Reception is conducted by:
Krivonosov Denis Sergeevich -
cardiologist, candidate of medical sciences
Make an appointment
Svitova Elena Olegovna —
Obstetrician-gynecologist. Functional diagnostics doctor. Ultrasound diagnostics doctor. Doctor of prenatal ultrasound diagnostics.
Make an appointment
Pelvic varicose veins (PVVD) is a chronic vascular pathology characterized by dilation of the pelvic veins. With the disease, the return flow of blood worsens, causing stagnation and poor circulation. Symptoms of pelvic varicose veins in women are nonspecific and are inherent in many gynecological pathologies, so literally a few decades ago the disease could not be diagnosed in time and only the symptoms were stopped, and their root causes were not eliminated.
According to a study conducted in 1999, in approximately 15-20% of cases in patients with vein disease, the reason for visiting a gynecologist was pain in the lower abdomen. However, the diagnosis was correctly made only in 2% of cases. It’s scary to imagine that about 15% of women had their uterus removed as a result of an incorrect diagnosis.
The Profimedica clinic employs professionals with extensive experience. Modern equipment from the world's best manufacturers allows specialists to diagnose and eliminate pathology at the earliest stages.
Causes of development of varicose veins of the pelvis
Today, the main cause of varicose veins is considered to be a history of pregnancy. The situation arises due to the fact that the growing fetus puts pressure on nearby organs and vessels, disrupting blood circulation. A healthy female body after childbirth is able to restore blood circulation on its own and no problems arise. However, under the influence of certain provoking factors, the tone in the vessels is not restored, leading to vascular pathology.
Factors contributing to the occurrence of the disease:
- excessive physical activity;
- sedentary lifestyle;
- diseases of the reproductive system (tumors, polycystic disease, endometriosis, etc.).
It is worth noting that varicose veins of the venous vessels of the pelvis can occur not only during pregnancy. Recently, scientists have been actively discussing the effect of hormonal contraceptives and hormone-containing drugs on the development of venous pathology. This assumption is based on the fact that the disease occurs much more often in women of childbearing age, which means hormones play a major role in this process.
Treatment at the Innovative Vascular Center
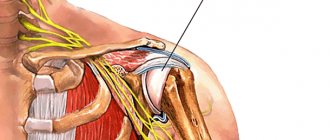
The Innovative Vascular Center uses endovascular technology to eliminate varicoceles. We perform retrograde venography of the testicular vein and embolize this dilated vein with special coils and sclerosants. This operation for varicocele does not require incisions or hospitalization for treatment, but reliably eliminates venous hypertension in the left testicle.
Early diagnosis and treatment are important for the outcome of these patients. The need for timely intervention is indicated by the fact that among patients operated on before the age of 21, the risk of infertility is minimal, and before the age of 30, the probability of childlessness increases 4 times! The earlier surgery is performed for varicocele in men, the greater the likelihood of avoiding complications. This is all the more important because modern technologies are highly effective and completely painless and have low prices.
Symptoms of varicose veins of the pelvis
All women of childbearing age need to be aware of the symptoms of varicose veins. Since the disease has a non-specific clinical picture, contacting a specialist is required when the following signs appear:
- Constant pain in the lower abdomen.
- When pain is relieved with analgesics and antispasmodics, the effect does not last long.
- The pain intensifies during and after sexual intercourse.
- There is a pronounced premenstrual syndrome.
- Painful sensations occur during hypothermia and overheating of the body, as well as during physical exertion and prolonged stay in one position.
In half of the cases with pelvic varicose veins, veins can be visualized in the area of the inner thigh, buttocks, and external genitalia. However, in the initial stages of the disease, this manifestation is absent, and it is quite difficult to independently suspect the pathology.
Medicine distinguishes 3 stages of the disease, depending on its severity. At the first stage, the diameter of the vein expansion is up to 0.5 cm. At the second stage, the expansion reaches 0.6-1 cm. At the third stage – over 1 cm.
The likelihood of developing male infertility
The time has passed when women were considered the main “culprits” of infertile marriages. According to modern data, more than 40% of cases of infertility in men are associated with dilation of the veins of the spermatic cord and testicles, and the prognosis worsens over time. Therefore, operations to eliminate varicocele should be performed at a young age. After successful treatment, the risk of testicular atrophy and infertility is significantly reduced. It is now possible to treat varicocele of any degree using endovascular surgery without incisions and pain, so you should not delay this treatment for a long time.
Diagnostics
Timely detection of the process of vascular dilatation increases the likelihood of its cure and prevention of relapses.
To diagnose pelvic varicose veins, doctors at our clinic use instrumental research methods. One of the most effective ways to detect the disease is ultrasonography. This method is carried out in conjunction with transvaginal and abdominal ultrasound, which allows specialists to obtain the necessary data for diagnosis. During ultrasonography, vascular dilation can be identified by multi-colored spots of irregular shape.
Another research method is laparoscopy. In this case, the presence of pathology is signaled by bluish-colored formations that have a thin, tense wall in the area of the uterine ligament or ovaries.
Recently, a modern diagnostic method – selective oophorography – has been gaining popularity. During the study, a contrast is performed on the patient's blood vessels, thanks to which the doctor is able to see any deviations in their structure.
A CT scan may also be performed. The method helps to see the vessels in the woman’s internal genital organs.
Pronounced discomfort during sexual intercourse and other unpleasant manifestations of the disease contribute to the deterioration of the psychosomatics of patients, which often causes diagnostic errors. The presence of a clear pathognomonic symptom, combined with the absence of signs of pathology of the pelvic organs during a traditional examination and manifestations of clear psychosomatic disorders, often leads specialists to think about the psychoneurological nature of the disease. As a result, instead of treating varicose veins, patients are prescribed consultations with sex therapists and psychotherapists.
What does it look like
A photo of a varicocele clearly demonstrates a male problem - the scrotum on one side (usually the left) is slightly lower. The skin covering the testicle does not hide the contours of the veins. When self-palpating the venous vessels, a man can feel their expansion. The patient may not even be aware of other symptoms of the disease. Palpation of the scrotum and visual examination are necessary actions for all men who care about their health. This is especially true for males planning fatherhood. You need to be regularly examined by a urologist. Medical examinations and consultations with qualified specialists are offered by the Global Clinic Center, which has extensive experience in the treatment of varicocele.
Treatment methods for pelvic varicose veins
At the Profimedica clinic, treatment of pelvic varicose veins is carried out in two ways: conservative and surgical.
In order to identify pathology, differential diagnosis is carried out using laparoscopy. The presence of varicose veins is indicated by bluish formations with a thin, tense wall in the area of the ovaries and the broad uterine ligament detected by this method.
Conservative treatment
The first method is used if the patient consults a doctor in the early stages of the disease. Conservative treatment methods include:
- Elimination of factors that provoke the development of pathology (change of sedentary or standing work, increased activity, etc.).
- Avoiding excessive physical activity.
- A balanced diet, including more fresh vegetables and fruits and excluding alcohol, cigarettes, fatty and spicy foods.
- Using a contrast shower to improve blood circulation in the body.
- Carrying out a daily set of exercises (“scissors”, “birch tree”, “bicycle”, etc.).
- The use of special breathing exercises, which are based on breathing using the muscles of the anterior abdominal wall.
- Constantly wearing compression tights.
- Taking medications that accelerate blood flow (phleboprotectors).
Surgery
If the disease was detected already in severe stages, or it was not possible to cure pelvic varicose veins in women using conservative methods, doctors may recommend surgical intervention.
During the operation, the surgeon eliminates the abnormal reflux of blood by passing through the dilated gonadal arteries. When eliminating the disease, as a rule, the method of embolization of ovarian vessels is used. For maximum precision of surgical intervention, all manipulations are carried out under the control of parallel angiography.
In rare cases, open resection or vein clipping techniques during laparotomy may also be used. In this case, the progress of the operation is monitored using an endoscope.
Our doctors
Malakhov Yuri Stanislavovich
Doctor - cardiovascular surgeon, phlebologist, Honored Doctor of the Russian Federation, Doctor of Medical Sciences, doctor of the highest category
Experience 36 years
Make an appointment
Drozdov Sergey Alexandrovich
Cardiovascular surgeon, phlebologist, Doctor of Medical Sciences
47 years of experience
Make an appointment
Causes and risk factors for the disease
In the veins surrounding the spermatic cord, a malfunction of the valve occurs, which prevents blood from flowing back. Instead of rising upward, the blood stagnates, because... is transmitted in the opposite direction. Because of this, the venous vessels become dilated and weak. The causes and risk factors of varicocele are associated with the appearance of primary and secondary reflux. The abnormal structure of the veins associated with congenital pathology leads to the complete absence of valves for the reverse outflow of blood or their atypical operation. During puberty, blood pressure on the vessels increases, and varicose changes occur in the veins near the spermatic cord. The weak walls of blood vessels inherited from birth by boys cannot cope with the flow of blood during physiological changes. As a rule, varicocele is inherited, so this should be taken into account in case of male infertility and comprehensive treatment of testicular varicose veins should be carried out. Secondary reflux occurs when the blood outflow valves stop functioning normally due to problems in the renal or vena cava. Varicose veins most often occur on the left side, because it is on the left that the venous vessels meet the renal vein. Narrowing of the lumen in the latter structure can cause varicocele. Unfavorable factors for testicular varicose veins:
- haemorrhoids;
- phlebeurysm.
The following are considered as a trigger for the appearance of varicocele:
- Hard physical labor.
- Extreme loads in sports or weight lifting.
- Lack of normal sex life.
- Professions that require long periods of standing.
- Chronic constipation.
The venous plexus of the prostate gland (Plexus venosus prostaticus, Santorini labyrinth) was first described by Santorini Giovanni Domenico (1681-1737) in 1724 [1]. This plexus, forming the dorsal venous complex, collects blood from the prostate gland (PG), the bottom of the bladder and seminal vesicles and flows into the internal iliac vein.
Pelvic venous congestion syndrome was first described by R. Gooch in 1831 in women [2]. Neurovascular bundles were described by PC Walsh and PJ Donker (1982) and are located on the dorsolateral surfaces of the pancreas between the rectum and pancreas [3]. It is believed that they do not belong to the venous plexus of the pancreas itself, although from our point of view this is not entirely correct and requires clarification (Fig. 1).
Rice. 1. Prostatic venous plexus and neurovascular bundles of the prostate gland
G.Z. Inaseridze identified two types of structure of the genitourinary venous plexus: reticular and concentrated (trunk) [4,5]. Later N.V. Kurennoy identified three types of structure of the genitourinary venous plexus: reticular; concentrated (main) and transitional [6]. O.S. Reiniger determined the prevalence of different types of structure of the genitourinary venous plexus during pelvic venography in 60 patients with benign prostatic hyperplasia: main - 53.3%, reticular - 33.3%, transitional - 13.3% of cases [7].
The syndrome of varicose veins of the pelvic organs occurs in various diseases: connective tissue dysplasia, portal hypertension, arteriovenous conflicts (Nutcracker syndrome, Posterior nutcracker syndrome, May-Thurner syndrome), tumor diseases (venous obstruction, arteriovenous fistulas) [8]. As is known, arteriovenous conflicts are the most common cause of varicocele.
The connection of varicocele with venous congestion of the pancreas was previously studied in the works of H. Sakamoto and Y. Ogawa, Y. Gat et al., A.I. Neumark et al., A.A. Capto [9-13]. Previously, we suggested that the anatomical vascular connection between the organs of the scrotum and the pelvic organs occurs in two ways: through the internal iliac vein, through the vein of the vas deferens (Fig. 2) [14].
Rice. 2. Anatomical connection of the organs of the scrotum and pelvis through the internal iliac vein (picture on the left) and through the vein of the vas deferens (picture on the right)
With retrograde phlebotesticulography with a 10-second delay, many researchers noted contrasting of the pericapsular area of the pancreas in patients with varicocele (Fig. 3) [15,16].
Rice. 3. Retrograde renal phlebotesticulography. Contrasting of the paraprostatic venous plexus on the side of the varicocele. On the left, discharge through the internal iliac vein predominates. In the middle and on the right, discharge through the vein of the vas deferens predominates
In continuation of the conducted research, in this work we made an attempt to determine quantitative criteria for varicose veins of the pelvic organs in men and propose a classification of varicose veins of the prostate gland.
MATERIALS AND METHODS OF RESEARCH
From September 2008 to September 2021, 206 patients with varicocele were examined and operated on. The examination of patients included a survey, physical examination, Ivanissevich test, semen analysis, ultrasound examination of the scrotal organs and transrectal ultrasound (TRUS) of the pancreas, color Doppler ultrasound of the pancreas at rest and during the Valsalva maneuver. Surgical treatment was carried out through a transscrotal approach along the Wesling line. Control examinations were carried out 3 and 6 months after surgery. Considering that the volume of the pancreas depends on the period of sexual abstinence, all ultrasound examinations were performed with the same period of abstinence - three days [17]. In cases of recurrent varicocele, magnetic resonance imaging of the inferior vena cava and pelvic vessels, retrograde venography of the renal and iliac vessels with phlebotonometry were performed.
RESEARCH RESULTS
The age of the patients ranged from 18 to 83 years and averaged 35.3 years. The diagnosis of varicocele was verified by physical examination, Ivanissevich test and scrotal Doppler ultrasound. Varicocele was left-sided in 131 (63.6%), right-sided in 3 (1.5%) and bilateral in 72 (34.9%) patients. When analyzing the ejaculate, pathospermia was found in 127 patients (61.7%), and an increased content of leukocytes (more than 1 million in 1 ml.) - in 148 patients (71.8%).
According to ultrasound of the scrotum, epididymal cysts were found in 112 (54.4%) patients. Combined pathology of the scrotal organs with varicocele was noted in 148 patients (71.8% of cases): bilateral varicocele, epididymal cyst, spermatocele, hydrocele, adhesions in the area of the epididymis and testicle, large hydatid of Morgagni, calculus of the inner lining of the testicle, lipoma spermatic cord. It was this circumstance that was the indication for the use of operative access along the Wesing line, in which it would be possible to simultaneously correct all identified problems from one incision.
According to TRUS of the pancreas, in all cases in patients with varicocele, visualization of the veins of the paraprostatic plexus on the side of the identified varicocele was noted. The classification presented in Table 1 was adopted as a working ultrasound classification of pancreatic varicose veins.
Table 1. Ultrasound classification of prostate varicose veins
| Stage | Definition of varicose veins | Maximum vein diameter, mm |
| 1 | Visible | 1- 4 |
| 2 | Significant | 5-10 |
| 3 | Expressed | > 10 |
The results of determining the stage of pancreatic varicose veins in 206 patients with varicocele are presented in Table 2.
Table 2. Prevalence of stages of prostate varicose veins in patients with varicocele
| Stage | Left-handed | Bilateral N=72 | Right-handed | Total N=206 | |
| N=131 | Left | On right | N=3 | ||
| 1 | 12 | 14 | 14 | — | 40 |
| 2 | 71 | 32 | 42 | 3 | 148 |
| 3 | 48 | 26 | 16 | — | 90 |
In all cases, the diameter of the veins of the prostatic venous plexus was positively correlated with the diameter of the veins of the right and left pampiniform plexus. In case of right-sided varicocele, according to TRUS data, dilatation of the veins of the paraprostatic venous plexus on the right was noted (Fig. 4).
Rice. 4. TRUS of the pancreas in patient M., 47 years old, with stage 2 right-sided varicocele. The volume of the pancreas is 35.0 cm3. The maximum diameter of the veins on the right is 3.5; 3.6 and 2.2 mm. Stage 1 varicose veins of the pancreas or visible varicose veins. Reticular type of venous plexus. BPH, chronic prostatitis. From the anamnesis, October 23, 2008, Ivanissevich surgery on the left
In most cases, patients had left-sided varicocele. At the same time, according to TRUS data, dilation of the veins of the paraprostatic venous plexus on the left was noted (Fig. 5).
Rice. 5. TRUS of the pancreas in patient L., 69 years old with left-sided varicocele stage 2. The volume of the pancreas is 16.5 cm3. The maximum diameter of the veins on the left is 6.0 mm. Stage 2 varicose veins of the pancreas or significant varicose veins. Main type of venous plexus. Chronic calculous prostatitis
With bilateral varicocele, dilation of the veins of the paraprostatic venous plexus on both sides was noted (Fig. 6).
Rice. 6. TRUS of the pancreas in patient K., 33 years old, with stage 3 bilateral varicocele. The volume of the pancreas is 22.3 cm3. The maximum diameter of the veins on the left is 10.9 and 18.3 mm, on the right 12.5 mm. Stage 3 varicose veins of the pancreas or pronounced varicose veins. Main type of venous plexus. Chronic calculous prostatitis
With a maximum vein diameter of 1 to 4 mm (visible varicose veins), the blood flow velocity in them was 1-3 cm/sec, and with the Valsalva maneuver - 5 cm/sec. With a maximum vein diameter of 5 to 10 mm (significant varicose veins), the blood flow velocity in them was 3-5 cm/sec, and with the Valsalva maneuver - 5-15 cm/sec. When the maximum diameter of the veins was more than 10 mm (pronounced varicose veins), the blood flow velocity in them was more than 5 cm/sec, and with the Valsalva maneuver more than 15 cm/sec (Fig. 7).
Rice. 7. Color Doppler TRUS of the pancreas in patient K. 42 years old with stage 3 bilateral varicocele. The diameter of the vein on the left is 14.3 mm, the blood flow speed is 5.9 cm/s (on the left). The blood flow velocity during the Valsalva maneuver is 17.4 cm/s (right). Severe varicose veins of the pancreas (stage 3)
In 93 patients (45.1% of cases), there were pronounced local changes in the pancreas in the form of foci of hypoechogenicity, fibrosis and calcification on the side of the varicocele. In 22 patients (10.7% of cases), TRUS revealed pancreatic cysts. We did not note any connection between the severity, localization of varicocele, severity of varicose veins of the pancreas and the size and localization of pancreatic cysts.
6 months after surgery, without any additional treatment, the following changes occurred in patients: 1) the diameter of the veins of the paraprostatic venous plexus on the side of the varicocelectomy decreased by 1.5 - 2.5 times in 175 patients (85.0%) (Fig. 8,9), 2) pathospermia remained in 88 patients (spermatogenesis was restored in 30.7% of cases), 3) pyospermia remained in 52 patients (disappeared in 64.9% of cases).
Rice. 8. TRUS of the pancreas in patient K., 30 years old with bilateral varicocele on 02/01/2016 (left) and 4 months (06/01/2016) after simultaneous bilateral varicocelectomy, plastic surgery of the testicular membranes according to Winkelmann from the midscrotal access along the Wesling line (from 02/09. 2016) (right)
Rice. 9. TRUS of the pancreas in patient Z., 40 years old with bilateral varicocele on 12/09/2015 (left) and 6 months (06/10/2016) after simultaneous bilateral varicocelectomy, excision of epididymal cysts of both testicles, plastic surgery of the membranes of the right and left testicle according to Winkelmann from the scrotum access via the Wesling line (from 12/22/2015) (right)
In the postoperative period, the development of recurrent left-sided and right-sided varicocele after left-sided varicocelectomy was noted in 5 patients (2.4%). A magnetic resonance imaging study of the inferior vena cava and pelvic vessels revealed MayThurner syndrome in all 5 patients (Fig. 10).
Rice. 10. Magnetic resonance imaging of the inferior vena cava and pelvic vessels in patients with recurrent varicocele. May-Thurner syndrome
All these patients underwent retrograde venography and phlebotonometry of the renal and iliac vessels. Phlebotonometry confirmed hypertension in the left internal iliac vein (pressure on average 31 mm Hg) and in the right internal iliac vein (pressure on average 27 mm Hg), which was 6-8 times higher than the average statistical norm. Phlebography revealed pronounced varicose veins of the paravesical and paraprostatic venous plexus due to May-Thurner syndrome (Fig. 11). All these patients underwent sclerotherapy of decompensated testicular veins.
Rice. 11. Retrograde venography of the left common iliac vein and selective venography of the left internal iliac vein in a patient with varicocele and May-Thurner syndrome. Severe varicose veins of the paravesical and paraprostatic venous plexus on the left
DISCUSSION
The criteria for varicose veins of the pelvic organs are currently determined based on the results of the following research methods: 1) ultrasound, 2) phlebography, 3) computed tomography (CT) or magnetic resonance imaging (MRI). These criteria have two features: they differ significantly from each other in assessing the diameter of dilated veins; describe varicose veins of the pelvis in women. Below we present a summary table 3, which presents the point of view of different authors on the criteria for pelvic varicose veins in women.
Table 3. Criteria for varicose veins of the pelvic organs in women
| Author | Research method | Vein diameter | Blood flow speed |
| Beard RW et al. (1984)[18]; Ignacio EA et al. (2008) [19] | Ultrasound | > 4 mm | < 3 cm/s |
| Inal M. et al. (2014) [20]; | Ultrasound | > 5-6 mm | ~ 3 cm/s |
| Ganeshan A. et al. (2007) [21]; | Ultrasound | > 6 mm | 3 cm/s |
| Leal Monedero J. et al. (2006) [22]; Barros FS et al. (2010) [23] | Ultrasound | > 7 mm | — |
| Black CM et al. (2009) [24]; Kim HS et al. (2006) [25]; Park SJ et al. (2004) [26]; Beard RW et al. (1984) [27] | Phlebography | > 5 mm | — |
| Kennedy A., Hemingway A. 1990 [28] | Phlebography | > 10 mm | — |
| Coakley FV et al. (1999) [29] | CT, MRI | Peri-uterine > 4 mm, ovarian > 8 mm | — |
Criteria for varicose veins of the pelvic organs in men A.Yu. Tsukanov and R.V. Lyashev considered dilation of the veins of the paraprostatic plexus to be more than 5 mm and/or the presence of blood flow reflux during the Valsalva maneuver during duplex angioscanning using a rectal sensor [30]. The criteria we proposed for varicose veins of the pelvic organs in men and the classification of this disease were based on measuring the maximum diameter of the veins of the paraprostatic plexus. We believe that venous dilatation is secondary to pathological blood flow and its duration, so measuring the maximum diameter of the veins can fairly accurately reflect the true state of the paraprostatic plexus veins. Considering that TRUS of the pancreas is a routine research method (in contrast to phlebography and phlebotonometry, CT, MRI), and based on the fact that the classification of varicose veins of the pancreas should have practical significance, we decided to base it on the results of ultrasound examination.
CONCLUSION
We have proposed an ultrasound classification of pancreatic varicose veins, which includes three stages: 1 - “visible varicose veins” with a maximum vein diameter of 1-4 mm, 2 - “significant varicose veins” with a maximum vein diameter of 5-10 mm and 3 - “pronounced varicose veins" with a maximum vein diameter > 10 mm. Our data indicate that the detection of dilated veins of the paraprostatic plexus according to TRUS may indicate the presence of varicocele and associated venous congestion of the pancreas. In all cases, pancreatic varicose veins were detected on the side of the varicocele and were ipsilateral in case of unilateral varicocele and bilateral in case of bilateral varicocele. 6 months after the operation, without any additional treatment, the diameter of the veins of the paraprostatic venous plexus decreased by 1.5-2.5 times in 85.0% and pyospermia disappeared in 65.0% of cases. This allows us to identify varicocele as one of the causes of pelvic disorders and prostatopathies associated with venous congestion. In case of recurrent varicocele, it is advisable to conduct a magnetic resonance examination of the inferior vena cava and pelvic vessels, phlebography and phlebotonometry of the renal and iliac vessels to confirm or exclude May-Thurner syndrome.
LITERATURE
1. Santorini GD Observationes anatomicae. Venice: Giovanni Battista Recurti, 1724; X: 193-194.
2. Gooch R. In: An Account of Some of the Most Important Diseases Peculiar to Women. Murray J, editor. London: Murray 1831: 1829 p.
3. Walsh PC, Donker PJ. Impotence following radical prostatectomy: Insight into etiology and prevention. J Urol 1982;128(3):492-497.
4. Inasaridze G.Z. Experimental data on ligation of the main veins of the bladder and clinical observations of similar changes in patients with pathology in the genitourinary venous plexus. Theses of the Ukrainian Congress of Urologists, Kyiv, 1939. P.78-79, 212-230.
5. Inasaridze G.Z. Extreme types of variability of the genitourinary venous plexus and their clinical significance: dissertation. Dr. med. Sci. M. 1940.
6. Kurennoy N.V. Details of the macroscopic structure of the urogenital venous plexus and their possible significance. Sat. "Issues of Urology". Kyiv, 1964. pp. 28-53.
7. Reiniger O.S. The role of the anatomical structure of the genitourinary plexus in the pathogenesis of bleeding after adenomectomy. Abstracts of reports of the IV Plenum of the All-Russian Scientific Society of Urologists. - M, - 1973, - P. 67-68.
8. Kapto A.A., Zhukov O.B. Varicose veins of the pelvis in men (literature review). Andrology and genital surgery. 2016; 17(2):10-19.
9. Sakamoto H, Ogawa Y. Is varicocele associated with underlying venous abnormalities? Varicocele and the prostatic venous plexus. J Urol 2008; 180(4):1427-1431. doi: 10.1016/j.juro.2008.06.048.
10. Gat Y, Gornish M. Reversal of Benign Prostate Hyperplasia by Super-selective Intraprostatic Androgen Deprivation Therapy. Euro Urol Rev 2009; 4(1):10-14.
11. Gat Y, Joshua S, Gornish MG. Prostate cancer: a newly discovered route for testosterone to reach the prostate: Treatment by super-selective intraprostatic androgen deprivation. Andrologia 2009; 41(5):305-315. doi: 10.1111/j.1439-0272.2009.00972.x.
12. Neymark A.I., Popov I.S., Gazamatov A.V. Features of microcirculation of the prostate gland and gonads in young men suffering from isolated varicocele and varicocele in combination with pelvic congestion. Experimental and Clinical Urology 2013; (2): 56-60.
13. Kapto A.A. The phenomenon of prostate varicose veins in patients with varicocele. Collection of abstracts of the 11th Congress of the Professional Association of Andrologists of Russia. May 25-28, 2021, Sochi, Dagomys. P.15-16.
14. Kapto A.A. Clinical aspects of vascular anatomy in patients with varicocele (lecture). Experimental and Clinical Urology 2006; (2):70-79.
15. Gat Y, Gornish M, Heiblum M, Joshua S. Reversal of benign prostate hyperplasia by selective occlusion of impaired venous drainage in the male reproductive system: novel mechanism, new treatment. Andrologia. 2008;40(5):273-81.
16. Osipov N.G., Teplinskaya N.P., Sabalenko Yu.A., Alekseychuk G.I. Changes in the architectonics of the veins draining the pampiniform plexus and spermatogenesis in patients with newly diagnosed and recurrent varicocele. Andrology and genital surgery 2014; (2):30-36.
17. Kapto AA.Value assessment of prostate tone in the complex treatment of patients with chronic prostatitis. Int Jmmunorehabilitation 2002; 4(2):316-317.
18. Beard RW, Highman JH, Pearce S, Reginald PW. Diagnosis of pelvic varicosities in women with chronic pelvic pain. Lancet 1984; 2:946-949.
19. Ignacio EA, Dua R, Sarin S, Harper AS, Yim D, Mathur V, et al. Pelvic congestion syndrome: diagnosis and treatment. Semin Intervent Radiol 2008; 25(4):361-8. doi:10.1055/s-0028-1102998.
20. Inal M, Karadeniz Bilgili MY, Sahin S. Nutcracker accompanying pelvic congestion syndrome; color doppler sonography and multislice CT findings: A case report. Iran JRadiol 2014;11(2):e11075 doi: 10.5812/iranjradiol.11075.
21. Ganeshan A, Upponi S, Hon LQ, Uthappa MC, Warakaulle DR, Uberoi R. Chronic pelvic pain due to pelvic congestion syndrome: the role of diagnostic and interventional radiology. Cardiovasc Inervent Radiol 2007; 30(6):1105-1111.
22. Leal Monedero J, Ezpeleta SZ, Castro FC, Senosiain LDC. Recidiva varicosa de etiologia pelvica. In: Thomaz JB, Belczack CEQ. Tratado de flebologia e lin-fologia. Rio de Janeiro: Livraria Rubio; 2006. P. 301-322.
23. Barros FS, Perez JMG, Zandonade E, Salles-Cunha SX, Monedero JL, Hilel ABS, et al. Evaluation of pelvic varicose veins using color Doppler ultrasound: comparison of results obtained with ultrasound of the lower limbs, transvaginal ultrasound, and phlebography. J Vasc Bras 2010; 9(2):15-20.
24. Black CM, Thorpe K, Nielsen R. Diagnosis and Endovascular Management of PVI. Pelvic venous insufficiency remains an underdiagnosed but treatable cause of chronic pelvic pain. Endovascular today. 2009. P. 67-71. Available from: https://evtoday.com/2009/07/EVT0709_08.php
25. Kim HS, Malhotra AD, Rowe PC, Lee JM, Venbrux AC. Embolotherapy for pelvic congestion syndrome: long-term results. J Vasc Intervent Radiol 2006;17(2, Pt 1):289-297. DOI:10.1097/01.RVI.00001948 70.11980.F8
26. Park SJ, Lim JW, Ko YT, Lee DH, Yoon Y, Oh JH, et al. Diagnosis of pelvic congestion syndrome using transabdominal and transvaginal sonography. AJR Am J Roentgenol 2004;182(3):683-688. DOI:10.2214/ajr.182.3.1820683
27. Beard RW, Highman JH, Pearce S, Reginald PW. Diagnosis of pelvic varicosities in women with chronic pelvic pain. Lancet 1984; 2(8409):946-949.
28. Kennedy A, Hemingway A. Radiology of ovarian varices. Br J Hosp Med 1990;44(1):38-43.
29. Coakley FV, Varghese SL, Hricak H. CT and MRI of pelvic varices in women. J Comput Assist Tomogr 1999; 23(3):429-434.
30. Tsukanov A.Yu., Lyashev R.V. Violation of venous blood flow as a cause of chronic abacterial prostatitis (chronic pelvic pain syndrome). Urology 2014; (4):37-42.
| Attached file | Size |
| 1.41 MB |
‹ Analysis of dietary patterns in urolithiasis Up Vaginal access in surgery of ureterovaginal fistulas: literature review and clinical case ›