A bone cyst is a limited cavity inside bone tissue filled with blood, serous, serous-hemorrhagic fluid. According to the International Histological Classification of Bone Tumors, a cyst is classified as a tumor-like process. Moreover, among all primary bone formations they occupy 3rd place and most often form in childhood, although the formation of cysts in the bones of adults is not excluded.
A neoplasm of this kind can occur in any of the bones of the skeleton, but the proximal humerus (50%) and femur (25%) are most often affected. Much less often, bone cysts are found in the tibia, fibula, calcaneus, and spine. Initially, they may not appear in any way, but as they grow, pain and other symptoms appear. The cyst disrupts the normal structure of the bone and increases the likelihood of fractures even with light loads. It can also lead to bone deformation, which in severe cases creates pronounced aesthetic defects.
Bone cysts in children
Cystic cavities of various types are one of the most common skeletal pathologies in children. Basically, neoplasms are formed in the zone of increase in bone length, i.e., its metaphysis - an area located near the epiphysis (head) of the bone and formed during the growth of the skeleton due to the division and subsequent ossification of cells of the epiphyseal plates.
After the end of the period of growth and formation of the skeleton, the epiphyseal plates are replaced by the epiphyseal line and ossify.
A bone cyst in children usually forms against the background of the development of a degenerative process, which becomes a consequence of vascular defects. As a result of emerging hemodynamic disorders and disruption of the outflow of interstitial (tissue) fluid in the metaphyseal section of the bones, an increase in intraosseous pressure in a specific area is observed. This causes the formation of a cavity that fills with liquid.
Impaired blood supply to the bone, a decrease in the supply of nutrients and oxygen leads to the activation of the production of specific enzymes that provoke resorption, i.e., bone resorption. This causes a decrease in bone mass. As a result, it becomes less strong and therefore more susceptible to fractures.
Subcortical bone cysts are most often diagnosed in children:
- solitary or simple (SKS);
- aneurysmal (ACC).
A comment
The information presented in the article is fundamentally new; The work is well structured, illustrated and argued. In conclusion, we can once again clarify the details of the separate lesion of the cyst of the odontoid bone and the CII body, indicating the features of the embryogenesis of the cyst. These technical details will improve the perception of the article by the magazine's readers.
The article is undoubtedly of practical interest and can be recommended for publication in a specialized neurosurgical journal.
A.Yu. Mushkin
(Saint Petersburg)
Solitary
SBS is one of the most common pathologies of the childhood skeleton. According to various authors, they account for 21-57% of all benign tumors in children. They are intramedullary, i.e., single-chamber cavities formed inside the bone marrow substance. They are filled with serous fluid and lined with a fibrous membrane of varying thickness, formed by connective tissue and single giant cells.
They can form in any bone, but are more often localized in long tubular bones, especially in the proximal (located closer to the body) metaphysis of the humerus and femur, and somewhat less commonly in the tibia. When the bone reaches a large size, it can “swell”, which leads to the formation of a characteristic swelling.
In 80% of cases, solitary cysts are diagnosed before the age of 20. Moreover, they are observed 3 times more often in boys than in girls. The peak incidence occurs between 10 and 15 years. Only 20% of patients are children under 10 years of age.
Aneurysmal
An aneurysmal bone cyst is a benign tumor-like formation, which, unlike a solitary cyst, has numerous vascular spaces filled with blood. It progresses rapidly and predominantly affects the pelvic bones, vertebrae and knee joint (metaphyses of the femur and tibia), but is less common than solitary.
ACC can be present in children of any age and gender, but most often this bone cyst is diagnosed in adolescents, namely girls 10-20 years old. Among all bone neoplasms, it accounts for 1–9.1%.
For what reasons degenerative bone cysts of this type are formed have not yet been fully studied, but it is also assumed that its formation provokes a local disturbance of venous outflow. Trauma can also cause the formation of an aneurysmal cyst. Less commonly, this bone cyst in children acts as an element in the structure of another tumor.
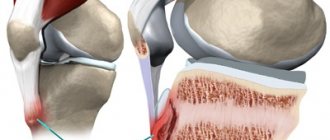
Subchondral cyst
This term refers to multiple small cavities in the articular surfaces of bones, the size of which does not exceed 1.5 cm. Most often, subchondral cysts are found in older people and are a consequence of degenerative diseases of the joints (arthrosis), inflammatory processes in them (arthritis) and other pathological changes . Although, due to the “rejuvenation” of degenerative-dystrophic diseases, today neoplasms of this kind are often found in middle-aged people, especially those engaged in heavy physical labor, in athletes and obese patients leading a sedentary lifestyle.
Most often, subchondral cysts occur in the hip and knee joints.
The manifestations of cysts are similar to the symptoms of arthrosis and arthritis. Therefore, they are usually discovered by chance during a routine examination of the joint to assess the dynamics of the underlying disease. If the patient neglects such procedures, the tumor tends to increase in size and deform the joint. This is accompanied by increased pain during movements, as well as impaired motor activity and even disability. Therefore, it is important not only to treat arthrosis and similar pathologies, but also to regularly undergo scheduled examinations and examinations.
conclusions
Since no single protocol has been developed for the choice of treatment method for children and adolescents with tumors and tumor-like diseases, the course of which was complicated by pathological fractures, each case requires a differentiated approach to treatment and depends on the nature, location of the fracture, as well as the age of the patient and the nosological affiliation of the underlying disease, which must be confirmed morphologically.
Information about authors
For contacts:
Snetkov A.I. — email
Intraosseous ganglion
An intraosseous ganglion or juxtaarticular bone cyst is a non-neoplastic cystic formation that has a fibrous wall and forms in the subchondral areas of the bone, i.e., adjacent to the hyaline cartilage. Often the neoplasm is multilocular.
Thus, it is localized directly in the joint, which leads to the appearance of characteristic symptoms, although more often it occurs hidden. Manifestations of juxtaarticular bone cartilage may include pain in the area of the affected joint that occurs during physical activity, local soreness, and rarely swelling.
The development of the pathology is based on mucoid degeneration of connective tissue, which is not associated with degenerative processes in the joint. The contents of the cyst are represented by mucinous mucous fluid.
The disease is rare, mainly in people 30-50 years old. Its development is associated with microtrauma of the joints and manifestations of local aseptic necrosis. This leads to bone marrow vascular disorders in the subchondral layer of bone. Therefore, the intraosseous ganglion has much in common with subchondral cysts that accompany degenerative-dystrophic pathologies of the joints.
Aseptic necrosis is a chronic non-infectious disease that provokes the systematic destruction of bone tissue of the epiphyses and restriction of movements in the joint. This is accompanied by a gradual flattening of the bone head due to the destruction of the bony partitions of the cancellous bone. The disease is characterized by pain that constantly intensifies and persists even at rest.
Installation of the acetabular cup
A series of X-rays are taken, in which it is important to correctly identify and evaluate the signs of arthrosis, since, for example, different methods of fixing endoprostheses are used for dysplastic and hyperplastic coxarthrosis. Sclerosis and cysts directly influence the choice of arthroplasty technique, in particular the method of cup attachment. It is impossible to integrate the coating of a cementless cup into sclerotic bone that has lost its elasticity.
For a more reliable fixation of the cup, the cavity is cleaned down to the level of the spongy substance, since this tissue is able to effectively participate in the process of osseointegration. Cement fixation is also more stable when placed on a spongy substance. It is important to remove as much sclerotic tissue as possible.
After treating the surface of the acetabulum with special cutters, holes for attaching the cup are drilled to the level of the spongy substance, and all cystic formations are cleaned out. The cavities remaining after curettage are filled with a substance obtained either from the head of the femoral bone or from the bone canal. The cavity is washed, tamponed, and a cup is installed. When planting on cement, the required thickness of the mantle layer under the bowl is taken into account.
If a cup of cementless fixation is installed in the presence of cysts, then after all the stages of cleansing the surface of the cavity from osteophytes and scraping out the cystic cavities, the remaining defects are filled with spongy autologous bone - a substance extracted from the head, as well as remaining during the treatment of the medullary canal. The substance is compacted at the bottom of the depression, strengthening it. If the patient’s own autologous bone is not enough, then a special synthetic hypoallergenic material is used. In order to increase reliability, the bowl is additionally secured with screws.
Minimally invasive endoprosthetics in the Czech Republic: doctors, rehabilitation, terms and prices.
Find out more
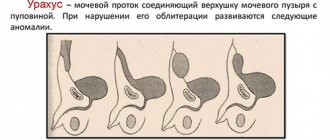
Epidermal inclusion cyst
An inclusion epidermal cyst is a cavity inside the bone, lined with stratified squamous keratinizing epithelium. It is most often a consequence of penetrating trauma, during which epithelial cells enter the bone tissue. This type is more common in the finger bones and skull and may not manifest itself in any way, and pathological fractures are rare.
A comment
The paper presents in detail two clinical cases of bone cysts in the clivus and axis.
Undoubtedly, the work is of scientific and practical interest, especially since the world literature does not describe such clinical observations of bone cysts localized in the area of the base of the skull and the craniovertebral joint.
These are rare, very interesting, from the point of view of clinicians, cases, which makes them very indicative. In addition, we were shown well-executed operations.
I consider it necessary to publish this work in the journal “Problems of Neurosurgery” as it is novel and contains information useful for colleagues.
A.O. Thickness
(Moscow)
Stages of development
In its development, a bone tissue cyst goes through 3 stages:
- Active (osteolysis phase). It lasts about 1 year and is accompanied by an increase in the size of the tumor, the appearance of swelling and other symptoms, and an increased risk of pathological fractures.
- Passive (demarcation phase). Lasts 6-8 months. The cavity gradually decreases in size, mainly due to compaction of the peripheral part of the bone. Symptoms gradually decrease.
- Regenerative (recovery phase). It occurs on average 2 years after the onset of the pathology. There are no symptoms, but there is still an increased risk of fracture because there is a residual cavity or limited area of osteosclerosis (hardening of the bone that reduces its elasticity and resistance to stress).
Symptoms
The clinical manifestations of a bone cyst depend on its location, size, shape and degree of bone destruction. When long tubular bones (humerus, ulna, femur, tibia, fibula) are affected, which is observed in the vast majority of cases, pain occurs. They are bursting, pressing, and arise or intensify during physical activity. With aneurysmal cysts, the pain is more intense and becomes constant over time. This is caused by a progressive increase in size of the cyst, which leads to bone degeneration, thinning of the cortical plate, stretching and thinning of the periosteum.
You may also experience:
- a swelling not fused to the skin in the projection of the cyst, which can be felt (with an aneurysmal cyst it is painful);
- stiffness, decreased range of active movements in the adjacent joint;
- contracture, i.e. incomplete extension or flexion;
- decreased supporting function of the leg, lameness due to the formation of neoplasms in the bones of the lower extremities;
- change in the shape of the limb in the affected area;
- swelling of soft tissues, redness and local increase in temperature;
- slight muscle dystrophy;
- joint deformation (in severe cases in combination with arthrosis);
- neurological disorders (shooting pains, impaired sensitivity and mobility, up to paresis and paralysis, dysfunction of internal organs) with damage to the spine and compression of the spinal roots.
Often the first symptom of a cyst is a fracture obtained in the absence of a serious traumatic factor. As a result, the limb is in a forced position, pronounced swelling of the soft tissues is observed, and compaction is determined. Sometimes the cause of the injury cannot even be determined. In such cases, the cyst becomes an accidental finding on an x-ray that explains the cause of the fracture.
But after a fracture occurs, the pathological cavity inside the bone can completely heal, which makes it possible to initially resort to traditional conservative treatment. In some cases, the fracture does not lead to a cure, and the cyst continues to progress, and sometimes becomes more aggressive.
Pathological fractures of the vertebrae are especially dangerous, which can provoke severe neurological complications.
Discussion
When a pathological fracture occurs, the doctor first of all faces the following questions: how will this complication affect the course of the underlying disease and what treatment tactics should be used in each specific case? Today, there are completely opposite approaches to the treatment of pathological fractures.
According to many authors [6–15], in 7–15% of cases, in patients who have suffered a pathological fracture due to a cyst, self-healing occurs—the closure of the cystic cavity. This is explained by post-traumatic drainage of the cyst cavity through the fracture line, a simultaneous decrease in intraosseous pressure, which can remain low for a long period, especially with significant displacement of bone fragments. J. Farber and R. Stanton [16] presented data on spontaneous resolution of solitary bone cysts in every 4th case of pathological fracture. In this regard, the proposed method of conservative treatment consists of long-term immobilization of the damaged limb and dynamic monitoring of the area of cystic transformation in anticipation of self-healing or reduction in the volume of the pathological cavity. J. Ahn and J. Park [17] conducted a retrospective analysis of the treatment of 52 children with pathological bone fractures due to solitary cysts and found that in the vast majority of cases the cyst persists and sometimes increases. According to the authors of this study [29], out of 42 patients with pathological fractures associated with bone cysts, repair was noted in only 1.
To stabilize and heal pathological fractures, as well as prevent fractures and heal bone cysts in adolescents after puncture biopsy, cannulated screws [18] or intraosseous Eder rods are used to avoid external immobilization [19].
At the same time, N.A. Sholokhova [20], having analyzed the results of treatment of more than 80 patients with bone cysts, came to the conclusion that a pathological fracture against the background of bone cysts does not help reduce intraosseous pressure and close the pathological focus. It is also inappropriate to use metal structures (cannulated screws and rods) in the treatment of bone cysts due to the fact that these techniques do not affect the pathogenesis of the disease.
According to S.T. Zatsepin [2], when treating pathological fractures against the background of giant cell tumors, it is necessary to postpone surgical intervention for 2 weeks from the moment of the fracture, since during a fracture, blood coagulation sharply increases, which will lead to inevitable extensive blood loss during surgery. Method of D. Alkalay et al. [21] involves a two-stage operation: at the first stage, reposition after curettage and minimal internal fixation are performed, at the second stage, repeated curettage, cryotreatment of the cavity, cementation and stable osteosynthesis are performed.
A.V. Ivanov et al. [22], taking into account that chondromas of the phalanges of the hands and feet are often diagnosed with fractures, they suggest immediately using excochleation or resection of the tumor, replacing the defect with auto- or allografts with metal osteosynthesis with miniplates. I.A. Karpenko et al. [23] believe that a two-stage method is most appropriate for treating patients with these pathologies: the first stage is the application of a distraction device for the purpose of repositioning the fracture, the second stage is intralesional resection with bone grafting.
When treating pathological fractures against the background of fibrous dysplasia, most authors give preference to surgical treatment—fracture reposition, removal of the pathological focus, and stable fixation [24]. However, R. Wirbel et al. [25] describe a case of healing of a pathological fracture and osteofibrous dysplasia within 10 months in a 4.5-year-old child after intraosseous osteosynthesis with a titanium rod.
The authors quite rightly highlight possible risks that contribute to the occurrence of pathological fractures and advise the use of metal osteosynthesis of the affected segment in order to prevent them [26].
So, for example, V.M. Shapovalov et al. [27] in the presence or risk of a pathological fracture due to benign tumors, combine bone grafting with stable internal fixation.
At the same time, S.T. Zatsepin [2] in patients with benign lesions, including complicated pathological fractures, after extensive intralesional resection, recommends performing bone grafting with fresh frozen cortical allografts with fixation on the axial graft.
L.M. Kuftyrev et al. [28] give preference to intraosseous resection of the focus of destruction, followed by free autoplasty from the iliac wing and fixation with the Ilizarov apparatus.
Thus, today, issues regarding means of fixation of pathological fractures and methods for replacing post-resection defects remain debatable. There is also no consensus on methods for preventing the occurrence of pathological fractures in patients with benign tumors and tumor-like diseases.
Diagnostics
If signs of a cyst appear, as with fractures, you should contact an orthopedic traumatologist. If the integrity of the bone is maintained, the doctor can palpate to detect a painless lump and perform tests to assess range of motion.
But the main way to diagnose a bone cyst is an x-ray examination. A bone cyst on x-ray looks like a single- or multi-chamber formation, combined with swelling and thinning of the cortical bone layer, and axial deformations. Sometimes abnormally healed pathological bone fractures and joint changes are found. But each type of cyst has its own radiological signs:
· An aneurysmal cyst is distinguished by metaphyseal lesions. Has an eccentric lytic lesion that often extends beyond the normal anatomical boundaries of the bone. There is thinning of the cortex, as well as the presence of a sclerotic “rim” along the periphery, which indicates a periosteal reaction. The neoplasm is septate, i.e. it is multi-chambered and has the appearance of “soap bubbles”.
- On X-ray, a solitary bone cyst looks like a centrally located lytic formation with a clear border. It can expand from the center to the periphery, but never penetrates the cortex and does not extend above the epiphyseal plate. Sometimes bone septa protruding inward are observed. They can create a deceptive multi-camera appearance. But, unlike an aneurysmal cyst, there is no periosteal reaction.
- Subchondral cysts are defined as single or multiple lesions that can mimic a tumor. There is always a narrowing of the joint space and signs of dystrophic changes.
- The intraosseous ganglion (juxtaarticular bone cyst) has the appearance of a clearly demarcated oval or round formation. It is eccentrically located and located subchondral in the epiphysis but not in the metaphysis. Deformation of the periosteum may be observed. The formation is delimited by a sclerotic rim, which is associated with the absence or mild severity of dystrophic changes in the joint.
Additionally, in order to differentiate the cyst from other bone tumors, the patient may be prescribed:
- Ultrasound – indicated for diagnosing degenerative changes in the cartilage tissue of joints;
- CT scan – allows you to detect specific signs (symptom of “horizontal levels”), determine the relative density, area, volume of the tumor, the number of chambers;
- MRI is the best method for diagnosing pathologies of soft tissue structures, used to diagnose joint diseases and in preparation for surgery, as it allows one to assess the location of the neurovascular bundle and avoid its injury during surgery.
If a specialist has doubts about the nature of the neoplasm, he may recommend performing a puncture of the cyst with further study of the obtained material in the laboratory. In particular, this is indicated for differentiating benign aneurysmal cysts from malignant telangiectatic osteosarcoma.
Additionally, a general urine and blood test and a biochemical blood test may be prescribed to assess the general condition of the body, identify signs of inflammatory processes, and exclude certain diseases.
Treatment
Treatment of bone cysts can be done conservatively or surgically. Tactics are always chosen based on the type of neoplasm, its location, stage of development, degree of influence on the functions and structure of the bone. If possible, preference is given to non-surgical treatment, especially in children, since the possibility of damage to the epiphyseal plates that ensure bone growth cannot be ruled out. In such cases, there may be a delay in the growth of a body part in the future.
But in some cases it is impossible to do without surgery. Radical removal of a bone cyst is indicated for:
- threat of development of spinal canal stenosis;
- risk of extensive bone destruction;
- the size of the tumor is more than 2/3 of the cross-section of the bone;
- localization in the loaded area, dangerous proximity to the epiphyseal plate, which creates a high risk of pathological fracture;
- prolonged, severe pain that cannot be eliminated by conservative methods;
- no tendency to shrink the cavity 6-8 months after the start of conservative treatment.
In case of a fracture, a plaster cast or polymer cast is applied to immobilize the limb, since when it heals, there is a possibility of self-healing.
Regardless of the chosen treatment method, control x-rays are taken 2, 6 and 12 months after the start of therapy. This allows you to track the dynamics of changes in the condition of the cyst and, if necessary, adjust treatment tactics.
What are the other methods for bone tumors?
Some bone tumors are sensitive to radiation therapy. Radiation therapy can be used as a stand-alone treatment or in combination with other treatments. Chemotherapy can be used for treatment depending on the biological behavior of the disease. It can be used before or after surgery.
Is there a difference between the sexes regarding the risk of developing this disease?
We can provide information on this issue in the USA. Malignant bone tumors are detected in 2500 cases per year, benign ones - in 200,000-300,000. Bone metastases occur in 250,000 - 300,000 cases per year. There were no differences between the sexes in terms of the risk of bone tumors.
What would you like to say about the follow-up of patients after treatment?
Follow-up of the patient is done initially at short intervals, and the follow-up itself will continue for many years. With this method, recurrence of the disease or its spread to other organs is detected at an early stage and a treatment plan is drawn up. At this stage, the patient needs psychological support and a return to a full social life. Lung, breast, thyroid and prostate cancers are the main causes of metastases, in addition to primary malignant bone tumors. In addition, it is necessary to carefully investigate the causes of bone pain that occurs in old age.
What is amputation?
Amputation is the removal of an affected part of the body in order to save the patient's life if it is impossible to save the organ. For example, if we are talking about the development of a disease in the leg, the leg must be amputated. But we are now far from such a surgical approach thanks to developments in diagnostics and treatment. If in the 80s 90% of patients diagnosed with cancer would have been treated with amputation, now this percentage is less than 10%.
Conservative treatment
The basis of treatment is drug therapy. It includes the use of NSAIDs and puncture of the cyst. NSAIDs have analgesic and anti-inflammatory properties. They are usually prescribed orally; for severe pain, intramuscular administration is possible. Contraindicated for gastrointestinal diseases.
Puncture of the cystic cavity is performed under local anesthesia. It involves inserting a needle into the cyst, through which its contents are aspirated. Perforation of the walls is also performed to reduce pressure. The cavity is washed with saline and then with a 5% solution of aminocaproic acid and an antienzyme drug is administered. For patients over 12 years of age, corticosteroids may be injected into the cyst cavity.
For large cysts in the active phase of osteolysis, punctures can be performed every 3 weeks, after its transition to the stage of demarcation - every 4-5 weeks. But in most cases, 6-10 punctures are enough to close the cyst. If the cyst is located in a hard-to-reach place, the puncture is carried out under CT control.
The liquid obtained during aspiration is sent for histological examination. This makes it possible to accurately determine the nature of the formation and exclude oncology, in particular malignant giant cell tumor.
The advantages of using puncture to treat cysts are undeniable. This minimally invasive procedure:
- allows you to quickly improve your well-being;
- high degree of security;
- quick and easy recovery period;
- no scars.
But in some cases, puncture is only a stage of preparation for open osteoplastic surgery.
Drug therapy is supplemented by courses of physiotherapeutic procedures and exercise therapy. Their main tasks are to maintain joint mobility at the proper level and consolidate the results of drug treatment. If there is a high risk of pathological fracture, patients may be advised to wear orthopedic products, in particular orthoses and braces.
If degenerative bone cysts lead to a fracture, immobilization using a plaster cast, plastic splints or other orthopedic devices is indicated.
What can you say about benign bone tumors and their treatment?
The most common benign bone tumors are non-osteogenic fibroma, simple bone cyst, osteochondroma, giant cell tumor, cartilaginous tumor, and fibrous dysplasia. Since treatment for benign bone tumors depends on the type of tumor and the age of the patient, monitoring the patient is sufficient in most cases. In some cases, drug treatment relieves pain. In some cases, especially in pediatric patients, tumors may disappear spontaneously over time. Some benign tumors can develop into malignant tumors and then metastases may begin to develop. Sometimes the doctor recommends removing the tumor. This approach prevents possible pathological fractures. Some tumors may recur even though they have been excised. Giant cell tumor is the most common benign tumor, which can have an aggressive course of development. In some cases, osteochondroma, which is localized in several areas, can develop into cancer.
BE ATTENTION TO THESE SYMPTOMS!
Specialist in orthopedics and traumatology, Professor Kaan Erler says: “If you experience pain despite being rested or if you suspect a bone tumor, please consult a doctor immediately. Orthopedic oncologists will help you in any situation.”
Surgery for bone cyst
Surgery is a last resort measure for the treatment of bone cysts, used when other methods are ineffective or there is a risk of developing serious complications, for example, the formation of a cystic cavity in the vertebra and compression (squeezing) of the spinal cord or its roots. If there are indications, in most cases local excision of the affected area of the bone is performed, i.e., marginal resection with careful treatment of the bone cavity. The formed defect is filled with the patient’s own bone graft or synthetic material.
When segments of the upper or lower extremities are affected, excochleation of the cyst is sometimes performed, i.e., removal of its contents with a blunt spoon without affecting the walls, followed by filling the resulting defect. For large defects, bone grafting can be performed using DHS and DCS systems, a locking plate, an intramedullary locking rod, screws, and the application of an Ilizarov apparatus.
In case of complex fractures with displacement, open reposition of bone fragments is performed with internal, or less often external, fixation in the correct position.
In some cases, removal of the cyst requires a bone osteotomy. The cut is made in the area between the healthy and changed areas of the bone. After this, intraosseous resection of the formation is performed and a bone graft is installed in the remaining cavity. To restore the integrity of the bone, a distraction regenerate is formed and compression-distraction osteosynthesis according to Ilizarov is performed.
After surgery, relapses practically do not occur.
If subchondral cysts are observed, especially those arising from severe deforming arthrosis or avascular necrosis, which is typical in adults and is accompanied by severe pain, patients may be offered various types of surgical interventions to solve these problems. Basically, today in such cases endoprosthetics of the affected joint is used, which involves replacing destroyed bone fragments with artificial prostheses. In terms of functionality, they are practically not inferior to a natural joint, and their service life is on average 20 years.
How is bone cancer treated?
Treatment of bone tumors is always the result of teamwork. The main members of this team are an orthopedic oncologist, an oncologist, a radiologist, a radiation oncologist, and a pathologist. The goal of treatment is to overcome the cancer and protect the affected limbs. Are there improvements in the treatment of bone tumors as medicine advances? Are there changes in surgical techniques? Previously, in order to remove a tumor from the body, there was mainly a method of amputation of limbs. But a surgical approach is now available that can both remove the tumor and protect the limbs. Surgery can be performed by removing the center of the tumor or removing it along with a small area of healthy skin. The goal of treatment is to ensure the functioning of the limb after cancer therapy. This is facilitated, in particular, by the development of reconstructive surgery. Also often used are prosthetics, bone grafts, which are pieces of bone taken from other parts of the skeleton, used to heal the affected area, and biological reconstruction techniques.
Rehabilitation
After surgical removal of a bone cyst, the body needs to create favorable conditions for recovery. For this purpose, a rehabilitation program is being developed. But its duration and nature are determined by the type of operation performed, its volume and degree of complexity.
All patients, without exception, are prescribed antibacterial therapy, designed to reduce the risk of developing postoperative inflammatory processes. In parallel, antifungal drugs and probiotics are prescribed to reduce the risk of adverse events after taking antibiotics.
Taking NSAIDs is also indicated to reduce the severity of pain. Exercise therapy is mandatory, designed to eliminate the risk of developing muscle atrophy, improve blood circulation and restore normal range of motion in the joints. The physical therapy program, the nature of the exercises, and the number of repetitions are selected strictly individually for each patient in accordance with the type of surgery performed, the general level of physical fitness and the nature of existing chronic diseases.
The prognosis for bone cysts is favorable. With timely and adequate treatment after closure of the cavity, complete recovery usually occurs, and the patient’s quality of life does not decrease.
Thus, bone cysts are far from uncommon, especially among children. However, adults are not protected from this disease. Moreover, under the guise of harmlessness and the absence of clinical manifestations, such benign neoplasms can lead to complex pathological fractures that deform the limbs and provoke the development of various kinds of complications. Therefore, if a cyst is accidentally discovered or its symptoms appear, you should contact an orthopedic traumatologist. Only a doctor can correctly assess the condition of the bone and choose the optimal treatment for the current situation. However, you should not be afraid of surgery. Treatment usually begins with conservative methods, which in most cases allow for recovery. Surgery is indicated only if they are ineffective or there is a high probability of complications. And modern surgical techniques ensure minimal intra- and postoperative risks, rapid recovery and complete recovery.
results
The results of treatment were monitored over a period of 1 to 9 years. The effectiveness of treatment was assessed taking into account oncological and orthopedic criteria. The effectiveness criteria were the absence of complaints, relapse of the disease, signs of consolidation of the pathological fracture, and function of the operated limb.
All patients underwent safe osteoplastic surgery, only in 1 case no surgical treatment was performed, since repair of the pathological focus was recorded after healing of the fracture against the background of the cyst. The period of immobilization in a plaster cast was 6 weeks. In situations with other patients, surgical treatment was necessary. Considering the absence of displacement or the presence of slight displacement of bone fragments and the nosological affiliation of the underlying disease, fixation with plaster casts in 21 cases was the first stage of treatment. Fixation mainly lasted 1 month from the moment of injury, thereby consolidating the fracture, which ensured the creation of more favorable conditions for surgical treatment. In case of significant displacement, the first stage was trephine biopsy to verify the diagnosis and closed reposition to eliminate gross displacement. After which the affected limb was fixed with a plaster cast or a skeletal traction system was applied. After morphological verification of the diagnosis, patients underwent open reduction of the fracture, removal of pathological tissue, alloplasty and, if necessary, metal osteosynthesis. Patients operated on without metal osteosynthesis were treated with unloading and fixation of the affected limb with a plaster cast for 3 months from the date of surgery. Next, the plaster cast was removed and the development of movements in the joints of the operated limb began. Full weight-bearing was recommended 4 months after surgery. The use of bone osteosynthesis made it possible to abandon the use of external immobilization and begin early activation of the patient, to begin early development of movements in the joints of the operated limb, which in turn helped to reduce the length of hospital treatment and facilitate patient care.
In the presence of a metal fixator, the development of movements in the joints of the affected limb began 1 week after the operation, and full load - after 1 month. In the postoperative period, dynamic observation of all patients who received surgical treatment in the department was carried out. Control radiographs were taken 3, 6, 9 and 12 months after surgery. Consolidation of fractures was observed 2.5–3 months after surgery. The timing of non-organotypic reconstruction of grafts depended on a number of factors: the volume of the post-resection defect, the number, type and type of grafts and nosology of the disease. Autografts were reconstructed most quickly in a period of 8 to 12 months. With the isolated use of Perfoost grafts, the period of reconstruction took on average from 12 to 14 months. In cases of massive alloplasty with extensive bone resections, when superficially demineralized allo-implants were combined with cortical frozen implants, the reconstruction period increased to 18 months.
The timing of removal of metal structures depended on the nosology of the pathological process. In fibrous and osteofibrous dysplasia, taking into account the nature of the disease, metal structures were left in place to prevent the occurrence of deformities and pathological fractures in the long-term postoperative period. In other cases, the metal structures were removed 1.5–2 years after the operation.
The following complications were recorded between 3 and 6 months. In case of bone cysts: in 5 cases - relapse of the underlying disease, in 2 - shortening of the damaged segment, 1 case each - joint contractures and neurological disorders; with fibrous dysplasia: in 1 patient - shortening of the damaged segment; with non-osteogenic fibroma: 2 – joint contractures. In the long-term postoperative period (9–18 months) with fibrous dysplasia, migration of metal structures was noted in 2 cases.