Sarcomas are a heterogeneous group of malignant neoplasms that grow from connective tissue, which is different from cancers, which are malignant tumors that develop from epithelial tissues. Soft tissue sarcomas can arise from any extraskeletal nonepithelial tissue except glia and tissues of the reticuloendothelial system. They most often have an aggressive course and are prone to recurrence, even after radical treatment.
Soft tissue sarcoma is a rare pathology. In Russia, the incidence in 2021 was 1.75 per 100,000 people. Most often, these neoplasms affect the lower extremities; this localization accounts for about 40% of cases. Sarcomas of internal organs are rare and are localized in the kidneys, heart, uterus and prostate. Breast sarcoma is considered separately, in which the average age of patients is about 50 years.
- Classification of soft tissue sarcomas
- Etiology and pathogenesis of soft tissue sarcomas
- Clinical symptoms of soft tissue sarcoma
- Diagnosis of sarcoma
- General principles of treatment of soft tissue sarcomas
How does sarcoma develop?
Is sarcoma cancer?
Official medicine in Russia and some other countries refers to cancer as malignant tumors that develop in epithelial cells contained in the skin or mucous membranes and lining the inner surface of organs. Sarcomas are not tied to specific organs, they form in different types of tissues, but behave in a similar way - they grow quickly, damage healthy cells and metastasize. Metastasis is an additional focus of cancer - a new tumor in an organ located far from the main tumor, including in lungs, bones and liver.
The disease begins with the appearance of just one mutated or altered cell. It becomes this way under the influence of radiation, various chemicals, diseases or hereditary characteristics, and gradually multiplies, creating copies of itself. Over time, they become more and more numerous, they turn into a tumor and destroy surrounding tissues. In addition, they have a special, very dangerous property - they know how to move around the body using the circulatory and lymphatic systems. The lymphatic system complements the cardiovascular system. The lymph circulating in it - the intercellular fluid - washes all the cells of the body and delivers the necessary substances to them, taking waste from them. In the lymph nodes, which act as “filters,” dangerous substances are neutralized and removed from the body, become established in other areas of the body and create additional tumors.
How not to miss a dangerous disease
During an ultrasound, a tumor can be detected long before symptoms appear. The doctor who has identified the tumor formation will determine the number of nodes, their consistency and location. Although uterine sarcoma does not have strictly defined acoustic signs, an experienced doctor will be alerted by the unclear contour of the formation, its lobular structure and irregular shape.
Since a malignant tumor grows quickly, the blood vessels cannot keep up with its growth. The neoplasm tissues are no longer supplied with blood and nutrients, which leads to necrosis and decay. Inside the sarcoma, a focus appears with liquid contents, which on ultrasound have a darker color, like the surrounding tissue. Such formations are called hypoechoic.
The uterus, affected by a tumor, is deformed, sometimes taking an incorrect position. When metastasizing to the ovaries, tumor areas are visible in them.
An additional method for detecting uterine sarcomas is an ultrasound examination with Doppler, which allows one to assess the condition of the vascular network. Inside the sarcoma, many thin or too wide blood vessels of irregular, convoluted shape are found. Because the vasculature is defective, blood flow has low resistance and blood moves quickly and chaotically. Myomas and fibroids of the uterus, with which sarcomas are often confused, grow much more slowly, so they have time to grow into full-fledged vessels.
If the doctor still has doubts, the patient is scheduled for a repeat examination. Sarcoma grows quickly, so the doctor will immediately detect an enlarged node.
Another sign of concern is a benign tumor that does not change size for a long time and suddenly begins to actively grow. Therefore, in the presence of any formations, it is necessary to periodically undergo an ultrasound scan so as not to miss their degeneration into oncopathology.
Since sarcoma often appears after instrumental abortions, diagnostic curettages, operations and difficult childbirth, women after them need to periodically undergo ultrasound to not miss the development of the tumor. The same examination is recommended for patients suffering from hormonal pathologies and those who have crossed the 40-year mark. These categories need to undergo an ultrasound of the uterus once a year or even more often.
Uterine sarcoma is also diagnosed in completely healthy young women. They are detected even in virgins and very young girls. Therefore, it is recommended for everyone to undergo an ultrasound once every year or two.
Types of soft tissue sarcomas
Doctors know of more than 50 different types of such tumors, the most common of which are:
- Fibrosarcomas
affecting the connective tissue of the legs, arms or torso. They most often occur in people between 20 and 60 years of age, but can even occur in infants. - Angiosarcomas
are hemangiosarcomas that begin in blood vessels, or lymphangiosarcomas that begin in lymphatic vessels. They appear, among other things, in those parts of the body that have been exposed to radiation therapy, in the chest area and in the extremities with lymphedema - an accumulation of lymphatic fluid in the tissues. Lymph is an intercellular fluid that washes all the cells of the body and delivers necessary substances to them, taking away waste . due to disruption of its outflow. - Leiomyosarcoma -
originating in smooth muscle, is often found in the abdominal cavity, but can also be found in other parts of the body, such as the extremities or the uterus. - Synovial
- Forms in the tissues surrounding the joint, usually in the hip, knee, ankle and shoulder. - fibromyxoid
sarcomas are slow-growing tumors usually found in young and middle-aged patients. - Kaposi's sarcoma -
develops in the cells lining lymphatic or blood vessels. - Alveolar cancer
is a rare type of oncology, mainly affecting young patients. - Neurofibrosarcomas, malignant schwannomas and neurogenic sarcomas
arise in cells surrounding the nerve. - Liposarcomas are
tumors of adipose tissue that most often form in people aged 50 to 65 years. - Clear cell -
usually develops in the tendons of the arms or legs. - Rhabdomyosarcomas
are the most common type of soft tissue sarcoma in children. - Epithelioid
- usually damage the tissue of the hands, forearms, feet or legs of adolescents and young patients.
Gastrointestinal stromal tumors- Low-grade myxofibrosarcomas are most often found on the extremities of older people.
- Malignant mesenchymomas -
have features of fibrosarcoma and at least two other types of sarcomas.
Reasons for the development of sarcoma
Doctors do not know the exact causes of such tumors - modern medicine only knows about factors that increase the likelihood of this event.
Radiation
, used to combat various types of oncology. Sarcomas can occur in parts of the body that have been exposed to radiation therapy. On average, about 10 years pass from the time it is carried out until the disease is detected. Treatment methods have been improved over several decades, and much more is known about choosing the right doses than before. Modern knowledge is helping to reduce the number of new diagnoses, but even today radiation is only used when its benefits outweigh the risks.
Heredity
. Some disorders caused by changes in genes are often inherited from parents and are associated with an increased likelihood of developing soft tissue sarcomas. These include:
- Gardner's syndrome
, leading to the appearance of a large number of polyps - growths of intestinal tissue; - neurofibromatosis
, which causes the formation of multiple nerve tumors; - Li-Fraumeni syndrome
, which increases the risk of breast cancer, brain tumors, sarcomas and leukemia - changes in bone marrow and blood cells; - retinoblastoma
is a life-threatening eye tumor that develops mainly in children; - Werner's syndrome
is a genetic disease, the owners of which age prematurely, suffer from cataracts - clouding of the lens, blockage of the heart arteries and other health problems; - tuberous sclerosis
, which causes seizures and a variety of tumors in various tissues and organs, including the brain, eyes, skin, heart, kidneys, liver, lungs and gastrointestinal tract; - Gorlin syndrome
, which increases the likelihood of developing many types of skin cancer, fibrosarcomasFibrosarcomas affect the connective tissue of the legs, arms or torso. They most often occur in people between 20 and 60 years of age, but can even occur in infants. and rhabdomyosarcomasRhabdomyosarcomas are the most common type of soft tissue sarcoma in children.
Chemicals
, such as arsenic and vinyl chloride, used in the production of plastics, increase the risk of liver sarcoma.
Damage to the lymphatic system
. Lymph is a clear liquid containing cells of the immune system, which are transported throughout the body through blood vessels and lymph nodes, which act as “filters” that retain and neutralize dangerous substances. If these important organs are damaged or after their removal, a person may develop lymphedema - accumulation of lymph and swelling, as well as its complication - lymphangiosarcoma. Lymphangiosarcoma is a life-threatening tumor that develops in the lymphatic vessels.
Injuries, lifestyle and bad habits, including smoking, poor diet and lack of exercise, do not increase the likelihood of developing sarcoma.
Chapter 12.
Osteogenic sarcoma is the most common primary bone tumor in children and ranks 6th in frequency among all malignant tumors of childhood. The tumor originates from primitive bone-forming mesenchyme and is characterized by the production of osteoid during malignant proliferation of spindle cell stroma. The peak incidence occurs in the 2nd decade of life. In boys, the incidence of the disease is higher, while at an earlier age girls are predominantly affected (who have a greater bone age during this period than boys).
Etiology
Tumor development has some connection with rapid bone growth. Children with osteosarcoma tend to be taller than normal for their age, and the disease affects the fastest growing parts of the skeleton.
The development of bone tumors is often associated with trauma, but rather trauma attracts the doctor's attention and prompts an x-ray examination
The only environmental agent known to stimulate bone sarcomas is ionizing radiation. Moreover, the interval between exposure to this factor and the occurrence of osteosarcoma can be from 4 to 40 years (on average 12 - 16 years).
Among those suffering from Paget's disease, 2% develop osteosarcoma, often with multiple bone lesions.
The presence of benign bone tumors (osteochondroma, enchondroma, etc.) increases the risk of osteosarcoma.
Among patients cured of retinoblastoma, 50% of secondary tumors are osteosarcoma (retinoblastoma is a tumor that is often hereditary), and both diseases have the same changes in the 13th pair of chromosomes.
An important role in the pathogenesis of osteogenic sarcoma is played by the mutation of the tumor suppressor gene P-53. In some cases, the development of the tumor is also influenced by the inactivation of other tumor-suppressing genes - RBL (retinoblastoma-suppressing gene - which confirms a certain connection between these diseases), the DCC gene isolated from colon carcinoma cells (it is assumed that this gene is localized in the long arm of chromosome 18, which is often absent in human osteosarcoma cells).
Currently, the attention of researchers is drawn to the study of the activity of the MDR gene, which determines resistance to drug therapy, which is associated with P-glycoproteins secreted by osteosarcoma cells. These proteins provide protection to the tumor cell, reducing its accumulation of chemotherapy drugs.
Diagnosis.
The diagnosis of osteosarcoma is based on histopathological criteria in conjunction with radiological findings. Standard histological types of osteosarcoma are osteoblastic (50%), chondroblastic (25%) and fibroblastic - less than 20%
Rare variants of osteosarcoma.
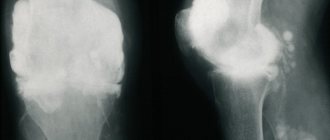
Telangiectatic - radiologically resembles an aneurysmal bone cyst and giant cell tumor, manifested by the presence of lytic foci with mild sclerosis (Fig. 12-1). The course of the disease and response to chemotherapy are practically no different from standard variants of osteosarcoma.
Juxtacortical (paraosseous) - comes from the cortical layer of the bone; tumor tissue can surround the bone on all sides, but, as a rule, does not penetrate the medullary canal. There is no soft tissue component, so radiologically the tumor is difficult to distinguish from osteoid. As a rule, this tumor is of low malignancy, progresses slowly, and almost does not metastasize. However, paraosseous osteosarcoma requires adequate surgical treatment, almost the same as standard tumor variants. Otherwise, this tumor recurs and the tumor component changes to a higher degree of malignancy, which determines the prognosis of the disease.
Periossal - just like paraosseous, it is located on the surface of the bone and has a similar course. The tumor has a soft tissue component, but does not penetrate the medullary canal.
Intraosseous tumors with a low degree of malignancy, well differentiated, with minimal cellular atypia, can be regarded as a benign tumor. But they also tend to recur locally with a change in the tumor component to a more malignant variant.
Multifocal - manifests itself in the form of multiple foci in the bones, similar to each other. It is not entirely clear whether they appear immediately, or whether rapid metastasis occurs from one focus. The prognosis of the disease is fatal.
Extraskeletal osteosarcoma is a rare malignant tumor characterized by the production of osteoid or bone tissue, sometimes together with cartilage tissue, in soft tissues, most often of the lower extremities. But there are also lesions in other areas, such as the larynx, kidneys, esophagus, intestines, liver, heart, bladder, etc. The prognosis of the disease remains poor, and the sensitivity to chemotherapy is very low. The diagnosis of extraskeletal osteosarcoma can be established only after excluding the presence of bone tumor foci.
Small cell osteosarcoma is a highly malignant tumor; its morphological structure differs from other variants, which determines its name. Most often this tumor is localized in the femur. Small cell osteosarcoma (differential diagnosis with other small cell tumors) necessarily produces osteoid.
Osteosarcoma of the pelvis - despite improved overall survival, osteosarcoma has a very poor prognosis. The tumor is characterized by rapid and wide spread in and along the tissues, since, due to the anatomical structure of the pelvis, it does not encounter significant fascial and anatomical barriers on its way.
Staging (Enneking WF, Spanier SS, Goodman MA, 1980, USA)
Stage IA - Well differentiated tumor. The lesion is limited by a natural barrier that prevents the spread of the tumor. No metastases
Stage IB - Well differentiated tumor. The outbreak extends beyond the natural barrier. No metastases
Stage IIA - Poorly differentiated tumor. The outbreak is limited by a natural barrier. No metastases.
Stage IIB - Poorly differentiated tumor. The outbreak extends beyond the natural barrier. No metastases.
Stage III - Presence of regional and distant metastases, regardless of the degree of tumor differentiation
Clinic
The main clinical sign of osteosarcoma is pain over the affected area. The pain is dull, constant with a gradual increase in intensity. A characteristic symptom is night pain. In 3/4 of patients a soft tissue component may be present. The limb is enlarged and often looks swollen. Pain and increased volume lead to dysfunction. The duration of the anamnesis is on average 3 months.
Damage to the metaphyses of long tubular bones is typical. The most common location (approximately 50% of cases) is the knee joint - the distal part of the femur and the proximal part of the tibia. The proximal humerus and femur and the middle third of the femur are also often affected. Damage to flat bones, especially the pelvis, occurs in less than 10% of cases in childhood (Fig. 12-2).
Osteosarcoma has a huge tendency to develop hematogenous metastases. By the time of diagnosis, 10%-20% of patients already have macrometastases in the lungs, detected by X-ray. But by the time the diagnosis is made, about 80% of patients have micrometastases in the lungs, which are not detected x-ray, but are visible on computed tomography. Since bones do not have a developed lymphatic system, early spread of osteosarcoma to regional lymph nodes is rare, but if it occurs, it is a poor prognostic sign. Other areas of metastasis are bones, pleura, pericardium, kidneys, central nervous system.
Osteosarcoma also has local aggressive growth, can spread to the epiphysis and the adjacent joint (most often the knee and shoulder joints are affected), spreading along intra-articular structures, through articular cartilage, through the pericapsular space, or, directly, due to a pathological fracture, and forming non-adjacent its satellite foci are “skip” metastases.
Page 195
Diagnostics
1. Complete x-ray examination. This study allows one to suspect the presence of osteosarcoma in a patient, and also reveals the presence of a soft tissue component, a pathological fracture, determines the size of the tumor, and the optimal level of biopsy.
X-ray signs of osteosarcoma (Fig. 12-3): -metaphyseal localization in long tubular bones; -presence of sclerotic and lytic foci in the bone, presence of vascularization; - foci of pathological osteoformation in soft tissues; -violation of the integrity of the periosteum with the formation of a “visor” or “Codman’s triangle”; - needle periostitis - “spicules” (growth of the periosteum in the form of needles located perpendicular to the surface of the bone); - X-ray of the lungs allows you to detect macrometastases (Fig. 12-4).
But many radiological findings can be misleading: -well-differentiated tumor; -lytic lesions or lesions with minimal sclerosis; -limitation of the focus to the bone marrow canal; - atypical periosteal reaction; -rare intraosseous localization; -rare skeletal localization (soft tissue, skull, rib, etc.).
2. Morphological examination of the tumor. One of the common reasons for the impossibility of performing organ-preserving surgery is an unsuccessful biopsy with local contamination with tumor cells and the development of a pathological fracture. Therefore, the biopsy should be performed by a surgeon and it is preferable to perform a trephine biopsy rather than a knife biopsy (to maximize the protection of tissue adjacent to the tumor from contact with the biopsy).
3. Bone scintigraphy (OSG) with Te-99 can detect other lesions in the bones, although the increase in the accumulation of the isotope is not specific. When performing OSG over time, based on changes in the percentage of isotope accumulation in the lesion before and after chemotherapy, one can fairly accurately judge the effectiveness of chemotherapy. A significant decrease in the percentage of isotope accumulation in the lesion correlates quite accurately with a good histological response of the tumor to chemotherapy.
4. Computed tomography (CT) of the lesion - allows you to identify the exact location of the tumor, its size, the relationship of the tumor to the surrounding tissues, and its spread to the joint. CT scan of the lungs can detect micrometastases that are not detected radiographically.
5. Magnetic resonance imaging (MRI). The most accurate method of contrasting a tumor, revealing its relationship to surrounding tissues, the neurovascular bundle, and also allowing one to determine the dynamics of the process during chemotherapy, its effectiveness and, accordingly, plan the extent of the operation. Currently, MRI is performed with contrast containing gadolinium, which accumulates along the periphery of the tumor, clearly delimiting it (Fig. 12-5).
The largest oncology clinics in the world use an improved method - DEMRI - dynamic capture of a contrast agent, determined by MRI. Using a computer, a quantitative determination (in%) of tumor cells accumulating contrast before and after chemotherapy is made, thereby determining the histological response of the tumor to treatment even in the preoperative period.
6. Angiography - performed before surgery. This method reveals whether the vessels are free or not from the tumor, which determines the extent of the operation. If there are tumor emboli in the vessels, organ-preserving surgery is impossible.
Prognosis factors (according to COSS-77-91 studies)
1. Determination of the volume of the tumor mass. Done before the start of treatment. For ellipsoidal tumors: length x width x thickness x 0.52 For discrete type tumors: length x width x thickness x 0.785
Patients are divided into groups depending on the volume of the tumor mass: group 1 - 70 ml or less - favorable. Group 2 - 71 - 150 ml - intermediate. Group 3 - more than 150 ml - high risk.
When the tumor volume is more than 200 ml, half of the patients develop secondary metastases.
2. Histological response of the tumor to chemotherapy. This indicator is expressed as the percentage of living tumor cells in all tumor tissue that is removed during surgery after preoperative chemotherapy (CT). The histological response of the tumor to chemotherapy determines the prognosis of the disease and the tactics of further treatment. Depending on the number of living tumor cells, 6 degrees of histological response are determined (Grad.n.Salzer-Kuntschik, Wien): I - complete absence of viable tumor cells; II - single live tumor cells or an area with live tumor cells III-IV - 10% - 50% of live tumor cells; V - >50% living tumor cells; VI - no response to chemotherapy.
Auxiliary prognostic factors: - level of alkaline phosphatase (high levels worsen the prognosis of the disease) - localization of the tumor (central localization and proximal thigh are the most unfavorable localizations).
Distribution of patients into risk groups (depending on them, the degree of treatment intensity is determined) - (COSS-96).
The low-risk group includes patients with a tumor volume of 70 ml or less, regardless of the degree of histological response of the tumor to chemotherapy (survival rate in this group with adequate treatment is 97%).
High-risk group - with a tumor volume of more than 150 ml with grades 5 and 6 histological response (survival rate with standard treatment is 17%).
Standard risk - all others (survival rate - 67%)
Each risk group requires specific therapy—longer and more intense for high-risk patients, and less intense for low-risk groups.
Treatment
Until recently, treatment for osteosarcoma was limited to surgery (in particular, limb amputation). But despite this, the survival rate was extremely low - 15%-20%. Significant progress in treatment has been achieved in the last two decades as a result of the development of adjuvant chemotherapy, as well as technical diagnostic tools.
The most important components of the treatment of osteosarcoma.
1. Preoperative chemotherapy is always the first stage of treatment and provides certain advantages: -improvement of systemic tumor control - suppression of micrometastases in the lungs; -improved control of the primary lesion, which expands the possibilities of reconstructive operations on the extremities; - the ability to objectively assess the histological response of the tumor to chemotherapy, which often determines the prognosis of the disease and the tactics of further treatment.
Modern osteosarcoma treatment programs use the following drugs: high-dose methotrexate (8-12 g/m2), adriblastine, ifosfamide, platinum drugs (carboplatin, cisplatin), etoposide.
2. Surgery is the second mandatory stage of treatment. The development of the capabilities of modern surgery, as well as means of controlling the primary tumor focus, makes it possible to improve the quality of life of patients using organ-preserving operations. The implantation of joint endoprosthesis, as well as the replacement of the resected bone area with auto- and allograft, has become widespread throughout the world. However, organ-preserving operations are not always possible for certain reasons: - tumor damage to the neurovascular bundle; -pathological fracture (currently not an absolute contraindication to limb salvage); -incorrectly chosen location for biopsy; - infection of the biopsy site; - the patient’s age is too young (since there is a large reserve for limb growth); but for the upper limbs this does not matter; -previous operations with soft tissue contamination; - large tumor sizes with significant involvement of soft tissues in the process.
The presence of metastases with modern treatment is not a contraindication to organ-conserving surgery.
If organ-preserving surgery is not possible, amputation is performed followed by prosthetic limb replacement. Amputation with modern prosthetics leaves great opportunities for leading an active lifestyle and even playing sports.
3. Postoperative chemotherapy - carried out taking into account the histological response of the tumor to chemotherapy (continuation of treatment, or change of therapy regimen, or cessation of therapy).
The issue of radiotherapy is discussed in the domestic literature. However, in most of the largest foreign clinics this issue is not resolved in favor of this method of treatment. As an example, we will cite 20 years of experience in conducting preoperative radiation therapy followed by surgery at the St. Petersburg Children's Clinic. Jude (Memphis, USA): 84 patients received preoperative RT, 61 received no RT. 5-year survival (without chemotherapy) was less than 20% in both groups of patients.
Currently, the development of metastases does not predict the fatal outcome of the disease. The level of modern thoracic surgery makes it possible to remove a large number of metastases by performing subsegmental resection. In this case, preoperative chemotherapy is also used to determine the histological response of the tumor to treatment. Carboplatin and etoposide are used as 2nd line chemotherapy drugs. The use of these drugs and radical removal of metastases can achieve 5-year survival in 55% of patients with secondary pulmonary metastases (COSS-96).
If standard chemotherapy is ineffective, high-dose chemotherapy using a colony-stimulating factor and peripheral stem cell transplantation is used
Attempts are currently being made to use drugs other than chemotherapy:
Liposomal muramyl tripeptide is a synthesized lipophilic analogue of muramyl dipeptide. It is encapsulated on liposomes and has a selective affinity for pulmonary macrophages and circulating monocytes, activating them and giving them tumoricidal properties
Verapamil and cyclosporine A - according to a number of researchers, reduce the expression of P-glycoprotein in the tumor, thereby improving the absorption of chemotherapy drugs by tumor cells. A good effect was noted when using these drugs together with ifosfamide and etoposide in common forms of osteogenic sarcoma.
Page 196
Signs and symptoms of soft tissue sarcoma
About half of them occur in the arms or legs. Most people notice a swelling that gradually enlarges over weeks or months without always being painful.
About 4 out of 10 sarcomas develop in the abdominal cavity - the abdomen, which causes not only discomfort, but also blockage of the digestive tract or bleeding from the stomach and intestines. In addition, they can put pressure on nerves, blood vessels and nearby organs, and can grow to very large sizes.
In rare cases, tumors appear in the chest, head or neck.
Possible signs of the disease include:
- the appearance of a new swelling or lump in any area of the body and the growth of existing ones;
- increasing abdominal pain;
- blood in the stool or vomit, as this may be caused by damage to the digestive tract from a growing tumor;
- black, tarry stools that acquire a similar color and consistency due to bleeding in the stomach or intestines.
Most often, the above symptoms are not caused by sarcomas, but if they appear, you should immediately consult a doctor.
What parents need to pay attention to
Early symptoms:
Pain
The first significant symptom is increasing pain in the affected limb. After some time, the pain becomes unbearable, depriving sleep, it can appear both during exercise and at rest and is not relieved by conventional analgesics.
Swelling
The affected part of the bone increases in volume, the soft tissues above it become swollen, and phlebectasias (a network of small dilated veins) appear on the skin.
Impaired function of the affected limb. Restricted mobility in a nearby joint
When osteogenic sarcoma is localized in the bones of the lower extremities, movements in the joints become difficult, and lameness develops over time. A late symptom of this disease may include a pathological fracture in the area of the primary lesion.
The main problem of late diagnosis of osteogenic sarcoma is due to the fact that for a long time local pain is associated with a previous injury to the limb. But at the same time, the severity and duration of pain symptoms are not compared with the extent of the injury.
Unfortunately, pain in the extremities in children and adolescents often goes unnoticed or underestimated and is associated primarily with “growing pains,” as a result of which the child receives long-term analgesic therapy without effect.
The duration of the pain syndrome, its pronounced nature, not correlated with previous traumatic changes, is always a reason for an expanded diagnostic search.
Diagnosis of soft tissue sarcoma
Detailed information about the disease and the general state of a person’s health allows us to choose the most appropriate treatment for each individual patient.
Highly qualified oncology specialists carry out a complete diagnosis of soft tissue sarcomas using the most modern equipment - quickly, efficiently, without queues and loss of time.
The examination begins with a general examination and a survey about symptoms and family diseases, after which the doctor prescribes a series of tests.
The first of these may be conventional radiography.
. With its help, immediately after diagnosis, doctors can see whether the tumor has spread to the lungs.
– computed tomography: X-rays create detailed images of internal organs and tissues. The method is used to detect tumors in the chest or abdominal cavity, as well as to detect damage to the lungs, liver and other organs.
MRI
– Magnetic resonance imaging: radio waves and strong magnets often work better than CT scans. MRI can provide information about the size of the sarcoma, its location, and sometimes even the type of tissue it consists of. In addition, this study is prescribed to study the condition of the brain and spinal cord.
Ultrasound
Using ultrasound waves, a specialist can distinguish seals from ordinary cysts - fluid-filled sacs.
PAT
– positron emission tomography: before performing this study, the patient receives radioactive sugar, which accumulates in dangerous tumors. A scan is then performed to show whether changes in the tissue are cancerous.
If a soft tissue sarcoma is suspected, the doctor prescribes a biopsy
, during which a small piece of the tumor is removed and sent to a laboratory where its cells are carefully studied.
Basic diagnostic methods
First of all, you need to see a therapist. The doctor conducts a visual examination and, if necessary, sends you for additional examination to an oncologist, endocrinologist or other specialists. To make an accurate diagnosis, the following examination is indicated:
- blood test - general, biochemical;
- urine test - general;
- x-ray of affected areas and joints;
- Ultrasound of the affected areas, as well as lymph nodes and the abdominal cavity;
- MRI;
- scintigraphy (special examination of bones);
- biopsy - collection of biological tissue directly from the site of the lesion for further analysis.
Stages of soft tissue sarcoma
Immediately after the disease is detected, doctors try to stage it - to understand how far it has spread throughout the body and damaged tissue. This information allows us to understand the patient’s approximate prognosis and select the most appropriate treatment methods for him.
Staging of soft tissue sarcomas is carried out according to the international TNM
, each letter of which has its own meaning:
- " T
" describes the size of the underlying neoplasm; - “ N
” – damage to nearby lymph nodes; - “ M
” - the presence of metastases - additional foci of the disease in other areas of the body.
Using " G"
"indicate:
- The degree of difference between tumor cells
and healthy ones is from 1 to 3. One is assigned to cells that are most similar to normal tissues, and 3 is assigned to highly altered cells; - The number of dividing cells
is from 1 to 3. The fewer there are, the lower the score. - Necrosis
: a score from 0 to 2 is given to determine the amount of dying tissue - the higher the number, the more there is.
Then the total number of points is calculated: G1 – from 2 to 3; G2 – from 4 to 5; G3 – from 6 to 8.
Stages:
1A
: the size of the sarcoma does not exceed 10 centimeters, the remaining tissues are healthy.
1B
: the tumor may be larger than 15cm, but its cells are very similar to normal, and other organs are not affected.
2
: the tumor is no more than 5cm in diameter, but is graded G2 or G3.
3A
: sarcoma from 5 to 10 cm, G2 or G3.
3B
: 10 to 15 cm, G2 or G3, but other tissues are healthy.
Or, if the tumor is located in the abdomen, any size of the main lesion and damage to the nearest lymph nodes. 4
: a tumor of any diameter and type G, which has damaged not only nearby lymph nodes, but also distant tissues, such as the lungs.
Treatment of soft tissue sarcoma
The fight against oncology is not an easy task, and requires the participation of not just one doctor, but a whole team of professionals.
The oncology department carries out all types of diagnostics and therapy of sarcomas using the most modern equipment. Our world-class specialists fully guide the patient and provide him with all the necessary assistance - quickly, efficiently, without queues or waste of time.
Each situation is unique and requires an individual approach and a combination of different techniques:
Surgery
, with which some tumors can be completely cured. The purpose of the operation is to remove the entire tumor and a certain amount of healthy tissue surrounding it - at least 1-2 centimeters, so that no altered cells remain in the human body. In the past, many patients with sarcomas on the arms and legs were treated with limb amputation. Today this method is rarely used, and only in some cases it is not possible to avoid this traumatic procedure. In addition, there are situations when, along with oncology, it is necessary to remove important nerves, muscles, bones and blood vessels.
Even if the disease has spread to distant parts of the body, such as the lungs or other organs, surgery can cure a person or prolong his life.
Radiation therapy
: Targeting the tumor with radioactive beams or particles is a key part of the fight against soft tissue sarcomas.
In most cases, this procedure is prescribed as an adjuvant
treatment after surgery.
With its help, specialists kill the altered cells remaining in the body and prevent the recurrence of the disease. Some patients require neoadjuvant
therapy, used before surgery to shrink the tumor and make it easier to remove. In addition, radiation can be used as a palliative - to relieve the symptoms of an advanced disease that cannot be cured.
There are several types of radiation therapy:
- classic external
, in which the effect occurs externally, through the skin; - intraoperative
, which involves irradiating tissue after tumor removal, before closing the wound; - brachytherapy - injection of small granules of radioactive material into areas damaged by sarcoma;
- and proton
therapy, which uses streams of protons instead of X-rays - positively charged particles precisely aimed at the changed cells.
Chemotherapy
– the use of special drugs that kill tumor cells.
They are injected into a vein or taken orally as tablets and reach all areas of the body. Thanks to this property, the method is effective even at advanced stages of the disease. Depending on the type and stage of sarcoma, this procedure can be prescribed as the main or auxiliary treatment - in addition to surgery, and combined with radiation therapy. Some patients require a special type of chemotherapy called isolated limb perfusion
. During this procedure, a specialist separates the blood circulation of the affected arm or leg from the rest of the body, after which it injects the active substances.
Targeted therapy
– drugs that attack only certain components of altered cells and cause minimal harm to healthy ones.
Pazopanib
(
Votrient
): Blocks several enzymes important for cell growth and survival—proteins that initiate or speed up the chemical reactions needed to copy genetic information. It can be used to treat advanced soft tissue sarcomas that have not responded to chemotherapy. It slows tumor progression and eases side effects in patients whose tumors cannot be treated with surgery.
Tazemetostat (Tazverik
): affects a protein that promotes the growth of some cancer cells. It is used for epithelioid sarcomasEpithelioid sarcomas typically damage tissue in the hands, forearms, feet, or legs of adolescents and young adults that cannot be removed by surgery.
Etiology and pathogenesis
The causes of soft tissue sarcomas have not been identified. Factors that increase the risk of developing this pathology:
- Paget's disease (ostosis deformans);
- Recklenhausen's disease (neurofibromatosis);
- Gardner's syndrome (diffuse polyposis of the colon);
- Werner's syndrome (multiple endocrine adenomtaosis);
- Taking anabolic steroids.
The clinical course of malignant soft tissue tumors is characterized by variability.
Common signs of soft tissue sarcomas include frequent local relapses. Why do sarcomas often recur? This is explained by the following reasons:
- Lack of true capsule;
- Tendency to infiltrative growth;
- Multicentric growth.
Treatment of soft tissue sarcoma by stages
At each stage of the disease, certain methods of therapy are used:
Stage 1
: Small tumors of the extremities are removed through surgery, followed by radiation therapy if necessary. If the sarcoma is located in other areas of the body - the head, neck or abdomen, radiation or chemotherapy is prescribed before the intervention to reduce the size of the tumor.
Stages 2 and 3
: also treated surgically, in rare cases amputation of the damaged limb is performed. Chemotherapy and radiation therapy may be prescribed before and after the procedure.
Stage 4
: Rarely can be completely cured. The highest chances of recovery are in patients whose tumors - primary and secondary - can be removed during surgery. If this is not possible, targeted, chemotherapy and radiation therapy are prescribed to reduce the symptoms of the disease, prolong life or improve its quality.
Rehabilitation
Rehabilitation measures after the surgical stage of treatment depend on the volume and type of intervention. The principles, duration and outcomes of rehabilitation largely depend on the latter.
To achieve maximum functional results, it is necessary to follow the basic principles of rehabilitation
- Gradually increase the intensity of exercises on the surgical area.
- Maintain regular exercise.
- You should perform restorative exercises aimed at the entire body.
Rehabilitation activities are divided into several stages, including:
- The first (early) period begins immediately after surgery, after removal of the drainage system. As a rule, this is the second and third day after surgery. The main goal is to ensure that the exercises are aimed at minimizing the load in the area of surgical intervention, while maximizing the range of motion in the joint without stressing the muscle and bone structures.
- The second period involves a gradual increase in muscle activity.
- The third period is aimed at increasing muscle mass.
During surgical interventions on the lower extremities, all stages of rehabilitation should alternate with regular walking with a gradual increase in load. The first steps should be taken with the help of a walker, on crutches, with a stick and then without support.
Prognosis and survival of soft tissue sarcoma
Each person's outlook is different and depends on a variety of factors, such as age, general health, type of disease, stage, location of the tumor, and response to treatment.
To present approximate forecasts, doctors use a special term - “five-year survival rate”. This statistic says nothing about a person's chances - it only shows the percentage of people still alive 5 or more years after diagnosis.
For soft tissue sarcoma the numbers look like this:
- at localized stages, before the tumor has time to spread beyond the area in which it first appeared: approximately 81%;
- at regional stages, with damage to nearby tissues or nearby lymph nodes: about 56%;
- when the disease spreads to distant parts of the body such as the lungs: 15%.
When the disease is advanced, the following signs come to the fore:
• purple color of the affected area; • expansion of veins; • increased bleeding from wounds.
In almost all cases, soft tissue sarcoma metastasizes hematogenously. Metastases usually affect liver and lung tissues. The rate of progression of the pathology depends on the type of cancer lesion, although according to the standard the disease develops quite quickly. The development of cancer pathology leads to increased pain. The greatest pain occurs when vessels, bones, joint cavities, and nerve trunks are affected. The most painful are sarcomas that form near bone tissue and nerve endings. The pain intensifies at night and during physical activity. loads