight is required than in adults. The drug has a high efficacy/tolerability rate in both children and adults.
Literature
- Kalinin V.V. New antiepileptic drug Topamax // Breast cancer. Psychiatry. 2002. No. 10. P. 25–33.
- Karlov V. A., Vlasov P. N., Freydkova N. V. Experience of using topiramate in complex therapy of drug-resistant epilepsy // Journal of Neurology and Psychiatry named after. S. S. Korsakova. 2003. Vol. 7. pp. 21–26.
- Mukhin K. Yu, Glukhova L. Yu., Petrukhin et al. Topamax in monotherapy for epilepsy // Journal of Neurology and Psychiatry named after. S. S. Korsakova. 2004. Issue. 8. pp. 35–40.
- Albsoul-Younes F., Salem H., Ajlouni S., Al-Safi S. Topiramate slow dose titration: improve efficacy and tolerability. Pediatric Neurol. 2004; 31: 349–52.
- Amerio R., Tonon A., Bonettelo P., Garafalo P. et al. Triveneto study group on epilepsies. Efficacy and tolerance of topiramate in 363 drug-resistant epilepsy patients. Epilepsy 2002; 43 (8): 347.
- Bujand M., Lopex Roa M., Tresierra F. et al. Topiramate as first ad-on option in refractory epilepsy. Epilepsy 2004; 45 (3): 148.
- Carpay JA, Guerrini R., Lahayl MY, Van Ouen JC Response of localization-relative or generalized epilepsy in monotherapy in non clinical setting. Epilepsy. 2004; 45 (3): 149.
- Chinvarun Y. Long-term, open-label study of topiramate as monotherapy in the treatment of adult patients with recently diagnosed partial onsed seizures. Epilepsy. 2005; 46 (8): 339.
- Grinspan A., Micaeloff Y., Rey E. et al. Topiramate (TPM): efficacy, tolerability and pharmacokinetics in children with epilepsy aged from 6 months to 4 years. Epilepsy. 2005; 46(6):238.
- Kruja J., Qukaj A., Davidhi A. et al. TPM in drug resistant epilepsy. Epilepsy. 2004; 45(3): 148.
- Leppik LE Issues in the treatment of epilepsy. Epilepsy 2001; 42 (4): 1–6.
- Loscher W., Schmidt D. New horizon in the development of antiepileptic drugs: search for new targets conference review. Epilepsy Res. 2002; 50:3–16.
- Marquez-Sanchez J., Marquez-Daniel F. Topiramate in refractory epilepsy: seizure control and assessment of side effects in 108 patients. Epilepsy. 2002; 43 (8): 349.
- Ormrod D., McClellan K. Topiramate: a review of its use in childhood epilepsy. Paediatr Drugs. 2001; 3:293–319.
- Privitera M., Brodie M., Mattson R. et al. EPMN Study Group. Topiramate, carbamazepine and valproate monotherapy: double-blind comparison in newly diagnosed epilepsy. Acta Neurol Scand. 2003; 107:165–75.
- Rielke S., Schreiner A. Efficacy and tolerance of topiramate in epilepsy after transition from valproat. Epilepsy. 2005; 46 (8): 183–184.
- Schmidt D., Loscher W. Drug resistance in epilepsy. Epilepsy Res. 2005; 46:858–870.
- Yi YH, Yang SQ, Liao WP et al. An open-label self—controlled study of topiramate as ad-on therapy with lower dose for treatment of refractory epilepsy. Epilepsy. 2005; 46(3):275–276.
V. A. Karlov , Doctor of Medical Sciences, Professor, Corresponding Member of the Russian Academy of Medical Sciences N. V. Freidkova MGMSU, Children's City Morozov Clinical Hospital, Moscow