Hemorrhagic stroke (HI) is a clinical syndrome in which there is a sharp development of focal and/or cerebral neurological symptoms due to spontaneous hemorrhage into the substance of the brain or into intrathecal areas. The pathological process is triggered by factors of non-traumatic genesis. This type of hemorrhage has the highest disabling ability and is associated with the highest risk of early death.
Causes and mechanism of development of hemorrhagic stroke
The factors that cause rupture of the vascular wall and hemorrhage may be primary and secondary diseases of the cerebral arteries. Primary diseases initially develop in one or more vessels of the brain; they are not a consequence of any other diseases and often represent congenital changes. Secondary pathologies of the cerebral arteries appear against the background of other diseases, such as diabetes mellitus or systemic lupus erythematosus.
The most common primary factors may be:
- aneurysmal dilatation - an area where, due to the weakness of the vascular wall or the consequences of an injury, the artery becomes wider and adapts less well to increased blood pressure or other changes in vascular tone;
- vascular malformation is a congenital disorder of the structure of a vessel, which is manifested by the formation of “vascular glomeruli” with cavities of various sizes;
- other congenital anomalies of the arterial vessels of the brain.
Secondary causes that can lead to changes in cerebral vessels and their rupture include:
- arterial hypertension, especially difficult to treat;
- atherosclerotic damage to the vascular wall;
- vasculitis - inflammatory changes in the wall of blood vessels;
- thrombosis of intracranial veins, which lead to hemorrhage;
- diseases manifested by pathology of the coagulation system (blood and liver diseases);
- uncontrolled use of drugs that affect blood clotting (anticoagulants, antiplatelet agents, fibrinolytics);
- pronounced metabolic disorders that develop during long-term severe illnesses.
The most common cause of hemorrhagic stroke in elderly patients is arterial hypertension - this is about 80% of “vascular accidents”. The second place is occupied by atherosclerosis.
In age groups under 40 years, congenital local dilations of blood vessels (aneurysms) and malformations predominate among the causes of hemorrhagic stroke.
Due to the differences in the causes of the disease in different age groups, early and most accurate diagnosis of the pathology comes first. On our website you can find comprehensive information about methods for identifying risk factors for stroke, as well as find out in which centers they are carried out.
Statistics facts from reliable sources
In the general structure of all types of strokes, hemorrhagic strokes account for 10%-15%. The frequency of its spread among the world population is about 20 cases per 100 thousand people. Experts, based on annual dynamics, report that in about 50 years all these indicators will double. Specifically in the Russian Federation, about 43,000-44,000 cases of HI are diagnosed annually. What is noteworthy is that it occurs approximately 1.5 times more often in men, but the mortality rate from its consequences predominates in women.
According to clinical observations, with this diagnosis, death occurs in 75% of people who are on mechanical ventilation, and in 25% of people who do not need it. Consolidated studies have shown that on average 30%-50% of patients die within 1 month from the moment of an attack of hemorrhage, and 1/2 of them die within the first 2 days. Disability (due to paralysis of the face and limbs, aphasia, blindness, etc.) among surviving patients reaches 75%, of which 10% remain bedridden. And only 25% of patients are independent in everyday life after 6 months.
Pathology represents a huge social problem, since the epidemiological peak occurs in working years - 40-60 years. Hemorrhagic strokes have become significantly “younger”; today they are quite common even among the youth group of people (20-30 years old). The risk category definitely includes people suffering from arterial hypertension, since in most cases this kind of hemorrhage occurs precisely because of chronically elevated blood pressure.
The primary factor that influences the prognosis of outcome is the promptness of providing adequate medical care to the patient.
Types of intracranial hemorrhages
Depending on the location of the vessel from which the blood leaked, this type of stroke is divided into:
- parenchymal hemorrhage, characterized by the formation of a hematoma inside the brain or hemorrhagic impregnation of the nervous tissue;
- subarachnoid, which occurs when blood accumulates between the arachnoid and pia mater of the brain.
With parenchymal hemorrhage, depending on the caliber and location of the vessel, blood may break through into the ventricles of the brain. Such strokes are often characterized by an extremely severe course and loss of a relatively large amount of blood.
Classification
It should be noted that a brainstem stroke results in almost instantaneous death. Only in rare cases is it possible to save the patient’s life with such a diagnosis. At the same time, there is no likelihood of returning to a full life.
The brain stem is the center of all body systems and is directly connected to the spinal cord. It serves as a link between the commands of the brain centers and the nerves of the body: it is thanks to it that we are able to move, breathe, swallow, see, hear, and so on. The brain stem also regulates the circulatory system, thermoregulation, and heartbeat. That is why damage to it during a stroke most often leads to death.
Based on their origin, primary and secondary hemorrhagic stroke are distinguished:
| Primary | provoked by a hypertensive crisis or thinning of the walls of arteries and veins due to prolonged stress on them (for example, due to high blood pressure, physical and nervous overload, etc.) |
| Secondary | provoked by the rupture of an aneurysm, hemangioma and other vascular deformations and anomalies (malformations), congenital or formed in the process of life. |
Depending on the localization zone, I distinguish the following types of hemorrhagic stroke:
- Subarachnoid - hemorrhage into the space between the hard, soft and arachnoid membranes of the brain;
- Hemorrhage on the periphery of the brain or in the thickness of its tissue;
- Venticular hemorrhage - localized in the lateral ventricles;
- Combined type: occurs with extensive hemorrhage affecting several areas of the brain.
Peripheral hemorrhage is much less dangerous than intracerebral hemorrhage, which inevitably provokes the formation of hematomas, edema and subsequent death of brain tissue. Hematomas are also distinguished by location:
- Lobar - the hematoma is localized within one lobe of the brain, without going beyond the cerebral cortex.
- Medial - hemorrhage damages the thalamus.
- Lateral – damage to the subcortical nuclei localized in the white matter of the hemispheres (fence, amygdala, caudate, lenticular nuclei).
- Mixed - hematomas affecting several areas of the brain at once are most common.
What happens during a stroke
Regardless of the cause of hemorrhagic stroke, the mechanism of damage to brain cells is the same. The pathological effect has several directions:
- Impaired tissue nutrition - due to the fact that the brain receives blood from several main vessels, this effect is partially compensated.
- Mechanical damage due to the fact that blood leaves the vessel under pressure and “pushes” the tissues apart.
In the case of parenchymal damage and hematoma formation, the second pathway is more pronounced, resulting in a disruption of communication between brain cells. Hemorrhagic permeation is a relatively uniform distribution of blood between the tissue structures of the brain, therefore the clinical course of such hemorrhage is more favorable.
In subarachnoid hemorrhage (SAH), there is a space where blood gets trapped. For this reason, mechanical damage is less than during the formation of a hematoma, but blood loss and malnutrition of brain tissue can be pronounced.
Cerebral hemorrhage (no matter how mild it may initially seem) is a condition that requires urgent diagnostic and therapeutic measures. Prescribing the correct treatment is possible only after neuroimaging, that is, magnetic resonance or computed tomography.
On our website you can get reliable information about the current discounts and promotions at various diagnostic centers for brain research this month. And also find out where it is possible to conduct an inspection at night, if necessary.
What it is?
Hemorrhagic stroke is an acute hemorrhage in the brain due to rupture or increased permeability of blood vessels. This cerebrovascular accident differs from classic (ischemic) stroke, which is more common (70% of patients).
The nature of changes in blood vessels during an ischemic stroke is the blockage of their lumen by blood clots, resulting in gradual necrosis of brain cells, and in a hemorrhagic stroke there is a violation of the integrity of the vascular wall, as a result of which the brain tissue is saturated and compressed by the gushing blood.
Hemorrhagic cerebral stroke is a dangerous and insidious disease. It is characterized by:
- High mortality (60–70% of patients die within the first week after the onset of the disease).
- Suddenness (in 60–65% of patients, hemorrhage occurs without any previous symptoms).
- Profound disability of surviving patients - 70–80% of people are bedridden and cannot care for themselves, the remaining 20–30% have a less pronounced neurological deficit (the function of the limbs, walking, speech, vision, intelligence, etc. is impaired)
More than 80% of brain hemorrhages are associated with increased blood pressure (hypertension). By taking antihypertensive drugs (blood-lowering drugs), you can reduce the risk of stroke, the amount of hemorrhage and the severity of brain damage. If patients are admitted to a medical facility within the first 3 hours, this increases the chances of survival. Specialized rehabilitation centers help restore lost brain functions as much as possible after a stroke. Complete cure is rare, but possible.
Manifestations of hemorrhagic stroke
Symptoms and signs of hemorrhagic stroke are very diverse, they depend on:
- process localization;
- prevalence of the lesion;
- volume and duration of blood loss;
- the degree of swelling of brain tissue and increased intracranial pressure.
The shorter the period from the onset of the disease to the provision of qualified care to the patient, the fewer complications and the better the prognosis. In order not to waste time, you need to know the general signs of a stroke:
- sudden weakness in the arm/leg;
- numbness of half the face, arms/legs on one side;
- new facial asymmetry;
- speech disorder;
- a sharp decrease in vision in one eye or blindness;
- causeless loss of consciousness, especially in combination with previous symptoms.
If any of the symptoms occur against the background of complete well-being, it is necessary to carry out an accurate diagnosis as soon as possible in a specialized medical institution.
All available information about the nearest medical centers where urgent computer or magnetic resonance imaging of the brain can be performed can be obtained by calling 8 (812) 317-00-37.
Different types of hemorrhagic stroke may occur in different ways, but they also have common features. The disease is often characterized by:
- abrupt onset;
- rapid deterioration of the condition;
- loss of consciousness;
- development in the afternoon, at the peak of physical or emotional stress.
Taking into account the peculiarities of the course of the disease, the most important factor for a successful outcome is time. This means that you should not wait for the condition to improve; you should urgently seek qualified medical help.
It is possible to carry out a timely and accurate diagnosis of this disease by dialing a phone number. Our employees will help you quickly select a medical center that meets your needs: the nearest location, the qualifications of specialists, the quality of diagnostic equipment, the cost of the study and the availability of current promotions.
Left-hand side
If the left side is affected, the consequences are characterized by disruption of the right side of the body. The patient experiences complete or partial paralysis, and not only the leg and arm are affected, but also half of the tongue and larynx. Such patients develop gait disturbances and a characteristic posture of the right hand (folded in a boat).
The victim experiences deterioration in memory and speech, and the ability to clearly express thoughts is impaired. Damage to the left hemisphere of the brain is characterized by problems with recognizing time sequences; it cannot decompose complex elements into components. Impairments in written and oral speech appear.
General cerebral symptoms
General cerebral symptoms include:
- Headache of great intensity, which occurs suddenly and is accompanied by dizziness. Some patients describe it as “a blow to the head.” It does not stop on its own and is not relieved by painkillers. Often SAH is accompanied only by this symptom.
- Vomiting without previous nausea, caused by cerebral edema and increased intracranial pressure.
- Loss of consciousness followed by the development of a coma. This symptom may be the only manifestation of a hemorrhagic stroke. It is important that there is a person with the patient who saw what happened.
- Stunnedness, causeless drowsiness. However, often at the initial stage of development of hemorrhagic stroke there is increased emotional and motor excitability, which is then replaced by inhibition.
- Signs of dysfunction of the autonomic nervous system: cold sweat, feeling hot, dry mouth.
- An increase in body temperature to high values can be observed in severe cases.
Precursor symptoms
The preceding signs or so-called aura do not always develop. This is rather an exception to the rule, since in most cases the opposite is observed.
Hemorrhage occurs suddenly. If we talk about manifestations that will indicate the approach of an emergency condition, they can be as follows:
- Intense heat in the chest, flushing of the face. A sudden sensation that comes out of the blue. As a rule, there are no objective reasons.
- Numbness of half the face. In addition, tingling may occur. Paresthesias indicate sudden, acute ischemia. This is a very alarming sign, even if nothing followed after it. You need to pay close attention to such “calls” and urgently run to the doctor.
- Problems with speech perception. The native language that a person has spoken for many years suddenly turns out to be incomprehensible. This is the first sign of a malnutrition of the temporal lobes of the brain, into which blood may bleed.
- Problems with coordination of movements. Acute dizziness. May result in a fall and injury.
Attention:
Aura or precursors of a pathological process occur in only 5-10% of the total number of cases. Much more often, the disorder debuts directly from the main clinic.
All possible symptoms of pre-stroke in women are described in detail here.
Focal symptoms
Focal manifestations are a group of symptoms characterized by a number of specific neurological signs that occur depending on the location of the lesion.
The most common focal manifestations are:
- weakness in the arm/leg/half of the body, up to paralysis;
- violation of the movement of facial muscles, due to which the eyelid does not rise, the corner of the mouth drops and the cheek “sails” when exhaling;
- impaired skin sensitivity;
- pathology of speech, vision, hearing;
- exotropia;
- swallowing disorder;
- spatial disorientation of varying severity - staggering, tilting and turning to the side when walking, inability to assume a vertical body position.
Sometimes, based on characteristic focal manifestations, the localization of the pathology can be assumed:
- When the lesion is located in the frontal lobe, characteristic symptoms may be a forced rotation of the patient’s head and eyes in the direction of the hemorrhage. The so-called “frontal psyche” often develops, which manifests itself in an inadequate assessment of the state of health and a decrease in criticism of one’s actions.
- The localization of the hematoma in the temporal lobe may be indicated by early epileptic seizures.
- Hematomas of the parieto-occipital localization can sometimes have scant symptoms and are detected by chance during CT or MRI of the brain, which indicates the importance of neuroimaging methods.
- Hemorrhagic stroke in the brainstem often manifests as breathing and heartbeat disturbances.
- Damage to the cerebellum is characterized by loss of consciousness, vomiting, severe dizziness and loss of coordination.
It should be noted that these clinical manifestations can be seen with small hematomas. With its significant size, cerebral edema rapidly increases and the patient’s condition becomes so severe that it becomes impossible to determine focal symptoms.
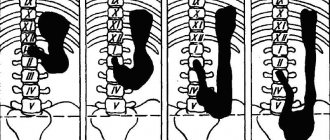
Typical location of hemorrhages
Most often, and this is about 55% of cases, hemorrhages occur in the putamental zone. Putamental bleeding occurs due to rupture of degenerated lenticulostriate arteries, which causes blood to enter the brain shell. The culprit of pathogenesis with such localization is usually long-standing hypertension. In some cases, bleeding from the putamentum breaks into the ventricular system, which is fraught with tamponade of the gastrointestinal tract and acute occlusive-hydrocephalic crisis.
The next most common location is the subcortical region (subcortical). Subcortical GIs are observed in 17%-18% of cases. As a rule, the leading sources of such hemorrhage are ruptured AVMs and aneurysms against the background of increased pressure. The subcortical zones involved in the hemorrhagic process are the frontal, parietal, occipital or temporal lobe.
The third most common place, where brain hemorrhage is determined in 14%-15% of cases, is the optic thalamus, or thalamus. Thalamic hemorrhages occur due to the release of blood from the blood vessel of the vertebrobasilar region. Pathogenesis can be associated with any etiological factor, however, as always, the involvement of hypertensive syndrome is significantly more often noted.
In fourth place (7%) in terms of frequency of development are pontine GIs. They are concentrated in the back of the brain stem, that is, in the pons. Through the bridge, the cortex communicates with the cerebellum, spinal cord and other major elements of the central nervous system. This department includes the centers for controlling breathing and heartbeat. Therefore, the bridge is the most dangerous localization of hemorrhage, practically incomparable to life.
Meningeal symptoms
Signs of irritation of the meninges can occur with parenchymal hemorrhage due to cerebral edema, but they are more characteristic of subarachnoid hemorrhage.
The most typical sign is a stiff neck, when the patient is unable to press the chin to the chest when lying down.
If the patient bends his knees while checking for rigidity, this is another sign of irritation of the meninges, which is called Brudzinski's sign.
Stroke hemorrhagic right side
This type of stroke has a number of characteristic signs. The clinical picture characteristic of a right-sided stroke is formed from the following symptoms:
- Persistent motor disturbances on the side opposite to the lesion. Hemiparesis of the left upper and lower limbs is formed.
- Violation of all types of sensitivity of the skin (tactile, muscle-articular, pain, temperature and others).
- Muscle spasm with the formation of contractures or lack of muscle tone.
- Complex of meningeal symptoms: Brudzinski, Kernig, oculofacial phenomenon and
other.
Complications of hemorrhagic stroke
The most common complication of non-traumatic hemorrhage is epileptic seizures. They are divided into early, which arose in the first week after a stroke, and late, which developed 7 days after a cerebrovascular accident.
To a serious life-threatening illness, the human body responds with a systemic inflammatory response - an increase in body temperature, changes in blood tests. Such a complication may indicate a deterioration in the patient’s condition. Then the doctor assumes an increase in the source of hemorrhage or the addition of an infection.
The consequence of maintaining a recumbent position may be the development of deep vein thrombosis of the legs, which will entail the development of other, no less dangerous, diseases.
Complications also include cardiac decompensation, which can manifest itself in the development of various arrhythmias, cardiomyopathies, and congestive pneumonia.
Due to damage to brain tissue, memory and mental performance may be impaired.
Diagnostics
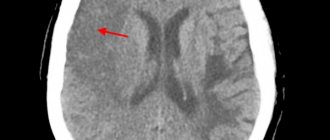
To accurately identify the disease and differentiate hemorrhage from ischemia, an instrumental examination is performed:
- MRI or CT scan - the images show a limited area of the hematoma. The safety of magnetic tomography allows for multiple examinations and monitoring of neuronal recovery.
- Angiography - shows the condition of blood vessels. Well displays arterial rupture, signs of atherosclerosis and congenital anomalies.
- Lumbar puncture - taking cerebrospinal fluid in the lumbar region for analysis. The diagnosis of hemorrhagic stroke is made when red blood cells are detected in the cerebrospinal fluid in high concentrations.
Diagnosis of hemorrhagic stroke
In order for a person without medical education to be able to promptly suspect the initial signs of a stroke in a relative or friend, special recommendations have been developed.
The “Face-Hand-Speech” test involves detecting the most typical signs of pathology:
- Detection of facial asymmetry.
- The patient needs to extend both arms in front of him. If one of them involuntarily descends, then there is a possibility of a vascular accident.
- The patient is asked to give his full name, address, time of year to determine speech impairment and the person’s orientation in space and time.
There are simplified versions of the tests, for example, UZP - smile, speak and raise your hands. If there are noticeable deviations in these actions, emergency measures should be taken to transport the patient to the hospital, that is, call an ambulance.
Before providing effective treatment, the doctor must answer two questions:
- Is there a stroke?
- If yes, what type of stroke developed?
Determining the nature of brain damage is only possible using CT or MRI - without these highly accurate research methods, the diagnosis of stroke is incomplete.
There are signs that are more likely to indicate the occurrence of a hemorrhagic stroke:
- The patient was previously diagnosed with arterial hypertension. In this case, the medications did not have the desired effect or the person did not take them.
- Deterioration of the condition is associated with a peak in physical activity or emotional stress.
- A sharp and significant deterioration in health with pronounced cerebral and focal symptoms.
For subarachnoid hemorrhage, slightly different signs have been identified, including:
- Young age of patients.
- Often the primary symptom is a severe headache.
- Insignificant severity of focal symptoms.
Often an important distinguishing feature of hemorrhagic stroke from ischemic stroke is the increase in impairment of consciousness with unchanged motor and sensory pathology. This may be a sign of an enlarged hematoma.
Differential diagnosis is vital because treatment for different types of stroke can vary dramatically.
Symptoms of hemorrhagic stroke
Subarachnoid hemorrhage is accompanied by severe headache, vomiting, convulsions may begin, consciousness is impaired, Terson syndrome is observed, and meningeal symptoms appear. Parenchymal stroke is characterized by unexpectedly occurring severe headache, pallor or redness of the face, asymmetry of facial features, impaired coordination of movement, impaired respiratory function, and agitation. Ventricular stroke, the most severe form of the disease, is characterized by rapid deterioration of the patient's condition; bloody vomiting, loss of consciousness, fever, convulsions, and coma may occur. Ventricular stroke most often leads to the death of the patient. In most cases, hemorrhagic stroke occurs during the daytime, and the patient suddenly loses consciousness.
At the first examination, doctors note a change in complexion, high blood pressure, impaired respiratory function, slow pulse, decreased muscle tone, and tendon reflexes. Such symptoms are characteristic of the first hours after a stroke, then an increase in muscle tone and tendon reflexes occurs, the function of the pelvic organs is disrupted, the condition worsens, and the patient may fall into a coma.
Make an appointment
Instrumental diagnostics
Computed tomography is the gold standard for detecting cerebral hemorrhage. This study is distinguished by its accessibility, information content and short scanning time.
A CT scan performed in the first hours of the disease will help the doctor establish an accurate diagnosis and prescribe the correct treatment.
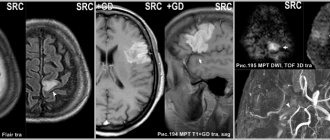
If the cause of the vessel damage is a malformation, then to identify it using CT, it is necessary to administer a contrast agent. Magnetic resonance scanning without any problems will allow you to localize pathologically altered vessels without paramagnetic enhancement.
MRI is more sensitive to small foci of hemorrhage and helps to more accurately determine the stage of the process. However, in order to clarify the hemorrhagic nature of the stroke, an MRI scan should be done 24 hours after the onset of the disease. Even many years after a vascular accident, an MRI of the brain will reveal pathology.
Since MRI shows the structures of the brain in more detail, this type of tomography is preferable to determine the root cause of a hemorrhagic stroke.
Each method has its own advantages and disadvantages, so before using them, it is recommended to examine a specialist - a neurologist.
Since the patient’s further well-being depends on the time of initiation of treatment, the primary diagnosis is carried out using computed tomography. Later, after starting the necessary therapy or surgical treatment, an MRI will help clarify the cause of the stroke.
Right side
If the right side is affected, the most dangerous consequence is damage to the brain stem, in which a person's chances of survival are close to zero. This department is responsible for the functioning of the heart and respiratory system.
Diagnosing a hemorrhagic stroke on the right is quite difficult, since the centers of orientation in space and sensitivity are located in this part. This lesion is determined by speech impairment in right-handed people (in left-handed people the speech center is located in the left hemisphere). In addition, there is a clear relationship: if the functionality of the right half of the brain is impaired, the left side suffers and vice versa.
Treatment of hemorrhagic stroke
After identifying signs of a stroke, relatives or friends need to provide emergency assistance to the victim, which consists of:
- positioning the person on the right side (especially when vomiting) to prevent stomach contents from entering the respiratory tract;
- raising the upper half of the body by approximately 30 degrees;
- measuring blood pressure and helping to take medication for high blood pressure (in this case, you should not give medications that need to be washed down with water, because a stroke may be accompanied by a swallowing disorder);
- organizing optimal air access, that is, loosening the collar, tie, belt and freeing from restrictive clothing.
Upon arrival of the ambulance team, any information about the disease will help in correct diagnosis. To do this, you need to tell doctors about:
- time of onset of the disease;
- the nature of the development of the pathology: the condition worsened sharply or gradually;
- the symptoms with which the disease began;
- signs of a stroke that occurred later;
- chronic diseases (especially those that could be the cause of the development of a vascular accident);
- constant use of medications;
- blood pressure numbers (if it was measured).
The medical professional should tell everything that happened to the victim.
Causes
Development factors have already been named earlier; it is worth specifying the described mechanisms and identifying the exact provocateurs. Among them:
Hypertension
Stable increase in blood pressure. It is considered an independent cardiovascular disease. It occurs frequently, especially in patients of the older age group. Almost in 90% of cases, albeit to varying degrees of severity.
The higher the blood pressure level, the more serious the risks. Since the vessels are in a state of constant increased load, they wear out faster. At a certain point, they simply cannot stand it and burst. Which leads to an emergency.
The cause of cerebral hemorrhage is an excessive impact on the internal lining of the artery, its muscle layer, dystrophy and, as the final result, a sharp rupture and leakage of liquid connective tissue.
Diabetes
An endocrine disease that stands apart. It is characterized by a stable, regular increase in blood sugar levels.
In addition, the pathology poses a danger to all tissues of the body. First of all, it is the blood vessels that suffer. A pathological narrowing of the lumen of the arteries develops. The tissues do not receive enough nutrition.
In addition, the phenomena of degeneration of the internal lining and muscle layer are increasing. The result is the same as in the previous case.
The disease cannot be treated as such, so the likelihood of encountering a hemorrhagic stroke is enormous and is growing every year.
By the way, this is one of the main factors in the death of patients with diabetes.
Smoking
Subjective reason. The problem is not only and not so much with nicotine, but with other toxic substances. The quality of vessels is affected by cadmium, arsenic vapors, sulfur structures, carbon compounds and other chemicals.
If you smoke regularly, the likelihood of a stroke increases. Because the vessels quickly wear out and narrow.
Alcohol consumption
About the same thing happens, only the poisons are different. When ethanol is processed, acetaldehyde and acetic acid are produced. They are dangerous for the heart and arteries. Which becomes the culprit that provokes hemorrhage.
Drug use
According to research, patients who love cocaine and synthetic stimulants are especially at risk.
The cause of intracerebral hemorrhage is thinning of the walls of blood vessels, increased pressure, and degeneration of the arteries. The result is obvious.
Arrhythmias
Oddly enough, the very nature of cardiac output determines the condition of the blood vessels. It turns out that the load on the arteries is distributed unevenly. Sometimes she is high, sometimes she is low. The pressure rises and falls.
In such an emergency mode, the body works constantly. This can't end well. The result of arrhythmias is cerebral hemorrhage. Provided that rhythm disturbances are not corrected in a timely manner.
Read more about the types of arrhythmias, possible risks and treatment here.
Atherosclerosis
Deposition of fatty compounds on the walls of blood vessels. Cholesterol plaques interfere with blood flow. The result is increased pressure as local resistance has to be overcome.
Gradually, the artery wears out, a wall protrusion of the vessel (aneurysm) is possible, then the likelihood of hemorrhage increases significantly. It makes sense to treat the disease at the earliest stage, while the chances of recovery are high enough.
Vascular defects
Congenital or acquired disorders. For example, too narrow a lumen or degeneration of the walls. Various options are possible. The bottom line is that they potentially increase the likelihood of a stroke.
If such a change is detected, you need to adhere to the rules of prevention: do not overexert yourself physically, eat right, etc. The treating specialist helps develop the strategy.
Heart defects
Also congenital or acquired. Most often, anatomical changes in the condition of the valves occur.
There are more dangerous variants of the pathological process, complex ones. Read more about the types of heart defects here.
Treatment is carried out by cardiology specialists and specialized surgeons.
Obesity
Increased body weight is associated with two disorders: increased blood pressure (hypertension) and changes in the nature of lipid metabolism (atherosclerosis).
Anemia
Basically, rare forms of the pathological process. The disorder is caused very rarely, in no more than 0.5% of cases.
Wrong lifestyle
A diet high in fat, carbohydrates, also sitting in one place, lack of mobility (so-called physical inactivity). They increase the risk, but do not themselves cause cerebral hemorrhage.
Hormonal imbalances
An increase in the concentration of substances in the adrenal cortex, pituitary gland or thyroid gland.
Use of certain drugs
To increase blood flow, oral contraceptives, and other medications.
These reasons need to be eliminated as quickly as possible. In the early stages, it is still possible to prevent the irreparable.
General principles of treatment
After admission to the hospital, the neurologist assesses the severity of the condition, and then determines whether the patient needs to be operated on or whether it is better to treat him conservatively.
Many doctors agree that the most dangerous are the 3rd day after a vascular accident, and stabilization of the condition occurs on days 5-7-14, depending on the severity of the pathology.
Regardless of the type of stroke, treatment begins with:
- Bed rest.
- Elimination of any physical stress. For this purpose, laxatives and other symptomatic drugs may be prescribed, for example, antitussives for severe dry cough.
- Organization of patient care for the prevention of infectious complications and bedsores.
- Adequate nutrition depending on the level of consciousness: if the patient can swallow on his own, he eats gentle food through the mouth, if he cannot, through a tube.
- Prescription of drugs that regulate blood clotting. This is necessary to stop bleeding or prevent its recurrence.
- The use of neuroprotectors - medications that reduce the “suffering” of brain cells from oxygen starvation.
Medicines are prescribed only when they are necessary and not contraindicated.
Treatment tactics
The treatment regimen is selected individually, depending on the examination results, the general condition of the patient and other factors, including age and concomitant diseases. The Clinical Brain Institute is a staff of professionals who will help you choose the right treatment regimen and will accompany the patient at all stages of treatment and rehabilitation. In case of stroke, conservative methods or surgical intervention may be recommended.
Conservative methods
In the acute period of hemorrhagic stroke, it is important to regulate blood pressure, as well as restore the level of blood circulation in the nerve tissues. This process is controlled by the systemic use of drugs from different groups:
- hypothetical agents for lowering blood pressure levels;
- potassium antagonists;
- antispasmodics and painkillers;
- sedatives;
- hemostatic drugs;
- antiprotease and antifibrinolytic groups;
- vitamin complexes;
- diuretics to prevent brain swelling;
- blood plasma substitutes.
Drug therapy is possible only if the size of the hematoma does not interfere with the normal functioning of the brain. As soon as the patient's condition becomes stable, measures can begin to restore lost skills. If with ischemic strokes this possibility appears within a few days after the attack, then after a hemorrhage in the brain the process takes longer.
Surgical treatment of hemorrhagic stroke
Surgery is performed to remove large hematomas that are preventing normal recovery. The operation is complex, so it is prescribed only in cases where conservative methods do not bring results. Thus, the size of a hematoma of 30 ml or more is considered critical - such a volume does not resolve on its own. Surgery is also recommended for hemorrhages in the cerebellar area, which are manifested by severe neurological symptoms. There are two methods of performing the operation: with access using classical and endoscopic methods.
Experts from the Clinical Brain Institute advise you to accept the decision voiced by your attending physician. If full treatment and rehabilitation are impossible without surgery, it is better to carry it out using endoscopy. However, there are also contraindications to surgery. These include medial hematomas and the patient being in a state of deep coma - in both cases, the risk of death during surgery is up to 100%.
Management of patients with subarachnoid hemorrhage
If the diagnosis of subarachnoid hemorrhage is confirmed, the patient must remain in the hospital for at least a month. Treatment consists of:
- Monitor blood pressure and lower it with medications if necessary.
- Prescriptions of drugs that relieve headaches and agitation.
- Normalization of breathing and metabolic disorders.
- Reduce intracranial pressure by administering osmotic diuretics and elevating the head of the bed for several weeks.
- Carrying out therapeutic measures to prevent complications in the form of spasm of cerebral vessels, that is, the prevention of ischemic disorders.
The danger of SAH lies in the fact that many patients consult a doctor only some time after the onset of the pathology. Therefore, treatment may be less effective.
Clinical picture
At the first symptoms of a hemorrhagic stroke, it is important to begin treatment immediately. This is an acute condition that does not go away without symptoms. In most cases, the patient experiences a sharp deterioration in health, and loss of consciousness may occur.
The first symptoms of hemorrhagic stroke
The first manifestations of a stroke may differ, depending on the volume of the hematoma and its location. The task of loved ones is to identify them at an early stage and call a medical team for urgent hospitalization of the patient. Experts from the Clinical Brain Institute advise you to familiarize yourself with the main symptoms that may indicate acute cerebrovascular accident:
- tingling sensation of the skin, numbness of part of the face;
- nausea and vomiting;
- headaches, as well as soreness in the eye area and behind the eyes;
- impaired motor coordination;
- rapid pulse;
- paresis and paralysis of muscles in any part of the body, most often the process is one-sided.
These symptoms are typical if the patient remains conscious. Fainting is a common sign of a hemorrhagic stroke, and it is strictly forbidden to try to revive the person. There are several phases of consciousness regression - the prognosis for each of them will also be different:
- stunning - minor changes in which the victim is poorly aware of what is happening and practically does not react to others;
- somnolence - lack of response to external factors, while the eyes remain open, breathing and heartbeat are normal;
- stupor - a condition that resembles sleep, with preservation of the swallowing reflex and the reaction of the pupils to light;
- coma is a complete lack of reaction to what is happening; the patient’s vital activity is supported by special equipment.
Various disturbances of consciousness are present in almost all patients, say experts from the Clinical Brain Institute. Based on their condition, it is already possible to preliminarily predict their chances of recovery. Thus, if consciousness is maintained, the probability of death remains within 20%, with stunning - up to 30%, with somnolence - up to 55%, with stupor - up to 85%. With the development of coma, the prognosis is questionable - survival rate is no more than 10%.
Signs of the acute phase of stroke
The clinical picture of stroke includes several main syndromes. They are a consequence of acute cerebrovascular accident and occur when neurons die. These syndromes suggest a hemorrhagic stroke, even if the patient is conscious:
- anisocoria - the patient’s pupils are dilated unevenly and have different sizes;
- decreased severity of reflexes, including a slower reaction of the pupils to bright light;
- the appearance of an oculocephalic reflex - if a patient in a coma turns his head to the side, his pupils shift in the opposite direction;
- bulbar syndrome - decreased tone of the chewing, swallowing muscles and tongue, which is manifested by corresponding symptoms;
- pseudobulbar syndrome - a violation of swallowing, chewing and speech while maintaining the tone of the corresponding muscles.
Immediately after a hemorrhagic stroke, it is difficult to predict the likelihood of full recovery. The patient’s condition can only be determined dynamically, so the patient spends the first time under 24-hour medical supervision. The fact is that during the course of the disease there are often several critical periods during which the likelihood of relapse is increased. The first of them occurs on the second to fourth day after the attack, the next one appears 10-12 days later.
Management of patients with intracerebral hemorrhage
Hemorrhagic stroke is a condition that requires emergency diagnosis, adequate treatment and observation.
To do this you need:
- Conduct constant monitoring of the patient’s condition, especially in the first days after the onset of the disease: monitoring breathing and indicators of the state of the cardiovascular system.
- Monitor blood pressure numbers. They are often not reduced to normal levels, so as not to impair blood supply to the brain and provoke vasospasm.
- Prescription of hypoglycemic drugs - in almost half of patients, blood glucose levels increase.
- Use of antipyretic drugs. An increase in body temperature entails worsening cerebral edema, increased intracranial pressure and can lead to a significant deterioration in the patient’s general condition.
- Carrying out symptomatic therapy and treatment of complications.
Mechanism of formation
The development of the disorder is based on one factor or several pathogenetic factors at once. What exactly can affect the likelihood of a violation:
- Cardiovascular diseases. Represented by a wide group of diagnoses. In the vast majority of cases, hemorrhagic stroke develops as a complication of long-term and untreated hypertension. That is, a stable and pronounced increase in blood pressure.
Statistics show that the mechanism accounts for up to 85% of the total number of hemorrhages. This is the absolute majority. The only way to prevent an emergency condition is to undergo high-quality treatment of the underlying pathology.
- Metabolic disorders. Basically, deviation of lipid movement. That is, a disorder in which the rate of deposition and elimination of fats significantly deviates from the conventional norm.
The pathological process leads to another problem - atherosclerosis. When cholesterol deposits form on the walls of blood vessels, which interfere with blood flow. The result is that the likelihood of hemorrhagic stroke and death from complications increases significantly.
- Hormonal imbalance. We are talking about a variety of disorders: from changes in the quality and intensity of the synthesis of sex substances to problems with the production of insulin and compounds of the adrenal cortex.
- Hereditary causes. The mechanism is associated with a not yet fully understood method of transferring risks from parents to children. The disease itself, of course, is not transmitted.
If a mother, father, grandmother, grandfather has a hemorrhagic stroke, this does not mean that the same thing will happen to a descendant. But the likelihood is growing. Apparently - by several tens of percent. The topic has not been fully studied, research continues.
- Toxic damage to the body. Poisoning by vapors of non-metals, some medications. The risk of hemorrhagic stroke increases with the systematic use of antiplatelet agents, anticoagulants, and hormonal agents.
- Some forms of anemia, blood diseases. Changes in the rheological properties of connective tissue lead to disruption of the speed and quality of trophic systems and an increase in blood pressure. In some cases, vascular permeability increases. The result is an increased risk of cerebral hemorrhage.
Mechanisms exist in isolation or are combined with each other. This question needs to be clarified, since the therapy strategy and its essence depend on the origin of the pathological process.
Rehabilitation after hemorrhagic stroke
Recovery of post-stroke patients is an important stage in improving a person’s quality of life. Carrying out these activities helps eliminate existing movement and sensitivity disorders.
Medical rehabilitation should be:
- individual - developed for a specific patient;
- timely - start as early as possible;
- adequate - depend on the patient’s condition and his capabilities;
- staged - gradual, slow complication of exercises and an increase in the variety of rehabilitation methods;
- long-term;
- comprehensive - for greater efficiency, the maximum possible rehabilitation methods are used to influence the human body from different angles;
- successive - when a patient moves from one medical institution to another, recovery measures must continue each other.
The main criterion for starting rehabilitation measures for hemorrhagic stroke is not only normal hemodynamics (blood pressure, heart rate), but also the reverse development of changes in the brain (for example, signs of a decrease in cerebral edema).
The most important factor influencing the quality of recovery is the active participation of the patient in the rehabilitation process.
The transition to more complex exercises is made only if the condition of the patient’s cardiovascular and respiratory systems is monitored.
Surgery for hemorrhagic stroke
The second stage of the treatment process is neurosurgical intervention. Its goal is to remove the life-threatening hematoma to improve survival and achieve the best possible satisfactory functional outcome. The sooner the operation is performed, the better prognosis can be expected. However, early surgery, as a rule, involves performing surgical procedures no earlier than 7-12 hours after the stroke. In the ultra-early period, it can lead to repeated bleeding.
When it is wiser to begin removing blood clots is decided by highly competent neurosurgeons. It was noted that operations performed even 2-3 weeks (inclusive) after the GI procedure can also lead to a positive effect. So the question of when to operate on a patient is entirely the responsibility of the doctor. Let us consider the fundamental surgical methods widely used for hemorrhagic strokes.
- Open decompressive craniotomy is indicated for medium and large subcortical, as well as large putamental and cerebellar hemorrhages. It is also addressed in case of pronounced displacement and increasing swelling of the cerebral component, deterioration of the patient’s neurological status. Open surgery is performed under complete general anesthesia using microsurgical optics. Removal of the accumulated clot is carried out through classic trepanation access. Next, an economical encephalotomy is performed, then the pathological component is sucked out with a special device. Dense accumulations are removed with fenestrated tweezers. At the end, the surgical field is thoroughly washed with sodium chloride solution, and thorough hemostasis is performed through coagulation and antihemorrhagic agents.
- The puncture-aspiration procedure is recommended for small hemorrhages of the thalamic, putamental, cerebellar location. The method consists of creating a small hole in the skull, puncturing the hematoma, and then freeing the brain from its liquid mass through aspiration. This technology can be implemented using one of two minimally invasive techniques: based on the principle of stereotactic or neuroendoscopic aspiration. Sometimes it is advisable to combine them with local fibrinolysis. Fibrinolysis involves installing drainage after puncture and aspiration into the hematoma cavity. Fibrinolytics are administered through the drainage over several days to activate the dissolution (liquefaction) of the blood clot and the removal of lysed blood elements.
Unfortunately, the functions of the central nervous system cannot be completely restored after hemorrhagic strokes. But in any case, it would be in the patient’s interests to go to a clinic where international-level doctors work in the diagnosis and surgical treatment of intracerebral lesions. This is the only way to ensure adequate and safe surgical support. Consequently, minimizing complications leads to more productive results in restoring quality of life.
We emphasize that the ideal execution of the operation in the right time increases the survival rate by 2-4 times. Proper postoperative care reduces the likelihood of relapse. It must be warned that a repeated stroke with hemorrhage in 99.99% of patients leads to death.
As a recommendation, we consider it important to say that the Czech Republic shows good results in the level of development of the field of brain neurosurgery in Europe. Czech medical centers are famous for their impeccable reputation and excellent rates of successful recovery of even the most difficult patients. And that’s not all: the Czech Republic has the lowest prices for neurosurgical care and one of the best postoperative rehabilitation. The choice of a medical institution for undergoing surgery, of course, remains with the patient and his relatives.
Rehabilitation in the intensive care unit
12-24 hours after a vascular accident, it is already possible to carry out restoration measures. Before they begin, a test is performed to assess independent swallowing, after which the patient’s feeding method is selected.
The following rehabilitation methods are used during the acute period of a stroke:
- Treatment by position. The position of the patient's head/arms/legs should be changed approximately every two to three hours, as well as turned to the side (if the condition allows it). In order to hold a person in a certain position, bolsters or pillows are used.
- Verticalization - giving the patient an upright position. This can happen passively (with the help of a functional bed or table), passive-active and active. However, to carry out this rehabilitation method, it is necessary to ensure the stability of the circulatory system. More often, verticalization begins in the neurological department.
- Breathing exercises can be carried out in various ways depending on the patient’s condition: vibration with the hands while exhaling, in a position that facilitates breathing, contact breathing (stimulation by touching the hands to the chest) and others.
- Therapeutic gymnastics includes assistance in restoring not only the large muscles of the limbs, but also the muscles of the neck and eyes. At the initial stage, passive gymnastics is performed, when flexion/extension of the patient’s fingers, arms and legs is performed by a qualified physical therapy nurse.
Also during this period, physiotherapeutic treatment is actively used: magnetic therapy, magnetic laser therapy, reflexology, electrical stimulation, darsonvalization and other methods.
Types of paralysis on the right side
According to the nature and localization of vascular accidents, the types and subtypes of paralysis are classified:
- Central paralysis. It develops when the areas of the brain and spinal cord responsible for the function of movement and the state of the neuromuscular complex are damaged. Characterized by specific spastic reactions. With the central form of paralysis, all muscles are affected, which are in constant tension, and when calm they show clonus - rhythmic twitching, mainly in the area of the knees and feet. In many areas, diagnostic reflexes are absent or weakened.
- Peripheral paralysis. With this type of stroke, a decrease or absence of neurological reflexes develops. The tone in the muscles is not determined, they atrophy, decrease in mass, patients lose the ability to move, self-care and generally do any activity. The main task is to restore the conduction pathways of impulses from the brain and spinal cord to the neuromuscular system. By the nature of the pathological symptoms and the areas of their location, it is possible to determine which segments of the central nervous system are out of order.
Rehabilitation in the acute period
At this stage (from 24 hours to 3 weeks), maintaining the achieved effect and improving exercise tolerance plays a significant role. For this purpose, methods such as:
- treatment by position;
- massage, which is equivalent to passive gymnastics;
- breathing exercises;
- active verticalization in the absence of contraindications (if necessary, using additional support);
- mechanotherapy;
- training on cyclic simulators.
During this recovery period, active correction of speech disorders is carried out with the involvement of speech therapists.
Consequences
If patients can be saved, they experience neurological deficits—symptoms caused by damage to the area of the brain where the hemorrhage occurred.
These may be consequences of a hemorrhagic stroke:
- paresis and paralysis - impaired movement of the limbs on one half of the body, since they are constantly in a half-bent position and it is impossible to straighten them;
- speech impairment and its complete absence;
- mental disorders and irritability;
- constant headaches;
- movement coordination disorders;
- inability to walk or even sit independently;
- visual impairment up to complete blindness;
- facial distortion;
- vegetative state - the absence of any signs of brain activity (consciousness, memory, speech, movements) with preserved breathing and heartbeat.
Symptoms of the disease and their duration depend on the location of the hemorrhage and its volume. The first 3 days are the most dangerous, since during this time severe disorders occur in the brain. Most deaths (80–90%) occur during this period. The remaining 10–20% of patients die within one to two weeks. Patients who survive recover gradually from a few weeks to 9–10 months.
Rehabilitation in the early recovery period
This stage begins 21 days from the onset of the disease and lasts up to six months.
Early recovery can take place in rehabilitation centers, clinics or at home. Self-execution of exercises is possible only if they are performed correctly and there is no need for constant monitoring of the patient. Therefore, all exercises at home are selected strictly individually.
The period of early rehabilitation should be a continuation of the inpatient recovery phase. Nowadays, more attention is paid to everyday skills: renewing them or teaching possible alternatives. Equally important is assistance in a person’s social adaptation.
Recovery in a rehabilitation center
The most effective assistance in rehabilitation is provided in specialized medical centers. It includes the following methods:
- kinesitherapy – training in walking and everyday skills;
- electrical stimulation of peripheral nerves and muscles;
- physiotherapy and massage;
- classes with a speech therapist-aphasiologist to restore speech;
- use of neurotrophic medications (Cerebrolysin, Piracetam, Semax);
- psychotherapy;
- biofeedback sessions;
- acupuncture;
- occupational therapy.
- Stroke on the left side: consequences and features of recovery. How long do people live with this diagnosis?
If the patient ends up at home, the possibilities for rehabilitation are reduced.
Rehabilitation in the late recovery period
This stage lasts from six months to a year after the stroke, and sometimes longer (with persistent changes). Rehabilitation in the late recovery period involves preparing the patient for the maximum independence that he can achieve.
In addition to physical rehabilitation, work continues on social adaptation and restoration of professional skills or reorientation.
Most experts point to the positive effects of occupational therapy, especially work related to the earth.
During this period, a person may need psychological support, so psychotherapeutic consultations are carried out.
Recovery after a stroke
The rehabilitation period after a hemorrhagic stroke is long, especially in old age. It depends on the lost functions and does not guarantee their complete rehabilitation. Lost abilities are restored most quickly in the first year after a stroke, then this process is slower. The neurological deficit that remains after three years will most likely remain for life.
Neurologists and rehabilitation specialists are ready to help restore lost functions as much as possible. For this:
- classes are held with a psychologist or psychotherapist;
- if reading/writing skills are lost, classes are held to restore them;
- hydrotherapy is carried out (massage in the pool, light exercises in the water);
- classes on special simulators;
- if speech reproduction is impaired, the person will have to work with a speech therapist; for paresis or paralysis, physiotherapy is carried out (for example, on the Myoton apparatus), massage and exercise therapy are performed with an instructor;
- drugs are prescribed that will help restore lost neural connections (“Cerakson”, “Somazina”), reduce high blood pressure (“Enalapril”, “Nifedipine”), antidepressants and sedatives;
- color therapy - treatment with visual images.
The prognosis for recovery depends on how large the area was covered by the hemorrhage, as well as on how qualified the actions of doctors and rehabilitation specialists were. Hemorrhagic stroke is a very complex pathology, the consequences of which are unlikely to be completely eliminated. Maintenance treatment and rehabilitation continue for a very long time.
How long does it take for speech to be restored?
Rehabilitation of speech functions usually begins a week after the rupture of a blood vessel in the brain, provided that the patient’s condition is stable. However, there are situations when the patient is not able to start exercising even after a month. One way or another, rehabilitation therapy should begin no later than two months later. Otherwise, it will be much more difficult to regain lost abilities.
It is very difficult to give an accurate forecast regarding the time of speech recovery after a stroke. Rehabilitation is a step-by-step process with a clear sequence. The duration of each stage varies and is individual for each patient. On average, the maximum improvement in speech abilities is observed in the first six months after the illness. The entire recovery period lasts from three to five years.
Right side massage
Recovery after a stroke with paralysis of the right side with the help of massage begins on the 20th day of illness. This is an average date; the severity of the patient’s condition, age, concomitant diseases, etc. are taken into account.
The first massage sessions begin with gentle stroking of the limbs, back and neck muscles. The intensity of the effect increases from session to session, the massage therapist’s actions are aimed at restoring normal blood circulation and sensitivity in the affected part of the body.
Complications
Neurologists have to deal with numerous complications of the physical and psychological state of a stroke, which include:
- Gross disturbances of mental, cognitive, speech activity;
- Perceptual inhibition;
- Inflammatory phenomena of the bronchopulmonary, genitourinary system due to congestion in an immobilized patient;
- Depressive states with suicidal statements.
These manifestations require the closest attention and active therapy from specialists in various fields.
The Yusupov Hospital has a full range of rehabilitation equipment, including innovative ones, and a staff of highly qualified specialists who are proficient in modern techniques and types of massage and physical therapy. Their efforts, led by the country's best neurologists, are helping people recover from stroke paralysis.