Causes
The causes of the disease have not been fully investigated. It is known that the disease and syndrome are provoked by environmental factors that have a negative impact on the body. An important role is played by the predisposition of the body, problems with the regulation of B-lymphocytes in the blood.
With pathology of the exocrine glands, degenerative processes and necrosis develop, acinar glands atrophy, and the functioning of the lacrimal and salivary glands deteriorates. Due to damage to the nerve fibers, the mucous membrane dries out. Autoimmune processes spread because the body is unable to compensate for its basic needs.
Women are more likely to develop the syndrome; men account for no more than 10% of all visits to the doctor. This is explained by frequent changes in hormonal levels in the female body - during pregnancy or lactation, menopause.
Predisposing factors
- Severe hypothermia or overheating of the body.
- Overdose of drugs.
- Stressful situations, mood swings, depression.
- Development of autoimmune diseases.
- Hypersensitivity of the immune system upon contact with new substances.
- Genetic predisposition.
Pathogenesis
The autoimmune process leads to apoptosis of secreting cells and the epithelium of the excretory ducts, causing damage to the glandular tissue.
Sjögren's syndrome is associated with increased cerebrospinal fluid levels of IL-1RA, an interleukin-1 (IL-1) antagonist. This suggests that the disease begins with an increase in the activity of the IL-1 system, which entails a compensatory increase in IL-1RA to reduce the binding of IL-1 to receptors. On the other hand, Sjogren's syndrome is characterized by a decrease in the level of IL-1 in saliva, which can lead to inflammation of the oral mucosa and its dryness.
Symptoms
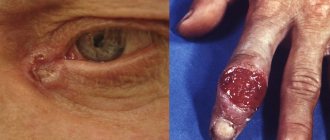
The symptoms of Sjögren's disease are quite varied. Most often, the salivary glands are affected, resulting in the development of sialadenitis or mumps, submaxillitis. At all stages of the disease, the patient is accompanied by keratoconjunctivitis or conjunctivitis, dryness of the mucous membrane of the eyes. For this reason, doctors recommend special moisturizing drops to help reduce the symptom. A characteristic symptom is recurrent stomatitis, atrophic or subatrophic rhinopharyngolaryngitis. The red border of the lips dries out and ulcers appear on it.
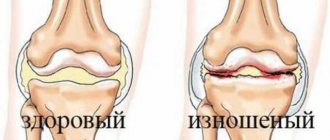
70% of patients have arthralgia - joint pain. In some cases, there is recurrent non-erosive arthritis that affects the small joints in the hands.
During the syndrome, kidney problems develop. Nephrotic syndrome, interstitial nephritis, or glomerulonephritis may occur. The epithelial tissues of the renal tubular apparatus and biliary tract are gradually affected.
The peripheral nervous system is affected, as a result of which the patient develops tunnel neuropathy, polyneuropathy, mononeuritis and other pathologies.
Sjögren's disease
The paper fully considers the etiology and pathogenesis, pathomorphology and diagnosis, including differential diagnosis, of Sjogren's syndrome, gives recommendations on the treatment of the syndrome and symptomatic therapy of its ophthalmological, dental, gastroenterological, and other manifestations. IN AND.
Vasilyev – Institute of Rheumatology RAMS, Moscow VI Vasilyev – Institute of Rheumatology Academician of the Russian Academy of Medical Sciences, Moscow
B
Sjögren's disease (N. Sjogren, Swedish ophthalmologist, 1899–1986) - Sjögren's disease is a systemic autoimmune disease related to diffuse connective tissue diseases; characterized by damage to many secreting epithelial (exocrine) glands, mainly salivary and lacrimal. There is also Sjogren's syndrome (damage to the lacrimal glands with the development of dry keratoconjunctivitis and salivary glands like parenchymal parotitis), accompanying rheumatoid arthritis, diffuse connective tissue diseases, hepatobiliary diseases and other autoimmune diseases. BS is the most common pathology among diffuse connective tissue diseases and occurs in women 10–25 times more often than in men, usually at the age of 20–60 years, and is much less common in children. Epidemiological studies conducted in recent years have made it possible to establish the presence of BS in 0.59–0.77% of the general population and in 2.7% of people over 50 years of age. Etiology unknown. Most researchers consider BS as a consequence of immunopathological reactions to a viral infection, presumably retroviral. The following facts support the possible involvement of retroviruses in the development of HD: • infection and persistence of immune system cells, such as CD 4+ lymphocytes and macrophages, in potential target organs, for example, the salivary glands; • similarities between known retroviral infections (eg HIV) and BS; • development of a disease resembling BS in transgenic mice having HTLV – 1 + tax gene; • increasing the content of cross-reacting antibodies to retrovirus antigens; • isolation of retroviral elements from cell cultures obtained from biopsy samples of the salivary glands of patients with sclerosis; • detection of antigens that react with monoclonal antibodies to some retrovirus antigens in lymphoid infiltrates in BS. Indirect evidence of the viral etiology of BS is the similarity of immunological disorders (polyclonal b-cell activation, a large number of immune complexes, decreased levels of serum b2-microglobulin, the presence of acid-labile interferon, a decrease in the amount of interleukin-2 (IL-2) and natural killer cells in the blood in BS and AIDS caused by known retroviruses, but direct evidence of the viral etiology of the disease has not yet been obtained.
Pathogenesis
The most recognized hypothesis is the autoimmune genesis of BS, which is supported by the frequent detection in patients of both organ-specific (to the epithelium of the ducts of the salivary glands and pancreas, parietal cells of the stomach, thyroglobulin, etc.) and organ-nonspecific autoantibodies (for example, rheumatoid and antinuclear factors, antibodies to some nuclear antigens - SS-A/Ro and SS-B/La). It is assumed that autoimmune disorders in HD are multifactorial in nature and consist of a combination of the following elements: • genetic control associated with the activity of specific immune response genes; • immune control, influenced by T-dependent lymphocytes; • possible viral infection; • influence of sex hormones on immune regulation; • influence of stress on the immune response. Cases of BS in identical twins, a significant prevalence of other autoimmune disorders in the families of BS patients, as well as an increased frequency of histocompatibility antigens DR 3 and B 8 in BS patients indicate the genetic determination of the disease. It has been shown that the activity of T-suppressors initially decreases, which leads to an increase in the activity of T-helpers and chronic stimulation of b-lymphocytes.
Pathomorphology
The main and pathognomonic morphological sign of BS is lymphoplasmatic infiltration of the parenchyma of the secreting glands. The majority of cells infiltrating the glands are T-lymphocytes, while b-lymphocytes account for 20%, monocytes, macrophages and NK cells - no more than 5%, 60-70% of T-lymphocytes are CD 4+ cells. Lymphoid infiltrates synthesize large amounts of IgG, IgM, rheumatoid factors, and produce large amounts of IL (IL-2, IL-6, IL-10), and their amount directly depends on the degree of lymphoid infiltration. In a third of patients, lymphoplasma cell infiltration is not limited to the tissue of the secreting epithelial glands and takes on a generalized character with the involvement of muscles (myositis), lungs (lymphocytic infiltrates with the development of interstitial pneumonia or foci of infiltration like pseudolymphoma), kidneys (interstitial nephritis), blood vessels (productive, productive-destructive vasculitis), causing functional changes in the affected organs with the development of various clinical manifestations. Involvement of the phagocytic macrophage system in the process in 5–10% of BS leads to the development of malignant lymphoproliferative diseases, mainly b-cell lymphomas and Waldenström macroglobulinemia.
Clinical picture
Clinical manifestations of BS can be divided into glandular and extraglandular. Glandular symptoms are caused by damage to the secreting epithelial glands, characterized mainly by their hypofunction. A constant clinical sign of damage to the lacrimal glands
with BS there is dry keratoconjunctivitis, associated with a decrease in the secretion of tear fluid.
Patients complain of burning sensations, “scratching” and “sand” in the eyes. Often there is itching of the eyelids, redness, and accumulation of viscous white discharge in the corners. Later, photophobia, narrowing of the palpebral fissures appear, and visual acuity decreases. A sharp decrease or complete absence of tear production leads to the development of pinpoint infiltrates, as well as the formation of deep xerosis of the cornea and its clouding. Secondary bacterial conjunctivitis is often associated. Enlargement of the lacrimal glands in BS is rarely observed. A serious complication of dry keratoconjunctivitis is the appearance of infiltrates, which can lead to the formation of purulent ulcers and perforation of the cornea. The second mandatory and constant sign of BS is damage to the salivary glands
with the development of chronic parenchymal mumps.
It is characterized by xerostomia and enlargement of the salivary glands. Often, even before the appearance of these signs, dryness of the red border of the lips, seizures, stomatitis, enlargement of regional lymph nodes, and multiple (usually cervical) dental caries are noted. Approximately half of the patients experience a recurrent course of mumps; in some patients, after the next exacerbation, the parotid glands remain constantly enlarged. In a third of patients, a gradual enlargement of the parotid glands is observed, leading to a characteristic change in the oval of the face, described in the literature as a “hamster face” or “chipmunk face.” The parotid glands are painless or slightly painful on palpation. Enlargement of the submandibular, sublingual and palatine salivary glands is rare. In the initial stage of the disease, dry mouth appears only during physical activity and anxiety. In the severe stage, dry mouth becomes constant, accompanied by the need to drink dry food and the desire to moisten the mouth during a conversation. The oral mucosa becomes bright pink and is easily injured. There is little free saliva, it is foamy or viscous. The tongue is dry. The lips are covered with crusts, symptoms of angular stomatitis and glossitis are observed, and a secondary infection, including fungal and viral, may occur. Multiple cervical dental caries is characteristic. The late stage is manifested by severe dryness of the mouth, the inability to speak, or swallow food without washing it down with liquid. The lips of such patients are dry, cracked, the oral mucosa shows signs of keratinization, the tongue is folded, its papillae are atrophic, free saliva is not detectable in the oral cavity. Partial or complete adentia is observed due to the progression of dental caries. Dryness of the nasopharynx
with the formation of dry crusts in the nose and in the lumen of the auditory tubes can lead to temporary deafness and the development of otitis media.
Dryness of the pharynx and vocal cords causes hoarseness. Subatrophic (or atrophic) rhinopharyngolaryngitis develops. Frequent complications are secondary infections: sinusitis, recurrent tracheobronchitis and pneumonia. Damage to the apocrine glands of the external genitalia
is observed in approximately 1/3 of patients with BS.
The vaginal mucosa is hyperemic, dry, atrophic, and patients are often bothered by burning pain and itching. A common symptom of sclerosis is dry skin. Sweating may be reduced. Changes in the digestive system
during BS are observed frequently and are diverse in nature.
Dysphagia is caused by the presence of xerostomia, as well as, in some cases, hypokinesia of the esophagus. Many patients develop chronic atrophic gastritis with severe secretory insufficiency, clinically manifested by gastric dyspepsia syndrome (severity and discomfort in the epigastrium after eating, belching of air, nausea, loss of appetite). Pain in the epigastric region is less common. There is a direct relationship between the degree of xerostomia and inhibition of the secretory function of the stomach. Pathology of the biliary tract (chronic cholecystitis) and liver (persistent hepatitis) is observed in most patients. There are complaints of heaviness and pain in the right hypochondrium, bitterness in the mouth, nausea, and poor tolerance to fatty foods. Involvement of the pancreas in the process (pancreatitis) is manifested by pain and dyspeptic syndromes. Clinical signs of intestinal damage (colitis) are usually mild, but most patients with BS are present. Extraglandular manifestations of BS
are very diverse and systemic in nature.
Arthralgia, slight stiffness in the morning, recurrent non-erosive (i.e. without bone destruction on radiographs) arthritis of small, less often large joints and painful flexion contractures occur in approximately 2/3 of patients. Signs of molymyositis (myalgia, moderate muscle weakness, a slight increase in the level of creatine phosphokinase in the blood) are observed in 5–10% of patients. It is extremely rare that severe myositis may develop. Most patients with BS have regional lymphadenopathy
(enlargement of the submandibular, cervical, occipital, supraclavicular lymph nodes), and in 1/3 of patients the lymphadenopathy is generalized.
In the latter case, hepato- and splenomegaly are often detected. The incidence of these symptoms increases with the presence of vasculitis and the development of malignant lymphoproliferation (pseudolymphomas, b-cell lymphomas and Waldenström's macroglobulinemia). Various respiratory tract lesions
are observed in 50% of patients.
A targeted X-ray and functional examination reveals signs of lung damage in 2/3 of patients. Dry throat, soreness and scratching, dry cough and shortness of breath are the most common complaints. Dyspnea most often indicates damage to the pulmonary parenchyma (interstitial pneumonia and interstitial fibrosis). Recurrent dry and effusion pleurisy is observed relatively rarely with BS. In 20–30% of patients, various lesions of the kidneys
, more often of the tubular apparatus: tubular acidosis, generalized aminoaciduria and phosphaturia with the development in some cases of nephrogenic diabetes.
The consequences of tubular acidosis can be osteomalacia, nephrocalcinosis and hypokalemia, leading to muscle weakness. The development of chronic renal failure is the result of a long course of tubular acidosis. Diffuse glomerulonephritis of a membranous-proliferative or membranous type of an immunocomplex nature is observed much less frequently. Severe forms of glomerulonephritis with nephrotic syndrome and the development of renal failure are observed in patients with BS with cryoglobulinemia. Acute renal failure due to renal artery thrombosis can cause death in patients with BS with productive-destructive vasculitis. In 1/3 of patients with BS, Raynaud's syndrome
, more often its erased forms.
In BS, there are two types of vasculitis: productive and productive-destructive. Changes in the type of obliterating endarteritis are also observed, which are not independent in nature and often accompany productive-destructive (70%), less often productive (30%) vasculitis. Cutaneous vasculitis in BS is caused by damage to small and medium-sized vessels. With BS, capillaritis, livedo reticularis, and various types of purpura are observed. Recurrent hypergammaglobulinemic and cryoglobulinemic purpura are observed in approximately 1/4 of patients. Pinpoint hemorrhagic rashes most often appear on the skin of the legs, but over time they spread higher and can be found on the skin of the thighs, buttocks and abdomen. The rash is accompanied by itching, painful burning and increased skin temperature in the affected area. Patients with long-term recurrent hypergammaglobulinemic purpura usually develop skin hyperpigmentation due to hemosiderin deposition. Skin biopsies of such patients reveal a picture of productive vasculitis. Severe forms of vasculitis with the development of multiple ulcerative-necrotic changes in the skin of the extremities, trunk and face, the formation of long-term non-healing ulcers and the occurrence of gangrene are observed in patients with recurrent cryoglobulinemic purpura. It is characterized by the appearance of rashes like vesicles and pustules with hemorrhagic contents. Skin biopsies reveal signs of productive-destructive vasculitis, often its necrotizing form. Patients with BS with productive vasculitis are characterized by the presence in the blood of high levels of g-globulin, circulating immune complexes, and rheumatoid factor, while the immunological marker of productive-destructive vasculitis is cryoglobulinemia, found in 95% of patients with this form of vasculitis. Clinical signs of peripheral polyneuropathy
with sensory disturbances of the “socks” and “gloves” type, paresthesia, less commonly, polyneuritis and mononeuritis, neuritis of the facial and trigeminal nerves are observed in a third of patients.
Myelopolyradiculoneuritis and cerebrovasculitis can develop much less frequently in patients with productive-destructive vasculitis. Clinically obvious signs of hypothyroidism
are found in 10–15% of patients (extremely rare - thyrotoxicosis).
Antibodies to thyroglobulin, the microsomal fraction of the thyroid gland and thyroid-stimulating hormone are detected in half of patients with BS; It is assumed that subclinical thyroid lesions are more common. Thus, endocrine glands, as well as exocrine glands, can be targets for immune attacks in HD. The known similarities in genetic susceptibility of HLA-DR 3 and the histological similarities between Hashimoto's thyroiditis and HS support speculation that similar mechanisms may be involved in these diseases. Insulin-dependent diabetes and pernicious anemia are rare in patients with BS. A third of patients experience allergic reactions
, more often to antibiotics, sulfonamides, novocaine, group B drugs, as well as to chemicals (washing powders, etc.) and food products.
Laboratory research
The most informative laboratory indicators for BS are high ESR, leukopenia, hypergammaglobulinemia (80–70%), the presence of antinuclear and rheumatoid factors (90–100%), as well as antibodies to soluble nuclear antigens SS-A/Ro and SS-B/La (60–100%). In a third of patients, cryoglobulins are detected, which can be polyclonal or monoclonal depending on the immunoglobulins included in their composition. Monoclonal immunoglobulins (IgM and IgA) with light chains are detected in cryoprecipitates and biopsies of the salivary glands in the early stages of the disease, which makes it difficult to differentiate between BS with transformation into malignant lymphoma and benign lymphoproliferation in this disease.
Diagnosis
In outpatient settings, it is advisable to take into account various combinations of the following symptoms: • arthralgia or (less often) non-erosive arthritis of the small joints of the hands; • recurrent parotitis and gradual enlargement of the parotid glands; • dryness of the oral mucosa (nasopharynx) and the rapid development of multiple, mainly cervical, dental caries; • recurrent chronic conjunctivitis; • Raynaud's syndrome; • persistent increase in ESR (over 30 mm/h); • hypergammaglobulinemia (over 20%); • presence of rheumatoid factor in the blood (titer more than 1:80). Although none of these signs, taken individually, is specific for BS, the presence of four or more signs allows in 80–70% of cases to suspect and subsequently confirm the diagnosis of BS using special research methods.
Criteria for diagnosis of BS
• Keratoconjunctivitis sicca: a) decreased tear production after stimulation with ammonia, Schirmer test (less than 10 mm/5 min); b) staining of the epithelium of the conjunctiva and cornea with rose bengal or fluorescein, followed by biomicroscopy. • Parenchymal parotitis: a) detection of cavities more than 1 mm during sialography; b) the level of stimulated salivary secretion is less than 2.5 ml/5 min; c) focal-diffuse, diffuse lymphoplasma cell infiltration in biopsy samples of the salivary glands of the lower lip. • Laboratory signs of systemic autoimmune disease: a) positive rheumatoid (antinuclear) factor; b) detection of Ro/La antinuclear antibodies. The diagnosis of definite BS can be made if three criteria are met and other diffuse connective tissue diseases, rheumatoid arthritis and autoimmune hepatobiliary diseases are excluded. Differential diagnosis for BS includes rheumatoid arthritis, systemic lupus erythematosus, autoimmune diseases of the liver and biliary tract in combination with Sjögren's syndrome. Despite the long-term existence of arthralgia for BS, in contrast to rheumatoid arthritis, the presence of persistent arthritis and joint deformities is uncharacteristic; X-rays do not show signs of erosive joint damage; arthritis with BS usually completely disappears on the 2-3rd day after the administration of small doses of corticosteroids. Systemic lupus erythematosus is characterized by erythematous rashes on the face in the form of a “butterfly”, endocarditis, exudative serositis, nephrotic syndrome, the presence of LE cells in the blood, etc. In chronic active hepatitis, biliary cirrhosis of the liver, in contrast to BS, disturbances in liver function tests are constant a sign that markers of the hepatitis B virus are detected in the blood; the material obtained from liver biopsy reveals the morphological changes inherent in these diseases. Some symptoms that occur with BS can be observed in various other diseases. Thus, an increase in the salivary glands is observed in gland tumors, Mikulicz's disease, malignant lymphomas, sarcoidosis, tuberculosis, actinomycosis, acute bacterial and viral sialadenitis, chronic parenchymal mumps, sialodochitis, hyperlipidemia and diabetes mellitus, as well as in neuroendocrine diseases (dysfunction of the reproductive and thyroid glands ). The use of criteria for diagnosing BS, the absence of signs of an autoimmune disease in these conditions, as well as a biopsy of the minor salivary glands of the lower lip make it possible to exclude BS in the majority of patients with these conditions.
Treatment
The main place in the treatment of BS belongs to corticosteroids and cytostatic immunosuppressants (chlorbutin, cyclophosphamide). In the initial stage of the disease, in the absence of signs of systemic manifestations and moderate abnormalities in laboratory parameters, long-term treatment with prednisolone in small doses (5–10 mg/day) is advisable. In severe and late stages of the disease, in the absence of signs of systemic manifestations, it is necessary to prescribe prednisolone (5–10 mg/day) and chlorobutine (2–4 mg/day), followed by long-term, for several years, maintenance doses of prednisolone (5 mg/day ) and chlorobutine (6–14 mg/week). This regimen can be used to treat patients in the initial stages of the disease in the presence of severe disturbances in laboratory indicators of process activity, as well as cryoglobulinemia without clear signs of systemic manifestations. In the presence of systemic manifestations, regardless of the stage of the disease, hormonal and cytotoxic drugs are used in significantly higher doses, taking into account the severity of systemic manifestations. Pulse therapy with high doses of prednisolone and cyclophosphamide (1000 mg of 6-methylprednisolone intravenously daily for three days in a row and a single intravenous injection of 1000 mg of cyclophosphamide), followed by transfer to moderate doses of prednisolone (30–40 mg/day) and cytostatics (chlorobutin 4- 6 mg/day or cyclophosphamide 200 mg intramuscularly 1–2 times a week) in the absence of hepatotoxic effects is the most effective method of treating patients with severe systemic manifestations of BS, as a rule, it is well tolerated by patients and avoids many complications associated with long-term use of high doses prednisolone and cytostatics. Extracorporeal treatment methods (hemosorption, cryoadsorption, plasmapheresis, double plasma filtration) in combination with pulse therapy are most effective in the treatment of patients with BS with ulcerative-necrotizing vasculitis, glomerulonephritis, polyneuritis, myelopolyradiculoneuritis, cerebrovasculitis, caused by cryoglobulinemia. The experience of previous studies indicates the need to use software, i.e. carried out over a long period of time, extracorporeal therapy
, especially in patients with BS with monoclonal cryoglobulinemia.
Upon achieving a pronounced clinical effect (improvement in general condition, regression of polyserositis, nephritis, polyneuritis, vasculitis, etc.) and a decrease in laboratory indicators of the activity of the process, patients are gradually transferred to maintenance doses of glucocorticosteroids and cytostatics. In parallel, symptomatic therapy is carried out for ophthalmological, dental, gastroenterological and other manifestations of the disease. Local therapy for keratoconjunctivitis sicca
is aimed at overcoming hypolacrimia, preventing secondary infection, accelerating the regeneration processes of the conjunctival and corneal epithelium.
Hypolacrimia is an indication for the use of artificial tears. They replenish the deficiency of the aqueous layer of the precorneal tear film and keep it in a stable position. The frequency of use of drugs depends on the severity of damage to the organ of vision and ranges from 3 to 10 times a day. In many artificial tear compositions, cellulose ethers are used as a polymer ingredient: hydroxylpropylcellulose - lacrisert, lacril, tiarisol, hydroxylcellulose - clerz, lyteers, hydroxymethylcellulose - lacrisin, lacrisify. Other hydrophilic polymers are widely used: polyvinyl alcohol - ligufilm, polyvinylpyrrolidone. In order to preserve residual tear secretion, various methods of blocking the lacrimal ducts are used: cauterization, the introduction of gelatin or adhesive tissue (N-butylcyanocryl) directly into the lacrimal canaliculi, as well as silicone plugs (punctum plug) for permanent tamponade of the lacrimal punctum and creating a physiological block. To protect the cornea, therapeutic soft contact lenses are used. To prevent secondary infection, use solutions of furatsilin (at a dilution of 1:5000), 0.25% solution of chloramphenicol, ciprofloxacin, etc. The use of trypsin, chemotrypsin (2 mg per 10 ml of isotonic sodium chloride solution), fibrinolysin and lecozyme helps to reduce the viscosity of the precorneal layer . In order to influence the regeneration of the epithelium of the cornea and conjunctiva, citral with riboflavin is instilled, and 0.5% thiamine, 10% methyluracil, and solcoseryl ointments are applied overnight. Therapy for chronic sialadenitis
is aimed at overcoming hyposalivation, strengthening the walls of the salivary gland ducts, preventing exacerbations of sialadenitis, improving the regeneration of the epithelium of the oral mucosa and fighting secondary infections.
In order to normalize the trophism and secretion of the salivary glands, novocaine blockades are used. In cases of exacerbation of chronic parotitis (and to prevent its relapses), applications of a 10–30% dimexide solution are used. In cases of the development of purulent parotitis, antibiotics are injected into the ducts of the salivary glands and antifungal drugs (nystatin, levorin, nystatin ointment) are prescribed locally. To reduce the permeability of the ducts, calcium preparations are administered intravenously or intramuscularly. It is possible to accelerate the epithelization of the mucous membrane of the oral cavity and the red border of the lips when erosions and cracks occur with the help of rosehip and sea buckthorn oils, solcoseryl and methyluracil ointments, as well as by treating the oral mucosa with the drug ENKAD (active nucleic acid derivatives). Decamine caramel also has antibacterial properties. For dry nasal mucosa, frequent applications of isotonic sodium chloride solution are used (using turundas). Vaginal dryness is reduced by using potassium iodide jelly. For dry trachea and bronchi, long-term use of bromhexine is recommended (8–16 mg 3 times a day for 2–3 months). If there are symptoms of chronic gastritis with secretory insufficiency, replacement therapy is carried out for a long time (hydrochloric acid, natural gastric juice, pepsidil). Insufficiency of pancreatic secretion requires taking enzymes: Panzinorm, Creon, Festal in courses of 2-3 months or continuously, treatment is also carried out with solcoseryl (2 ml intramuscularly 2 times a day for 15-30 days). The prognosis for life
is favorable.
With timely treatment, it is possible to slow down the progression of the disease and restore the ability of patients to work. With a late start of treatment, severe ophthalmological, dental, and systemic manifestations of the disease usually quickly develop, and the patient becomes disabled. A patient with BS with monoclonal cryoglobulinemia and in cases of the development of malignant lymphoproliferative diseases has a less favorable prognosis. Prevention
is aimed at preventing exacerbations and progression of the disease. It provides for early diagnosis and timely initiation of adequate therapy. Some patients need to limit physical activity and stress on the visual organs, and eliminate allergenic effects. Vaccination is contraindicated for patients; thermal procedures should be used with great caution. Sanitation of the mouth and timely dental prosthetics are necessary.
Literature:
1. V.I. Vasiliev, M.V. Simonova, T.N. Safonova. Sjögren’s disease // Guide to internal medicine “Rheumatic diseases”, under the guidance of. V.A. Nasonova, N.V. Bunchuk. M., “Medicine”, 1997;196–210. 2. International Seminar on SjЪurgren's Syndrome. Editors R. Manthorpe, J. U. Prause. Scand Jorn of Rheum 1986;61:1–291. 3. Sjogren's Syndrome. Clinical and Immunologic Aspects. Editors N. Talal, Moutsopoulos HM, Kassan SS. Springer-Verlag, Berlin-Heidelberg, 1987;1–299. 4. Siogren's Syndrome. State of the art. Kugler Publications. Amsterdam/New York. Editors Homma M., Sugaj S., Tojo T., Miysaka N., Akizuki M. 1994;1–615. 5. Fifth International Symposium on Sjbgren's Syndrome. Fox RI. Arthritis Rheum 1996;39(2):195–6.
Diagnostics
During the consultation, the doctor examines the patient, collects anamnesis, and carefully examines complaints. Diagnostic procedures are then determined, which may include:
- Clinical blood test. Reflects a reduced level of hemoglobin and leukocytes, increases the erythrocyte sedimentation rate.
- Blood chemistry. Shows changes in seroglycoids, gamma globulin, and total fibrin.
- Immunological reactions . Determines an increase in immunoglobulins lgM and lgG, a decrease in the number of T cells.
- Slit lamp examination . Helps identify dry mucous membranes of the eye.
- Schirmer test . Calculates the volume of tear fluid produced by the glands.
- ANA profile . Determines the presence of autoimmune pathologies that occur not only in Sjogren's syndrome, but also in other diseases.
- Sialometry . Calculates the volume of fluid produced by the salivary glands.
- Sialography . Assess the condition of the parotid salivary gland duct using a contrast agent and radiography.
- Lip biopsy. Detects changes in the number of lymphocytes in the salivary glands.
- Ultrasound of the glands. Displays the presence of stones in glandular ducts and hypoechoic areas.
Differential diagnosis allows you to accurately identify the cause of the patient’s poor health.
Forecast
Sjögren's syndrome can damage vital organs with a transition to a stable state, gradual progression, or, conversely, long-term remission. This behavior is also typical for other autoimmune diseases.
- Some patients may have mild symptoms of dry eyes and mouth, while others develop serious complications. Some patients are completely helped by symptomatic treatment, others have to constantly struggle with deterioration of vision, constant discomfort in the eyes, often recurrent infections of the oral cavity, swelling of the parotid salivary gland, difficulty chewing and swallowing. Constant loss of strength and joint pain seriously reduce the quality of life. In some patients, the pathological process involves the kidneys - glomerulonephritis, leading to proteinuria, impaired renal concentrating ability and distal renal tubular acidosis.
- People with Sjögren's syndrome have a higher risk of developing non-Hodgkin's lymphoma compared to healthy people and people with other autoimmune diseases. About 5% of patients develop some form of lymphoma.
In addition, it has been found that children of women with Sjogren's syndrome during pregnancy have a higher risk of developing neonatal lupus erythematosus with congenital heart block.
Treatment
There is no standard treatment for Sjögren's disease, so doctors select supportive and symptomatic treatments. For example, to eliminate dryness of the mucous membrane, medications are selected that protect and moisturize the cornea. These include Gilan, which contains highly purified sodium hyaluronate. It creates a protective film on the surface of the eyes, which protects the mucous membrane from drying out, inflammation or irritation. In some cases, doctors select soft contact lenses.
To reduce inflammation of the lacrimal glands, the doctor prescribes drugs with cyclosporine. You can get rid of dry mouth with the help of medications that stimulate the flow of saliva. To normalize saliva production, medications with calcium are selected, and you need to drink water during meals. Since the syndrome accelerates the development of caries, it is necessary to carry out careful oral hygiene and regularly consult a dentist.
In some cases, pancreatic insufficiency is observed, for the treatment of which medications with enzymes are selected. If gastric secretory insufficiency is present, replacement therapy is used.
If the patient exhibits musculoskeletal symptoms, they are treated with nonsteroidal anti-inflammatory drugs. To stop the inflammatory process in the parotid glands, doctors select antifungal drugs and prepare a course of antibiotics.
In the later stages, there are serious complications that require the use of immunoglobulins, immunosuppressants, and corticosteroids. When glomerulonephritis, ulcerative necrotizing angiitis and other pathologies appear, clinical recommendations include plasmapheresis and hemosorption.
Forms and stages of Sjögren's syndrome
There are subacute and chronic forms of the disease. For subacute, extraglandular symptoms are more typical: rheumatological disorders, vasculitis and corresponding skin lesions, malfunctions of the kidneys and PNS. Chronic is characterized by a predominance of glandular abnormalities: improper functioning of the glands, diseases of the ENT organs.
According to the severity of symptoms, early, severe and late stages are distinguished. Negative changes in connective tissue occur with varying intensity. With a high degree of intensity, symptoms of mumps, stomatitis, conjunctivitis and arthritis are noted. In severe cases, generalized lymphadenopathy (enlarged nodes of the lymphatic system) and hepatosplenomegaly (enlarged spleen and liver) are diagnosed. Based on the results of laboratory tests, a violent inflammatory process is revealed.
Moderate intensity is expressed in a decrease in the immune response, there is extensive destruction of the epithelium of the glands. Low intensity causes xerostomia (saliva deficiency), keratoconjunctivitis (inflammatory damage to the conjunctiva and cornea) and gastritis (inflammation of the stomach lining).
Prevention
There are no specific preventive methods, since the reasons causing the development of the syndrome have not been fully studied. There are general recommendations that can reduce the likelihood of its occurrence. These include:
- Regular preventive examinations with doctors.
- Timely treatment of infections, especially ENT-related.
- Strict adherence to treatment regimens selected by the doctor.
- Elimination of frequent stress and emotional overload.
- Reducing the load on the organs of vision, digestion and speech.
- Refusal of sunbathing and visiting the solarium.
- Vaccination only if prescribed by a doctor.
Sjögren's syndrome occurs in many patients and is accompanied by a number of unpleasant symptoms. Its treatment includes taking drugs that impair the functioning of the immune system. It is possible to maintain a stable condition only with complex therapy selected by a dentist, gastroenterologist, ophthalmologist and rheumatologist. Treatment and prevention are determined only by doctors.
Prognosis and possible complications
Sjögren's syndrome does not pose a serious threat if treated correctly, but its manifestations can complicate a person's life. It is necessary to eliminate symptoms in a timely manner and carry out supportive procedures so that a person does not become disabled due to severe complications. Only through complex treatment can it be possible to slow down the destruction of connective tissue and maintain a person’s ability to work.
Complications and consequences of Sjogren's syndrome:
- secondary infection;
- mumps;
- sinusitis;
- blepharitis;
- bronchitis;
- bronchopneumonia;
- tracheitis;
- diabetes;
- kidney failure;
- thyroid dysfunction;
- circulatory disorders in the brain.